
Compensatory Treatment of Class III Dentoalveolar Malocclusion with Mini Screws in the Mandibular Notch
Machine translation
Original article is written in ES language (link to read it) .
Summary
Introduction: mini screws in orthodontics have revolutionized mechanics in orthodontics, improving orthodontic outcomes and controlling the 3rd Law of Newton.
Clinical case: 16-year-old male patient in growth, with no pathological data reported.
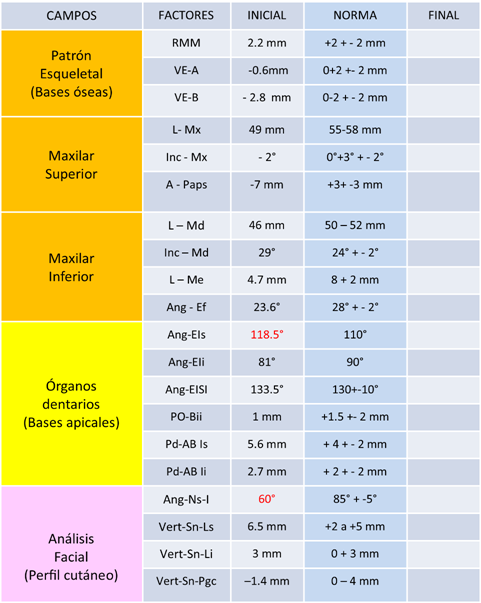
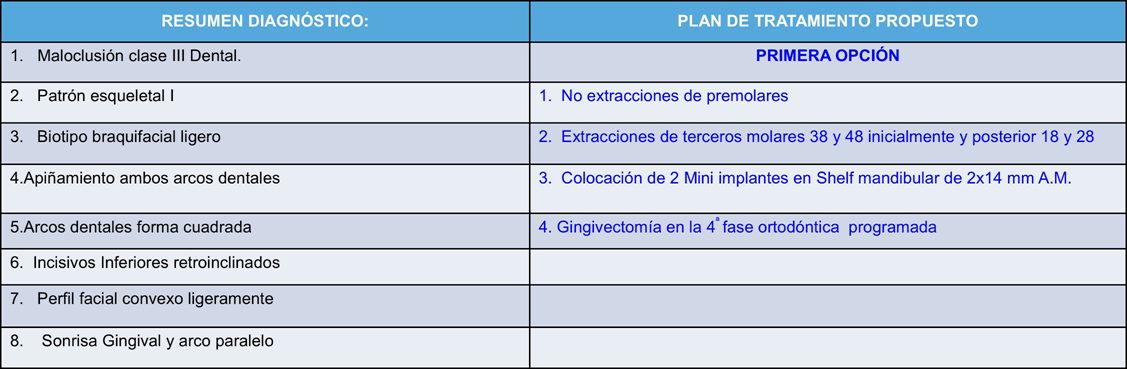
Diagnosis: class III dentoalveolar malocclusion, skeletal pattern I, retroclined lower incisors, slight brachyfacial biotype, convex facial profile, gingival smile, and does not present mutually protected occlusion.
Treatment plan: a conservative class III compensation treatment was proposed to the patient's parents, the placement of 2 mini screws of 2X14 mm medical steel in the mandibular notch and gingivectomy before completing the treatment to improve smile height and aesthetics.
Results: all orthodontic objectives of Class I molar and canine, correct horizontal and vertical overbite, improvement of the gingival smile, achievement of mutually protected occlusion, improvement in the final position of lower incisors, and softening of the patient's facial profile were achieved.
Introduction
According to the World Health Organization (WHO), malocclusions rank third in prevalence among pathologies affecting oral health, following dental caries and periodontal disease. Individuals with class III malocclusion may present combinations of skeletal and dentoalveolar characteristics, which is considered to be of multifactorial etiology.
In orthodontics, anchorage control is a critical consideration when diagnosing and establishing the treatment plan for patients with dental and skeletal malocclusions.
Orthodontic anchorage is defined as the resistance to unwanted dental movement; traditionally, anchorage is divided into: free, moderate, maximum, and absolute or skeletal, the latter having gained prominence in recent years with the use of mini screws and mini plates.
