Corrector for Treating Class II, Division 1 and 2: Simple, Durable, Comfortable, and Effective
Machine translation
Original article is written in ES language (link to read it) .
Orthodontic Considerations
Class II malocclusions represent a high percentage in our daily orthodontic practice, hence the great diversity of therapies for each particular case, whether to limit, redirect maxillary growth, stimulate mandibular growth, or distal the upper posterior dentition; the clinician's decision to use a removable orthopedic appliance, fixed intermaxillary, elastics, extractions, non-extractions, or surgery leads us to consider fixed intermaxillary correctors as a viable alternative in patients who are growing or in second treatments where class II dental persists (young adults).
We have worked for over 10 years, using the first ForsusTM nitinol plate, later the ForsusTM with insertion pins, and currently the ForsusTM with an EZ2 module, the latter improved, which facilitates its quick and easy insertion for the clinician, and we have found that it is:
• Simple
Because it does not require a specific laboratory working time, its design allows for placement in the same appointment as the patient.
• Comfortable
Its small size allows the patient to perform all oral functions, it is not bothersome, requires little cooperation from the patient, and facilitates oral hygiene.
• Durable
The ForsusTM is designed to withstand the fatigue generated by prolonged mouth opening and closing and does not lose its strength generated by the compression of the spring.
• Effective
The force it generates (8 ounces = approximately 227 grams per side) is constant throughout the 24 hours of the day, making the orthopedic and orthodontic result we require predictable.
The ForsusTM FRD meets the requirements of any class II corrector, as it has a telescopic component that acts as a piston within the spring.
Below is a guide for you to choose the ideal corrector for your patient, and clinical intraoral aspects are illustrated.
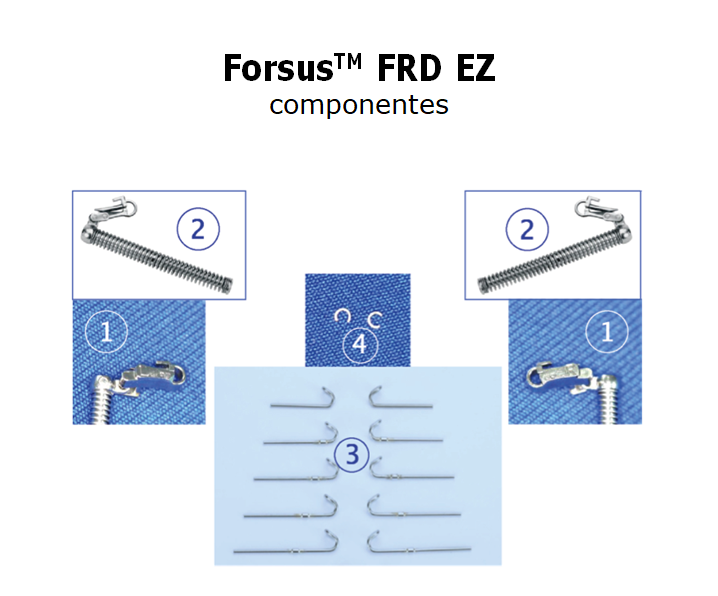
- Right and left EZ2 insertion module.
- Universal telescopic spring.
- Pusher stem or piston.
- C-shaped closing or crimpable stops.
Selection of the ForsusTM FRD size
The millimeter ruler is placed distal to the upper occlusal tube of 6s, in the central area between the canine and lower premolar, the line that remains in this area is the correct measurement of the ForsusTM piston, in addition, bands with an extraoral arch tube should be cemented towards occlusal and palatal boxes should be placed so that at the end of the mechanics the intraoral anchorage (palatal bar or Nance button) is inserted.

Steps to Insert the ForsusTM FRD
- Using a Weingart plier, insert the universal spring module from mesial to distal into the occlusal tube of the extraoral arch of the first molar band.
- Check that it is well inserted.
