Instrumentation and irrigation in endodontics
Endodontic treatment at the stage of preparing root canals for filling requires solving the following problems:
creation of a “carpet path”, passage of a canal;
establishing the length of the root canal;
sequential mechanical treatment and irrigation of the canal.
Learn more about this topic in the webinar Clinical Root Canal Treatment Strategy for Effective Irrigation .
Passing and establishing working length
Small hand files are preferable to use for the first passage of channels No. 6-15. Both K-Reamer and K-file will do.
The working length is the distance from the top of the cusp or the most elevated part of the tooth to the physiological narrowing. Establishing the working length is also an important stage of endodontic treatment, since its value is very variable.

Figure 1. Dental pulp.
Methods for determining working length:
physical, using an apex locator;
X-ray;
combined.
Apex location is based on the fact that tissues have a constant electrical resistance. The resistance of tooth tissue is higher than that of the mucous membrane or periodontal tissue, therefore the electrical circuit that occurs between the electrodes that are placed in the canal and on the lip is not closed until the file reaches the periodontal tissue.
The first generations of apex locators worked exclusively in dry and clean channels; their mechanism of action was based on the determination of direct current strength. More modern models of apex locators determine impedance using alternating currents of different frequencies. The lowest impedance is determined in the apex region, and the highest in the orifice region. The apex locator sets the area where the resistance drops. Not a single model of this device is capable of measuring the length of the canal, even if it is equipped with a millimeter scale.
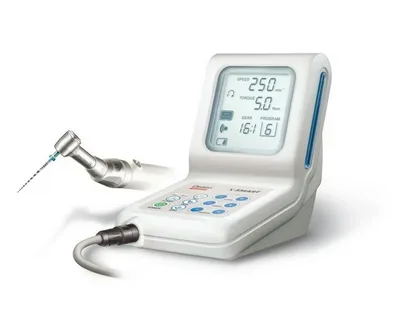
Figure 2. Apex locator.
Algorithm for measuring working length:
the instrument is inserted into the canal, not reaching 2 mm from the point established on the diagnostic radiograph;
confirmation of working length by physical method;
control radiograph.
Verification of the working length occurs when the instrument is located 0.5-2 mm from the radiographic apex and reaching the area of the apical constriction is confirmed by the apex locator data.
Root canal irrigation
Medicinal treatment of root canals is carried out with sodium hypochlorite and ethylenediaminetetraacetate (EDTA).
A 1% sodium hypochlorite solution is characterized by proteolytic properties and ensures the dissolution of pulp residues, organic components of dentin, frees the canal and simplifies its mechanical treatment. It also has a bactericidal effect and is capable of oxidizing pigments that appear during hemorrhages and pulp necrosis. Due to this, sodium hypochlorite has a lightening effect and is effectively used to correct discoloration of teeth.
The most universally accepted concentration of sodium hypochlorite is 3%; it is used by most manufacturers.
EDTA helps soften dentin to a depth of 50 microns on the canal walls by chelating calcium ions, which greatly simplifies machining. The use of EDTA is effective for getting rid of the smear layer, opening the dentinal tubules, and creating conditions for the application of endosealant.
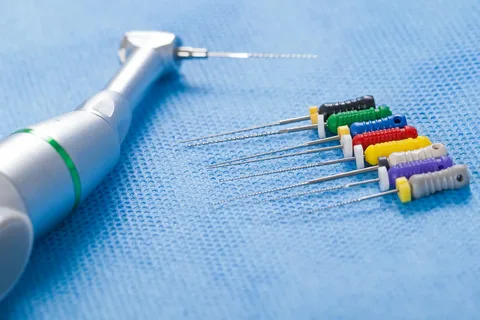
Figure 3. Endodontic instruments.
EDTA is produced in the form of gels or solutions in a concentration of 17%. The irrigation algorithm involves medicinal treatment of the canal lasting at least 30–45 minutes, which significantly exceeds the period of time required for instrumental treatment of the canal.
Ways to reduce drug treatment time:
increasing the volume of irrigant;
frequent drug changes;
ultrasonic activation of the solution.
Mechanical processing of channels
Basic methods of mechanical treatment of canals:
Standardized technology.
Step-back.
Crown-Down.
Balanced-forced tehnigue preparation.