Currently, there is a wide range of interradicular and extra-alveolar mini screws ranging from 1.0 mm to 2.3 mm in diameter and from 4 mm to 21 mm in length. Extra-alveolar mini screws in the mandibular notch are reliable for retracting the entire mandibular dental arch, correcting severe anterior crowding skeletally, protrusion, and performing treatment without extraction therapy or orthognathic surgery.
In orthodontics, maximum or absolute anchorage is sometimes required, that is, a high resistance to displacement, so that if a force is applied to a tooth, we will always have movements in the opposite direction that are sometimes undesirable, or we move pieces that we do not want to move. For this reason, the different types of anchorage have been widely used throughout the history of orthodontics.
Extraoral mini-screws have caused a renaissance in the field of orthodontics with their concept of absolute anchorage; it is a mechanics that, in the hands of an experienced orthodontist, can overcome clinical challenges and turn borderline surgical cases into non-surgical ones, without compromising the results obtained; however, the selection of cases remains the key to clinical success.
The use of mini-screws in the mandibular notch allows the entire mandibular dentition to retract as a block, since the mini implants are located outside the line of action of the roots and therefore do not interfere with the movement of the entire dental arch.
Micro implants aim to generate absolute anchorage; their stability is multifactorial and mainly depends on the type of implant, length, diameter, placement position, and the area where it will be inserted.
Mini implants are a good alternative for generating absolute anchorage; they allow movements in the three-dimensional space while remaining immobile. A longer and wider mini implant will have better primary stability than one with a smaller diameter, but it will also depend on whether it is placed in the mandible or maxilla, as the bone tissue has different characteristics.
The bone thickness of the mandibular shelf was found to be greatest between the first and second molars, buccally, where there is the greatest thickness of the cortical bone; therefore, it is an optimal site for the placement of the mini implant.
The refinement and introduction of temporary intraoral anchorage devices in the early 21st century had a significant impact on contemporary orthodontics. Undoubtedly, their use has greatly improved, and among the advantages, the reduction of time to correct side effects, the ability to withstand a variety of orthodontic loads for absolute anchorage, ease of placement and removal, low cost, and the possibility of immediate activation stand out. All these crucial advantages have provided confidence in the use of micro implants.