- Insert the pusher or piston into the spring.
- Bring the mesial end of the piston to the lower rectangular Nitinol or steel main arch, between the canine and the first premolar, turning it occlusally.
- Completely close the omega of the piston to prevent it from dislodging during the function of mouth opening and closing, and check that during mouth closure, it does not disturb or interfere with the compression of the spring, as well as during maximum mouth opening, the same steps for the opposite side.


Clinical Aspects
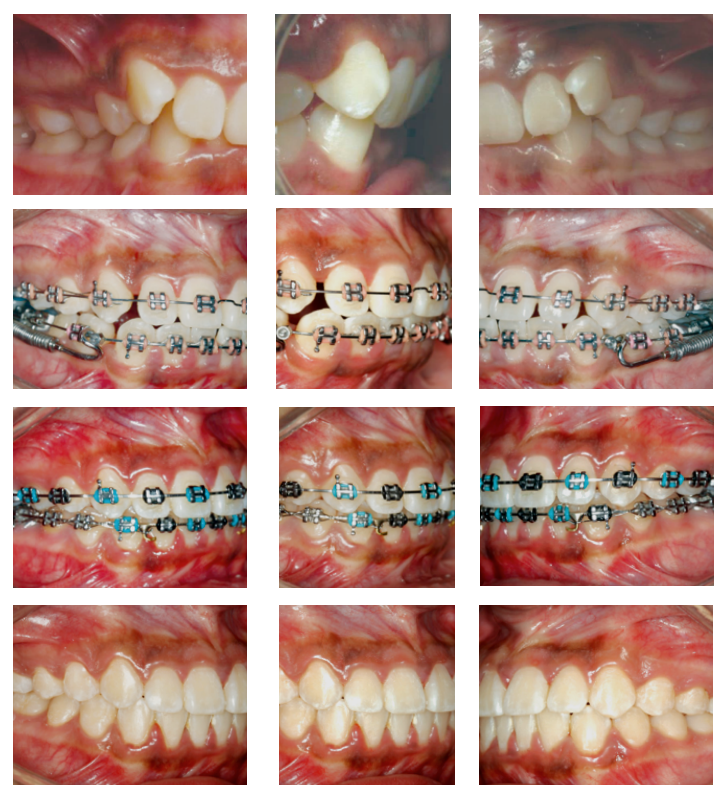
Intraoral clinical aspect 1:
Class II malocclusion, Division 1 in growth (13 years) MBT bracket system, Gemini 0.022”, ForsusTM FRD EZ2.

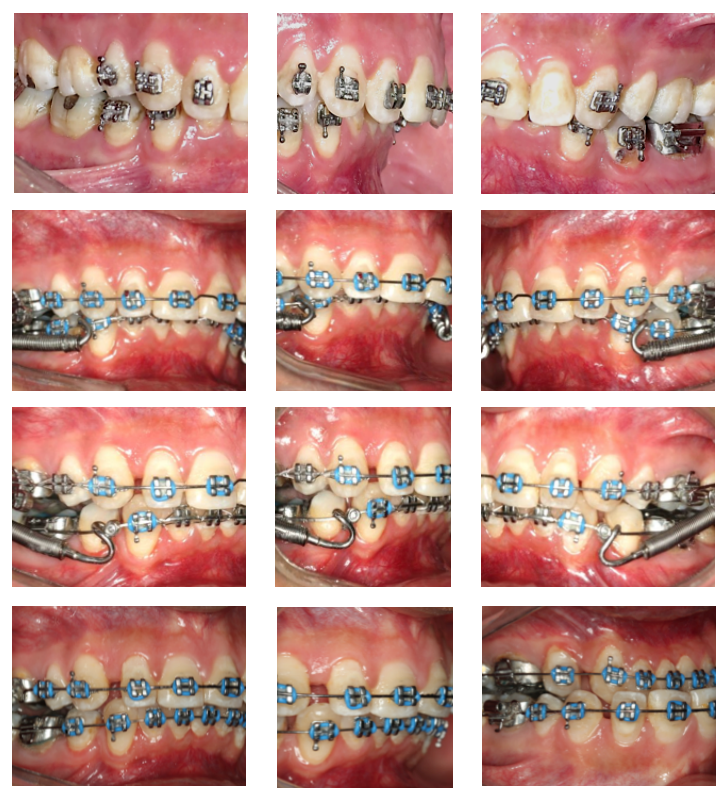
Intraoral clinical aspect 2:
Class II malocclusion, Division 2 in growth (12 years) MBT Gemini 0.022” bracket system, ForsusTM FRD EZ2.