Standardized technology
It involves expanding the channel with K-files; the following stages can be distinguished:
Passage of the canal, measurement of working length. Using K-reamer No. 8-15, the root canal is passed to a physiological narrowing. The working length is fixed with a locking disc.
The canal is expanded to a set length using a K-file corresponding to the size of the instrument used to traverse the canal. The movements of the K-file are rotational (“winding the watch”), followed by sawing movements.
As the root canal is processed, the K-files are replaced, each time the next size is taken. The channel is expanded to the required size, but minimally to No. 25.
This technique is relevant for processing straight channels that have a round cross-section, but it is not effective in the case of curved or complex channel configurations.

Figure 4. Mechanical processing of the canal.
Step-back
The apical-coronal “Step-back” technique (or step back), it is based on the use of endodontic instruments of increasing diameter to treat the canal from the apical narrowing to the mouth.
Stages of this technique:
Working length measurement.
A K-file is selected of such a size that it fits into the canal the entire length; it is used until the instrument begins to move freely in the canal. Next, the same thing is done with the next size instrument, after which control is carried out with the previous file to prevent blocking of the apex with dentinal filings. The canal expands its entire length to at least file No. 25 (Master Apical File).
Each subsequent tool processes a canal 1mm shorter than the previous one, but after each file a Master File is taken, which removes sawdust and smoothes the walls along the entire length of the canal.
Gates Glidden is used to treat the canal orifice.
Disadvantages of this technique
frequent pushing of dentine filings beyond the apex;
formation of a dentinal “plug”;
danger of root perforation;
shift in the position of the apical constriction due to the difficulty of controlling the working length during instrumentation and elimination of curvature in the canal.
Crown-Down
From the crown down or a step forward, the “Crown-Down” technique involves sequential machining of the canal from a larger instrument to a smaller one. In the modern concept of endodontic treatment, this technique is considered the most preferable.
Algorithm for instrumental canal processing using the Crown-Down technique:
Gates Glidden is used to treat the canal orifice.
We choose a large K-file, for example, No. 35, it is optimal to process the first 15mm of the canal. We work with this file until its movements in the canal become absolutely free. The upper third of the canal can also be processed using machine tools.
Each subsequent K-file is one size smaller than the previous one, so we continue until the tool is 3 mm from the expected working length. At this stage it is necessary to accurately determine the working length.
As soon as the canal is passed through its entire length, the operation is repeated, but we start with file No. 40, not No. 30, and then repeat the procedure with file No. 50, all manipulations are repeated until the apical third is processed to size 25.
The advantages of the Crown-Down technique are as follows:
minimal probability of pushing infected dentin residues beyond the apex;
convenience of canal irrigation;
low risk of the instrument moving beyond the apical foramen;
careful control when working in the apical third due to the initial creation of convenient access.
Balanced Strength Technique
Balanced-forced technique preparation is another technique used in endodontic treatment; it involves mechanical preparation of the canal using instruments equipped with an inactive tip. This technique is relevant for instrumental processing of canals of any configuration, both straight and curved, with curvatures.
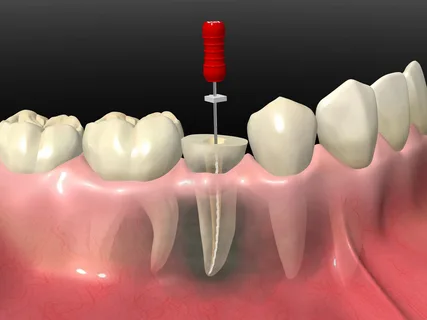
Figure 5. Endodontic treatment of the tooth.
Stages of the balanced strength technique:
The file is inserted into the canal until it stops, and it is turned clockwise by 90-120°.
Applying constant moderate pressure on the file with your finger so that it is at the fixed depth, it is rotated in the opposite direction by 270-360°. Manipulations must be carried out using a lubricating gel to prevent the file from jamming.
Each subsequent tool is one size larger than the previous one.
It is very important to control the pressure on the file so that it is not removed, but rotates at the same depth. After each file removal, the canal is cleaned and washed.
The steps are repeated until the entire length of the canal is processed. The finished channel has a smooth surface and a taper corresponding to the cone of the tool.
New practice-oriented information on endodontic treatment in the online course What's NEW in endodontics: from anesthesia to obturation .