There are also some limiting factors like any other anchorage reinforcement technique related to mini screws that must be considered before clinical application, where the loss of stability of these devices is the main issue. Orthodontic micro-screws tend to have a failure rate of around 10% to 30%.
Clinical Case
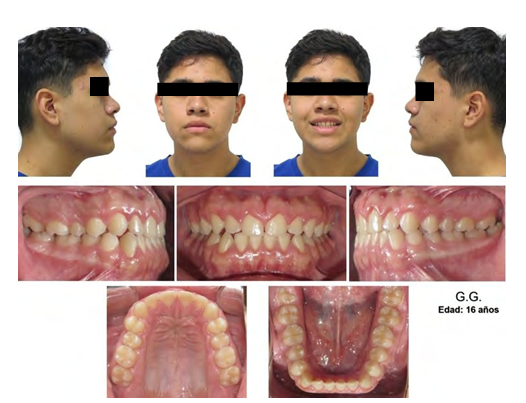
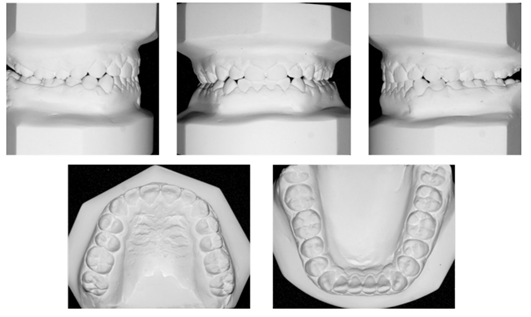
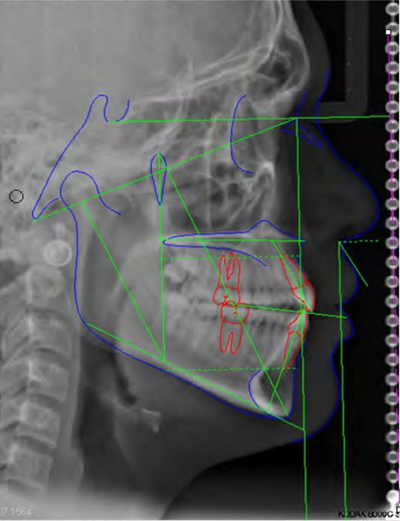
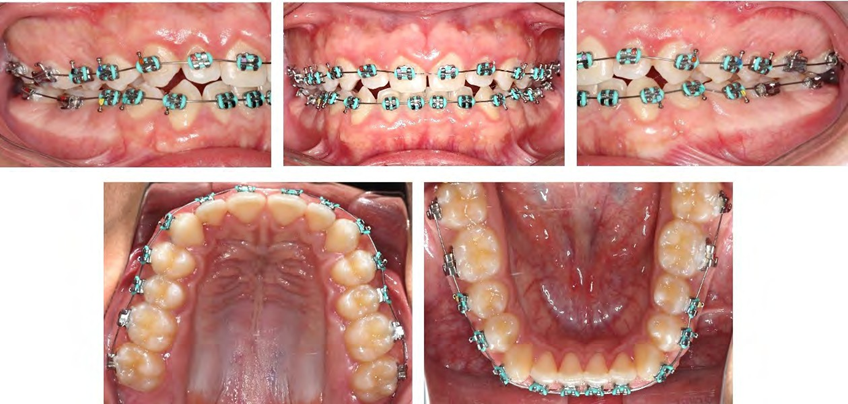
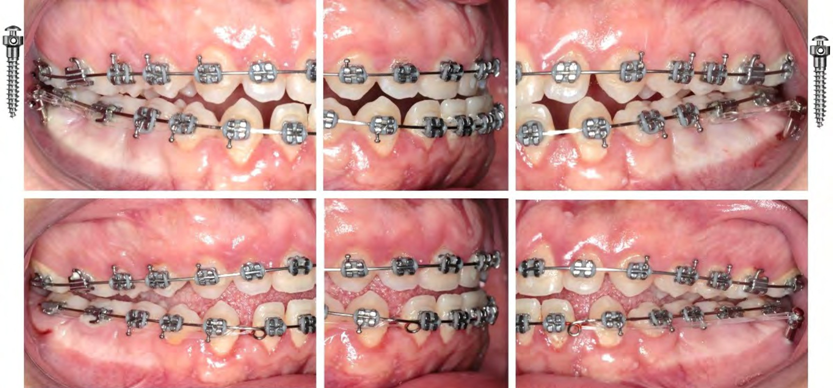
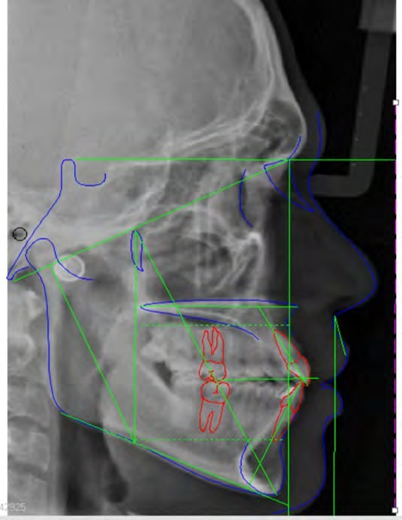
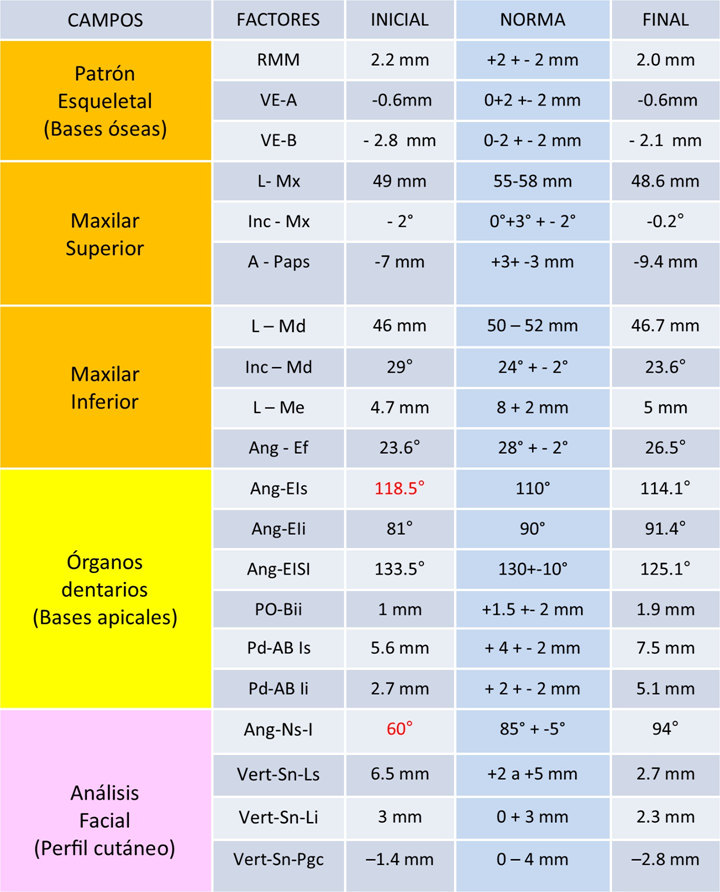
16-year-old male patient, in growth, presents class III molar and canine malocclusion, skeletal pattern I, retroclined incisors, decreased vertical and horizontal overbite, convex facial profile, gingival smile, and does not present mutually protected occlusion. (Figure 1-7, Table 1).
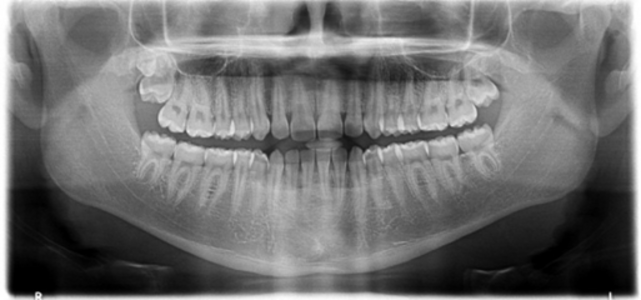
In the progress orthopantomography, the extractions of dental organ (do) 38 and 48 are observed, which were necessary to perform for the placement of the 2 mini-screws 2x14 mm of Medical Steel. (Figure 8).

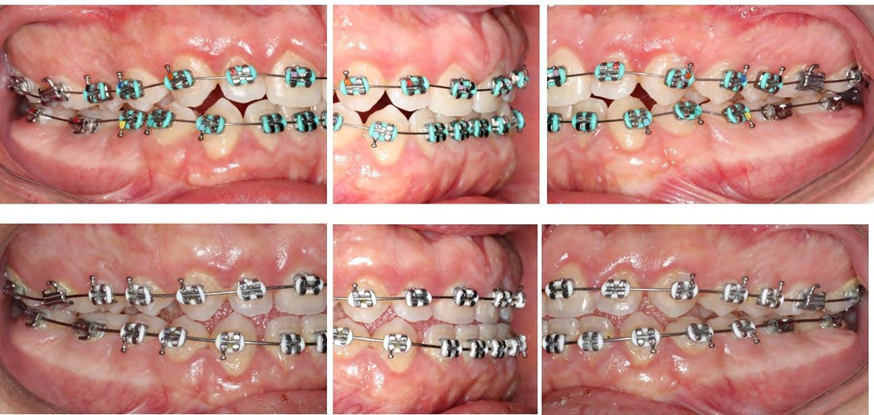
In the second orthodontic phase, 2 mini-screws were placed in the mandibular notch, leveling of tubes and brackets, which allow for good distal movement of the posterior tooth group in a time frame of 5 months, closing spaces with 1 double helix arch 0.020”. (Figure 9).
Subsequently, space closure was performed with arches using 0.019x0.025” steel posts and type 1 upper and type 3 lower ligatures. (Figure 10).
