Protocol for Indirect Restoration Intraoral Scanning Under Dental Dam Isolation: A Dental Technique
Abstract
This paper aims to describe an intraoral scanning protocol for indirect restorations utilizing dental dam isolation. This technique consists of the initial scan of both arches and their occlusion. Then, after necessary dental preparation is performed under isolation with a dental dam, intraoral scanning of preparations is performed, maintaining the dental dam in place. The proposed protocol shortens the operative time minimizing clinical factors that can affect the scan accuracy and maximizing preparation margins’ visibility, ensuring a stress-free environment. This method can be applied for chair-side dentistry and conventional workflow for sending scans to the laboratory technician.
Digital systems are becoming very common in dentistry. Among the recent advancements in computer-aided design and computer-aided manufacturing (CAD/CAM), intraoral scanning has been successfully integrated into clinical dentistry. The advantages of a digital workflow include time efficiency, reliability, repeatability, and overall increased treatment quality. Digital scanning techniques are a clinically acceptable alternative to conventional impression making for unitary and short-span teeth and implant-supported fixed prosthesis.
More digital protocols of total rehabilitation you can find in our course "Indirect restoration in the biomimetic concept".
The light scanning process is based on capturing the reflected light that has been previously emitted on the tooth surface. Several factors may influence scanning accuracy, such as the scanner selected, surface characteristics to scan, the calibration, handling, learning, scanning protocols, and scanning conditions. Several clinical factors such as moisture, saliva, blood, and optics’ fogging may cause excessive light reflection that may reduce the quality and sharpness of the captured image. Tongue movement may wet the scanning surface and reduce the scan quality. As the moving mucosa, it may interrupt the scanner’s image stitching process, which together with a lack of defined and stable intraoral features to ensure rigid stitching may also distort the resulting scan. Limiting the impact of these conditions will improve the precision and trueness of digital scans.
Success in restorative treatments depends mainly on the effective control of moisture and microbes during the procedure. Although there is no robust evidence to favor the dental dam technique in improving restorations’ survival rate, this is the most used isolation method. The alternatives to dental dam offer only partial isolation and insufficient soft tissue retraction. Dental dam use is highly recommended in many dental procedures based on adhesion, such as immediate dentin sealing, build-up, and direct or indirect restoration placement. Clarity of operative field, moisture reduction, gingival retraction, isolation from saliva, blood, and tongue are ideal intraoral scanning requirements. The dental dam can help fulfill these requirements, so maintaining it when restorative treatment is finished while making the digital scan may be beneficial for scanning accuracy and time efficiency. This paper aims to describe a protocol for indirect restoration intraoral scanning under dental dam isolation.
Technique
Scan the arch to be treated and the antagonist dentition using an intraoral scanner (Medit i500, Medit corp., Seongbuk-gu, South Korea) (Fig 1A,B).
Scan the intermaxillary relationship in the desired treatment position (maximum intercuspation position (MIP), centric occlusion (CO) depending on the required treatment position. (Fig 1C)
Place the dental dam on the teeth to be treated. It is advisable to extend the isolation to at least 2 to 3 more teeth from those that require dental preparation.
Perform tooth build-up if needed, dental preparation, and immediate dentine sealing under dental dam isolation (Fig 2).
Duplicate the arch’s scan data to be treated and trim the tooth area to be prepared. It is recommended to extend the trimmed area only to the adjacent teeth contact points to guarantee more reference surface for matching the next scan (Fig 3A).
Scan intraorally the prepared teeth filling the previously trimmed scan. To facilitate the dental scan process, start the scanning from the broadest tooth reference available, and pull down the dental dam for complete clarity of the cervical and interproximal tooth surfaces. Available space for restoration can be checked with the scanner’s space evaluation tool. If insufficient, a rescan after further dental preparation will be needed. (Figs 3B,C, 4, and 5).
Export all scans aligned to the same XYZ spatial coordinates in standard tessellation language (STL) files.
Import STL files into CAD software (Exocad DentalCAD; Exocad) and design the indirect restorations. Afterward, fabricate the restorations with subtractive CAM from a lithium disilicate block (Amber Mill, Hass Bio corp., Gangwon-do, Korea) in a milling machine (DWX-42W, Roland, Irvine, CA) (Fig 6). Next, perform adhesive cementation of the indirect restorations under dental dam isolation with light cure luting cement (Enamel plus HRi, Micerium s.p.a., Avegno, Italy), following the restoration manufacturer’s recommendations. Finally, provide proper finishing and polishing (Figs 7 and 8).
