Application of the Jigger FF in the correction of Class II malocclusions
Machine translation
Original article is written in ES language (link to read it) .
Summary
The purpose of the study is to present a new device, referred to by the author as Jigger FF, which is made with 0.028” diameter round stainless steel wire, open nitinol spring of 0.032” diameter, light intermaxillary elastics of 3/16” diameter and 2½ ounces of force. Its fabrication is quick, versatile, and reduces treatment costs, requiring little cooperation from the patient, who needs to accept it and limit care to changing the light elastics, with greater directional control of the forces, comfort, and freedom of mouth opening and closing.
Its main biomechanical functions are two: 1) To derotate molars that condition a class II molar relationship; and 2) To distalize molars unilaterally or bilaterally, with results from the first function obtained within 8-12 weeks and the second function requiring approximately 12-20 weeks.
Conclusions. The results obtained are excellent, derotating molars and achieving class I sagittal relationships in less time; the distalization of molars is effective, requiring a longer period and distalizing 4 to 6 mm, which can be done unilaterally, which is frequently the case, or bilaterally in those cases where the patient's facial profile is not compromised.
Introduction
In the 1950s, a new approach to the treatment of dental malocclusions began when Kloen and Ricketts demonstrated the effects of applying extraoral forces on the upper dentition and the maxilla.
The typical biomechanics for correcting Class II malocclusion has been the extraoral arch, to delay the anterior growth of the upper maxilla or to distalize the upper teeth with high, medium, or low extraoral support.
Another approach has been the use of functional appliances such as: the Andreasen activator 1908, Balters' Bionator 1960, Frankel regulator, all of which generate a pushing force vector; the first two are tooth-supported and the last one is mucosa-supported. All are force transmitters that originate from muscular action and affect the dentition, their biomechanical design provokes muscular reaction, modifying the level of postural mandibular muscle activity.
It is well known to every clinician that the same mechanotherapy cannot be used for all patients with class II malocclusion; a variety is needed along with precise knowledge of each one to achieve the expected results.
Mechanics have proliferated, always seeking greater effectiveness in correcting this malocclusion, and we find in the wide market of orthodontic commercial houses bimaxillary appliances such as Herbs, Jasper-jumper, Twin Force Corrector, Sabbagh, Forsus Nitinol Plane, Forsus Fred, among others, and unimaxillary appliances such as Wilson's Bimetric Arch, Jones-Jig, Lockar distalizer, sectional or continuous thermal arch, all with the ultimate goal of molar distalization.
In this work, a versatile, practical appliance that reduces costs in orthodontic clinical practice was used.
- Installation procedure. The placement of the appliance is recommended once the first phase of orthodontic treatment (dental leveling and alignment) is completed. The Jigger FF appliance was placed in the upper dental arch between the canine and first premolar in the mesial part, and between the second premolar and molar in the distal part. The open nitinol spring without compression should be positioned between the distal part of the appliance and the molar, with a continuous round stainless steel wire of 0.016” gauge in a 0.018” slot and 0.018” gauge in a 0.022” slot (Figures 1, 2, and 3).



- Use. Its recommendation is for class II dentoalveolar malocclusions, unilaterally or bilaterally, in growing patients or adults, without joint dysfunction issues, who are cooperative for changing light elastics daily.
Case Description
- Case 1. Unilateral molar distalization. This is a 23-year-old female patient, with a previous orthodontic treatment, a class I right molar relationship and a class II left molar relationship, with agenesis of O.D. 22, her cephalometric values are within normal range, her facial profile is slightly convex, with a Normofacial Biotype (VERT of 0), her upper dental midline deviated to the left by 3 mm, the reason for the consultation is to improve the molar and canine relationship on the left side.
Fixed orthodontic MBT 0.022” appliances are placed, the results are shown in figure 4.
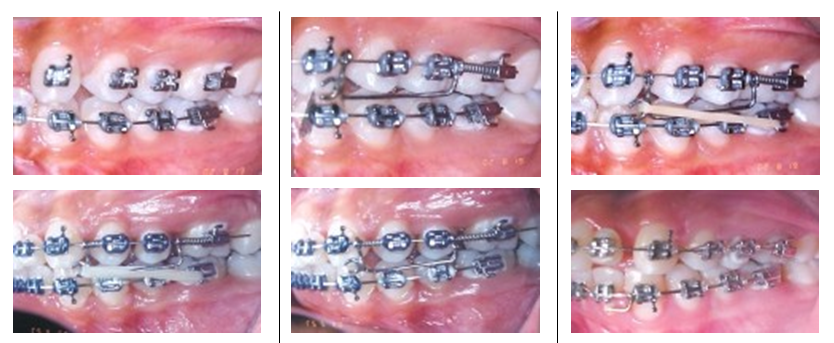
- Case 2. Bilateral molar distalization. A 21-year-old female patient, with a diagnostic summary of skeletal class I, bilateral class II molar relationship, slight crowding, convex facial profile, normofacial biotype with a VERT of +3, her management begins with fixed orthodontic appliances MBT 0.022”, after the first phase of treatment is completed, a round steel arch of 0.018” is placed along with two bilateral Jiggers with Niti spring and light elastics of 3/16 and 2½ ounces of force for the first two months, and for the next two months, the force is doubled, the results are shown in figure 5.

Discussion
In the first case, distalization is effective in correcting the molar class II to class I, obtaining space that allows us to correct the class II canine relationship, generating sufficient space for the placement of the missing O. D. 22 implant.
- Case 2. The results are excellent, achieving the correction of class II molar and canine, reducing maxillary dental protrusion, obtaining a correct overbite and overjet. One of the aspects that must be taken care of in this mechanics is the retention until the end of the treatment once molar distalization has been achieved, the bite opening is controlled by making the mesial part of the Jigger lower than the distal part so that the force vector of the elastics is horizontal and not vertical.
Bibliographic References
- Canut BJA. Clinical orthodontics. 2nd Edition. Mexico City: Editorial Salvat; 1992.
- Thomas G, Rakosi M, Petrovic. Dentofacial orthopedics with functional appliances. 2nd Edition, Spain: Editorial Harcourt; 1998.
- Rakosi T, Irmtrud J. Atlas of maxillary orthopedics: Diagnosis. Spain: Editorial Ediciones Científicas y Técnicas; 1992.
- Villavicencio J, Fernández y Magaña AL. Dentofacial orthopedics. 1st Edition. Caracas, Venezuela: Editorial Actualidades Médico-Odontológicas Latinoamericana, C.A.; 1996.
- Nanda Ravindra. Biomechanics in clinical orthodontics. 1st Edition. Buenos Aires, Argentina: Editorial Panamericana; 1998.
- Graber MT, Vanarsdall LR. Orthodontics, general principles and techniques. 2nd Edition. Editorial Panamericana; 1999.
- Wilson LW, Wilson CR. Multi-directional 3D Functional Class II Treatment. JCO 1987: 186-9.
- Gianelly AA, Bednar J, Dietz US. Japanese niticoil used to move - molars distally. Am J Orthod ODF 1991; 99: 564-6.
- Jones DR, White JM. Rapid Class II molar correction with an open-coil jig. JCO 1992; Vol. XXVI.
- Gianelly AA. Distal movement of the maxillary molars. AJODO 1988; 144: 66-72.