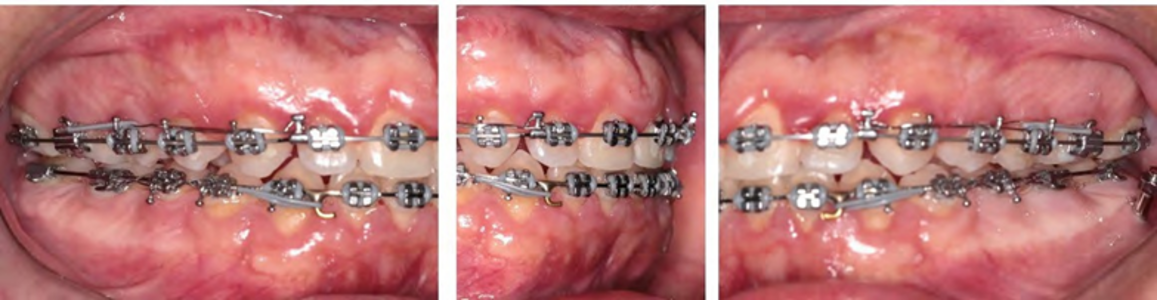
The use of elastics allows us to improve the posterior occlusal settlement. (Figure 11).
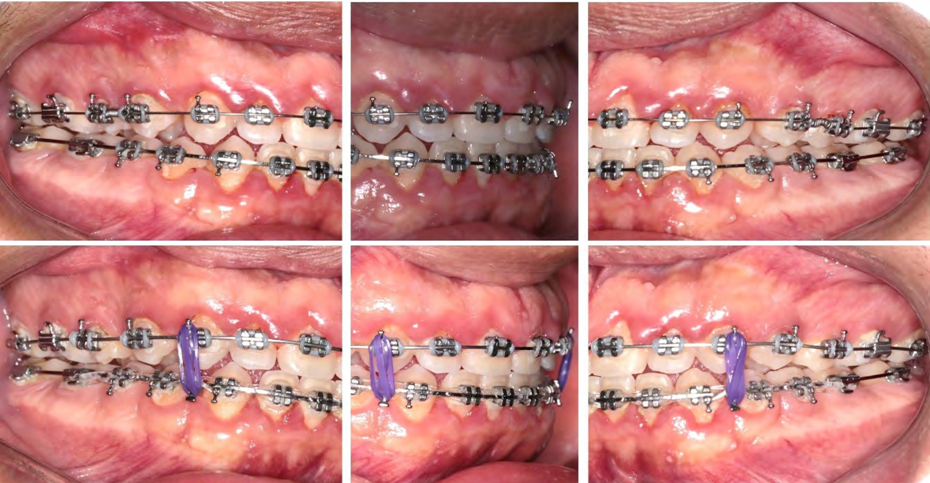
The patient underwent a gingivectomy in the upper dental arch from tooth 14 to 24 to improve the aesthetics of their smile. (Figure 12).

Results
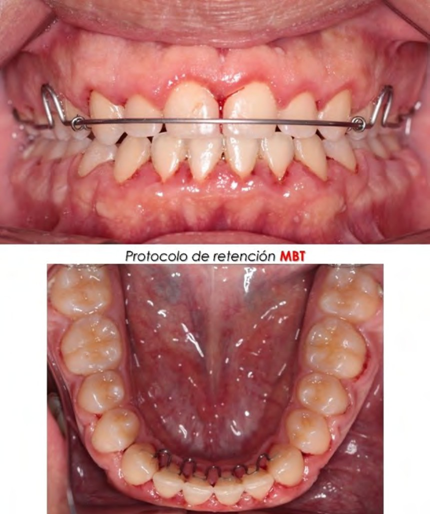
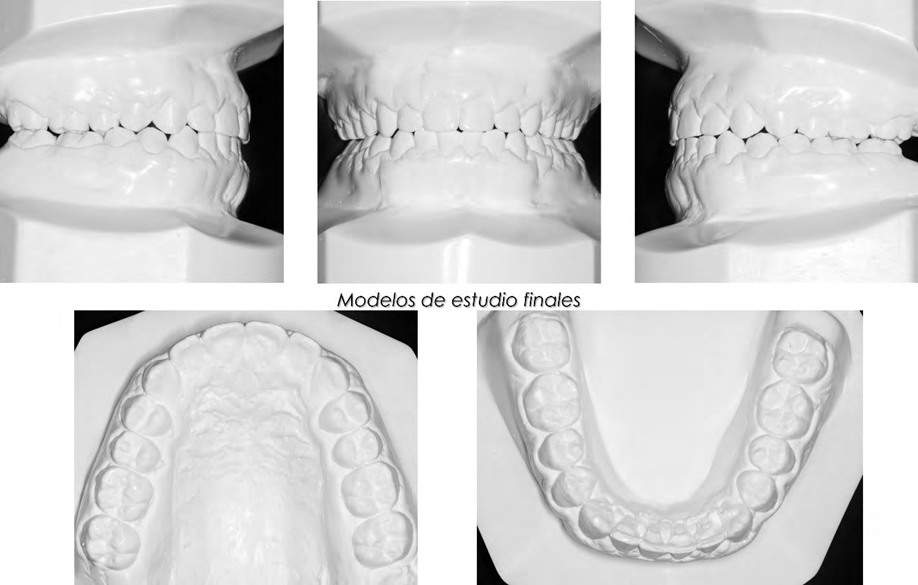
All orthodontic objectives of Class I molar and canine, correct horizontal and vertical overbite, improvement of the gingival smile, achievement of mutually protected occlusion, improvement in the final position of lower incisors, and smoothing of the patient's facial profile were achieved. (Figure 13-17, Table 2)


Discussion
The results obtained coincide with those reported by Chang C. et al. where mini screws in the mandibular notch are a reliable solution to move the entire mandibular dental arch to correct dental class III protrusion and malocclusion and to perform treatment without premolar extractions or orthognathic surgery.
Mini screws are attachments that allow for absolute or skeletal anchorage when orthodontic treatment requires it, as observed in the present clinical case, where the entire lower dental arch was moved distally as reported by Benavides Ch. S.
Without a doubt, extraoral mini screws have caused a renaissance in the field of orthodontics with their concept of absolute or bony anchorage in the last decade; it is an added mechanics to overcome new clinical challenges and convert borderline surgical cases to non-surgical ones as reported by Ghosh A.
Authors: Fonseca Balcázar Franco, Fonseca Esparza Khiabet, Fonseca Esparza Franco