 Figure 1 Preoperative intraoral scans with no dental dam. A, Maxillary scan. Occlusal view. B, Mandibular scan. Occlusal view. C, Intermaxillary scan in treatment position.
Figure 1 Preoperative intraoral scans with no dental dam. A, Maxillary scan. Occlusal view. B, Mandibular scan. Occlusal view. C, Intermaxillary scan in treatment position.
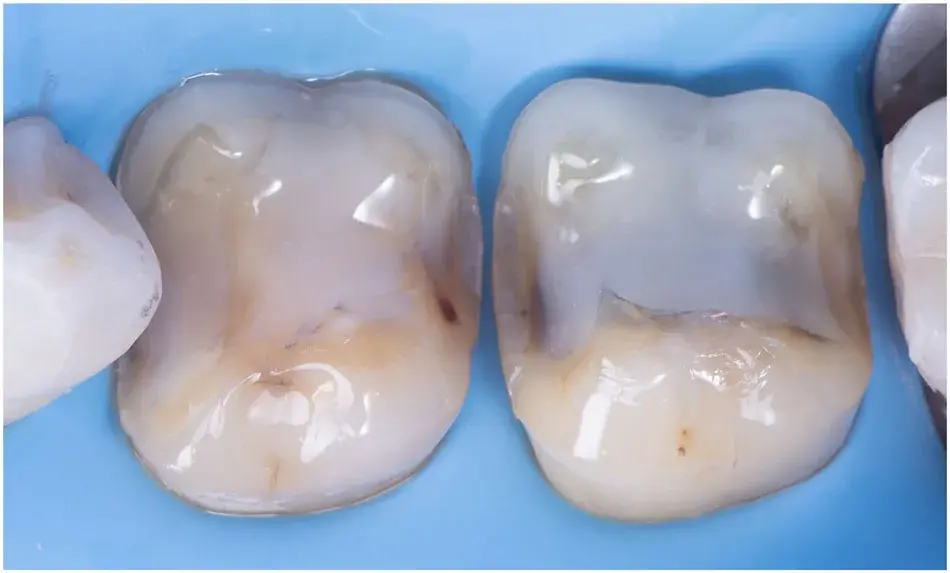 Figure 2 Dental preparation performed with dental dam isolation. Occlusal view.
Figure 2 Dental preparation performed with dental dam isolation. Occlusal view.
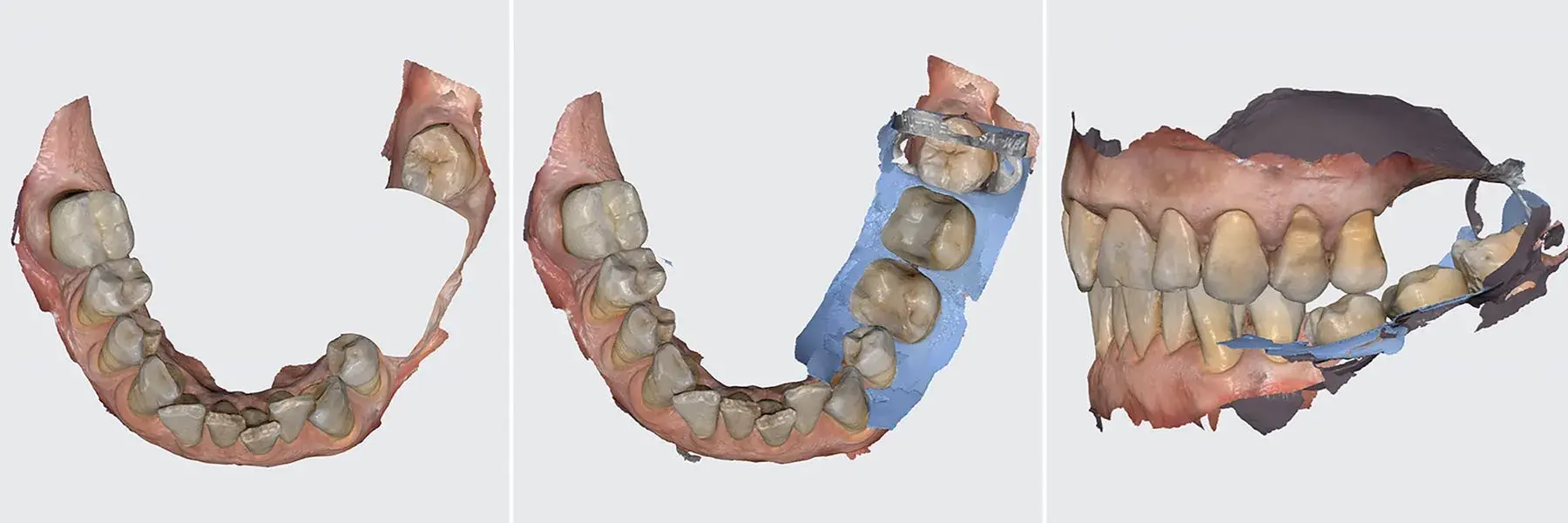 Figure 3 Postoperative intraoral scan. A, Duplicate of scan corresponding to arch be treated with area to be prepared trimmed. Occlusal view. B, IOS with dental dam isolation. Occlusal view. C, Postoperative scans aligned in treatment position
Figure 3 Postoperative intraoral scan. A, Duplicate of scan corresponding to arch be treated with area to be prepared trimmed. Occlusal view. B, IOS with dental dam isolation. Occlusal view. C, Postoperative scans aligned in treatment position
 Figure 4 Intraoral scan with dental dam isolation. Close up occlusal view.