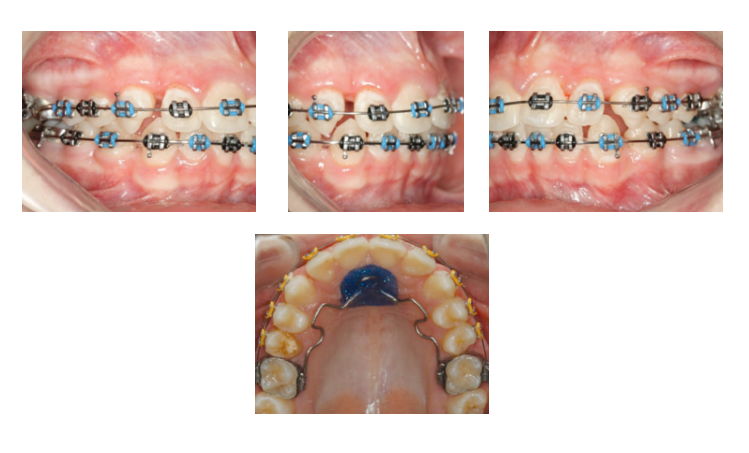
Intraoral clinical aspect 3:
Class II dental malocclusion, second orthodontic management, without growth (26 years), MBT Gemini 0.022” bracket system.
Disengagement of the ForsusTM FRD EZ2
With an angled and thin Weingart pliers, grasp between the insert and the universal spring and with a downward and mesial motion, the insert is dislodged.

Intraoral anchorage:
The anchorage at the end of the use of the ForsusTM, whether a palatal bar, nance button, or continuous 0.020” steel or Australian arch with a mesial stop just at the main tube, is highly recommended for 3-4 appointments to maintain our results and continue with the biomechanics of each case.
Conclusions
The ForsusTM FRD fixed Class II intermaxillary corrector offers us a safe and effective alternative to address the issues that arise in our clinical practice, recommended for use in growing patients or where other removable orthodontic appliances have failed due to lack of patient cooperation.
Bibliography:
- Lorenzo F, Lisa A, Veronica G, Caterina M, Efisio D and Tiziano B. Effectiveness of comprehensive fixed appliance treatment used with the Forsus Fatigue Resistant Device in Class II patients; Angle Orthod. 2011; 81:678-683.
- William V. The Forsus Fatigue Resistant Device; Journal Clinic Orthodontics, June 2006; 368-76.
- Belma I, Ebru K, Cagri T, and Mufide D. Treatment effects of the Forsus Fatigue Resistant Device used with miniscrew anchorage; Angle Orthod. 2014; 84: 76-87.
- Graham J, Peter H B, Ki B and Donald R. Class II Non-Extraction Patients Treated with the Forsus Fatigue Resistant Device Versus Intermaxillary Elastics; Angle Orthod. 2008; 78:332-38.
- Amy C, Humam S, Carlos F, Brian P And Sawsan T. Patient experiences with the Forsus Fatigue Resistant Device; Angle Orthod. 2013; 83:437-446.
- Fonseca B F. Simple and effective biomechanics in orthodontics. 1st ed., Venezuela: Editorial Amolca; Year 2016.