References:
- Telley Millán M, Katagiri Katagiri M, Pérez Tejada HE. Case study of Class I, Class II, and Class III malocclusions according to Angle in the Orthodontics Department of UNAM. Mexican Dental Journal. 2007;11(4).
- Awuapara Flores S, Cerro Temoche AH, Meneses López A. Miniscrews: tomographic-anatomic evidence. Rev estomatol Hered. 2008;18(2).
- Baumgaertel S, Razavi MR, Hans MG. Mini-implant anchorage for the orthodontic practitioner. American Journal of Orthodontics and Dentofacial Orthopedics. 2008;133(4).
- Chang C, Liu SSY, Roberts WE. Primary failure rate for 1680 extra-alveolar mandibular buccal shelf mini-screws placed in movable mucosa or attached gingiva. Angle Orthodontist. 2015;85(6).
- Benavides Chaverri S, Cruz López P, Chang Valverde M. Microimplants, a new option in orthodontic treatment. Vital Dentistry. 2016;2(25).
- Ghosh A. Infra-Zygomatic Crest and Buccal Shelf - Orthodontic Bone Screws: A Leap Ahead of Micro-Implants – Clinical Perspectives. Journal of Indian Orthodontic Society. 2018;52(4_suppl2).
- Almeida MR. Biomechanics of extra-alveolar mini-implants. Dental Press J Orthod. 2019;24(4).
- Fritz M, Doron Y, Álvarez E, Angela R. Characteristics of the areas designated for the use of mini implants measured through Cone Beam computed tomography. Latin American Journal of Orthodontics and Pediatric Dentistry [Internet]. 2022 [cited 2024 Feb 22]; Available from: https://www.ortodoncia.ws/publicaciones/ 2022/art-59/
- Ochoa J, Peralta P, Rojas M, Rouillon J, León B. Stability of micro-screws in orthodontics. Ecuadorian Journal of Science, Technology, and Innovation in Public Health. 2022;54–9.