Figure 4 Intraoral scan with dental dam isolation. Close up occlusal view.
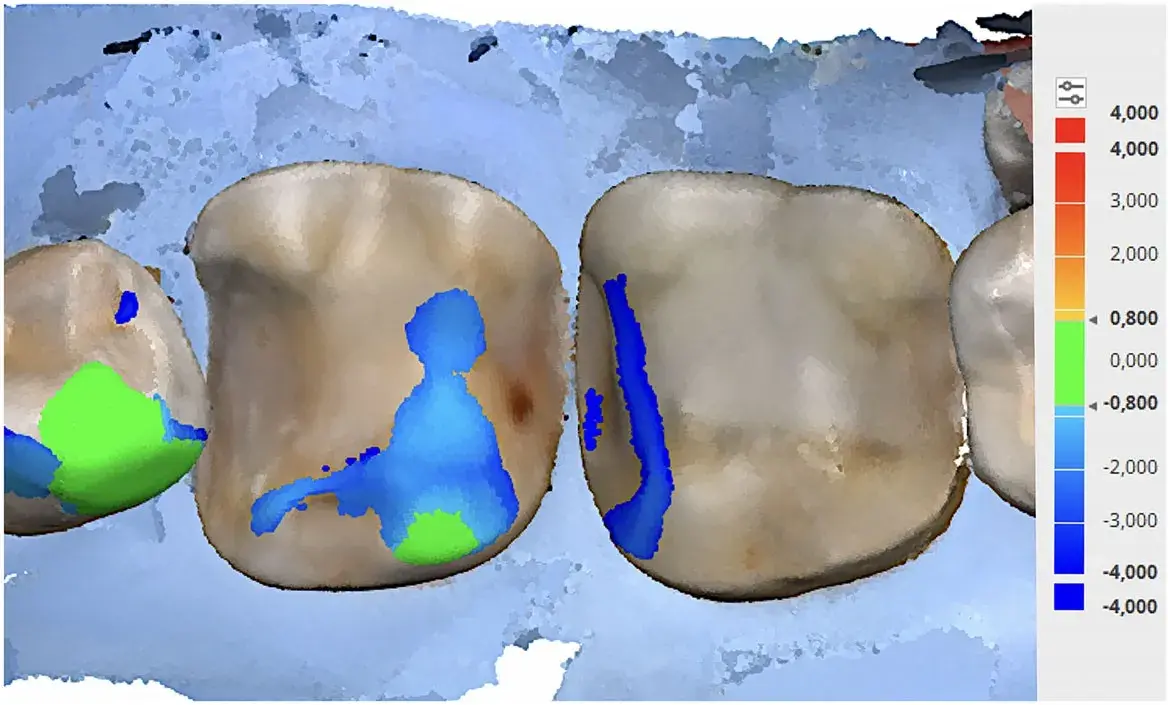 Figure 5 Clearance analysis of dental preparation. Occlusal view.
Figure 5 Clearance analysis of dental preparation. Occlusal view.
 Figure 6 Detail of indirect restorations made with subtractive computeraided manufacturing (CAM) from a lithium disilicate block.
Figure 6 Detail of indirect restorations made with subtractive computeraided manufacturing (CAM) from a lithium disilicate block.
 Figure 7 Final restoration cemented. Buccal view with dental dam isolation.
Figure 7 Final restoration cemented. Buccal view with dental dam isolation.
 Figure 8 Final restoration cemented. Occlusal-buccal view after dental dam removal.
Figure 8 Final restoration cemented. Occlusal-buccal view after dental dam removal.
Discussion
The technique described in this article offers several advantages in scanning error reduction and overall efficiency. The final scan of the prepared tooth is made after finishing the restorative procedure before removing the dental dam. Scanning with the dental dam in place allows an outmost control of some distortion factors, such as the presence of saliva and blood. It also minimizes the interruption of the scanner’s stitching process caused by tongue or soft tissue movement, resulting in quicker and higher quality scans. Scanning under dental dam isolation may shorten the operative time and maximize preparation margins’ visibility, providing a stress-free environment. A limiting factor of this technique is that preparation margins should be supragingival and always visible on the dental dam.
This protocol can be integrated into both chair-side and outsourced CAM digital workflows. Chair-side workflow may maximize the overall cost-effectiveness ratio of the indirect restoration treatment, allowing the final prosthesis delivery in a single appointment.18 In both situations, digital scan quality and sharpness are improved due to having controlled many distortion causes. This higher quality scan will allow a better marginal and internal fit of the final restoration.
There are additional information you can gain in our course.
Summary
A protocol for indirect restoration intraoral scanning under dental dam isolation has been described step-by-step. It allows an outstanding control of many scan distortion factors, such as moisture and saliva, resulting in high-quality sharp scans. The final scan is done when restorative procedures are finished before removing the dental dam.
Authors
Lucas Q. Caponi, DDS, MSc
Eduardo Flor, DDS, MSc
Jorge Ortega-Martínez, DDS, PhD
Oscar Figueras-Alvarez, DDS, PhD
References
Rekow ED: Digital dentistry: the new state of the art – is it disruptive or destructive? Dent Mater 2020;36:9-24
Duret F: Toward a new symbolism in the fabrication of prosthetic design. Cah Prothese 1985;13:65-71
Van Noort R: The future of dental devices is digital. Dent Mater 2012;28:3-12
Patzelt SB, Vonau S, Stampf S, et al: Assessing the feasibility and accuracy of digitizing edentulous jaws. J Am Dent Assoc 2013;144:914-920
Aragón ML, Pontes LF, Bichara LM, et al: Validity and reliability of intraoral scanners compared to conventional gypsum models measurements: a systematic review. Eur J Orthod 2016;38:429-434
Joda T, Zarone F, Ferrari M: The complete digital workflow in fixed prosthodontics: a systematic review. BMC Oral Health 2017;17:124-131
Medina-Sotomayor P, Pascual-Moscardó A, Camps I: Relationship between resolution and accuracy of four intraoral scanners in complete-arch impressions. J Clin Exp Dent 2018;10:e361-e366
Abduo J, Elseyoufi M: Accuracy of intraoral scanners: a systematic review of influencing factors. Eur J Prosthodont Restor Dent 2018;26:101-121
Lim JH, Park JM, Kim M, et al: Comparison of digital intraoral scanner reproducibility and image trueness considering repetitive experience. J Prosthet Dent 2018;119:225-232
Rutkunas V, Ge ¯ ciauskait ˇ e A, Jegelevi ˙ cius D, et al: Accuracy of digital implant impressions with intraoral scanners. A systematic review. Eur J Oral Implantol 2017;10 Suppl 1:101-120
Wang Y, Li C, Yuan H, et al: Rubber dam isolation for restorative treatment in dental patients. Cochrane Database Syst Rev 2016;9:CD009858
Browet S, Gerdolle D: Precision and security in restorative dentistry: the synergy of isolation and magnification. Int J Esthet Dent 2017;12:172-185
Magne P: Immediate dentin sealing: a fundamental procedure for indirect bonded restorations. J Esthet Restor Dent 2005;17:144-154
Magne P, Spreafico R: Deep margin elevation: a paradigm shift. Am J Esthet Dent 2012;2:86-96
Vandenberghe B: The digital patient – imaging science in dentistry. J Dent 2018;74:S21-S26
Schepke U, Meijer HJ, Kerdijk W, et al: Digital versus analog complete-arch impressions for single-unit premolar implant crowns: operating time and patient preference. J Prosthet Dent 2015;114:403-406
Su TS, Sun J: Comparison of marginal and internal fit of 3-unit ceramic fixed dental prostheses made with either a conventional or digital impression. J Prosthet Dent 2016;116:362-367
Blatz MB, Conejo J: The current state of chairside digital dentistry and materials. Dent Clin North Am 2019;63:175-197