Decision making for direct posterior restorations
DECISION-MAKING IN DIRECT RESTORATIONS:
Hybrid glass and short-fiber-reinforced composites.
Dr. ERALDO PESARESSI TORRES
The ‘Minamata convention’ urges the dental profession to promote oral health, reducing the need for restorative care, and when necessary, opt for alternatives to dental amalgam. Recent advances and consensus in cariology point to a diagnosis of caries risk and detection of lesions in stages that can be controlled without the need for surgery. The interpretation of dental caries as a non-communicable disease, biofilm-sugar dependent, allows changing the treatment approach towards modulating the patient's habits that allows postponing the first surgical intervention. However, when there is suspicion of a lesion that radiographically reaches the middle third of the dentin, a restorative approach will be required. The question to ask ourselves is: At what point should we intervene surgically in the caries process?
Clinical decision-making in relation to the cleaning techniques for a carious lesion and the ideal restorative materials for each case can be determined by some criteria such as: size and etiology of a lesion, aesthetics, number of affected teeth, periodontal considerations, endodontic and occlusal In the case of carious lesions or structural losses (class I, III, IV and V) the vast majority of cases can be resolved directly using restorative materials such as composite resin. In cases where the risk of caries is high or in cases of proximity to the pulp, a bioactive material such as a glass ionomer could be more recommendable, especially in young permanent teeth, where it is necessary to promote extrinsic mineralization.
Innovation around glass ionomers has managed to incorporate smaller vitreous particles (silicates) and greater reactivity, as well as the addition of higher molecular weight polyacrylic acid in an encapsulated presentation (EQUIA Forte Fil). This new technology allows to considerably improve the mechanical properties due to the acceleration of the formation of the matrix, forming a differential category in this type of products called 'hybrid glasses'. Additionally, the encapsulated presentation reduces the risk of the so-called 'operator factor' during mixing and application inside the cavity, making it consistent for the user. In addition, by applying a nano-filled resin coating (EQUIA Forte Coat), the material properties achieve their maximum potential for flexural strength and micro-hardness by protecting the material surface during the first few minutes of setting where there is a great risk of gain and loss of water. This new technology inherits some of the essential properties of conventional ionomers such as chemical adhesion (through the formation of chemical bonds between carboxyl radicals and calcium in the tooth structure) and the release of ions, such as strontium and fluorine, which contributing to the remineralization of the substrate and reducing the risk of secondary caries, respectively. As it is a biocompatible material that loses its acidity after a few minutes, the use of a cavity base is not required as long as there is at least 0.5 mm of dentin remnant from the pulp chamber.
When there are cases of teeth with extensive lesions, with loss of several cusps or root canal treatment, indirect alternatives are usually chosen, either in laboratory resin or ceramic materials. Teeth with extensive restorations or endodontically treated teeth are considered to be at higher risk of fracture due to their loss of dentin elasticity, loss of structural support elements (adamantine bridges, marginal ridges, pulp chamber roof, etc.) and lower water content. However, adhesive restorative materials allow the use of minimally invasive approaches that preserve the greatest amount of dental remnant and thus improve the long-term performance of restored teeth. Some indicators such as the depth of the cavity, the width of the isthmus and the cavity configuration are very critical factors to determine the reduction of dental rigidity and the risk of fracture. In cases of endodontically treated teeth, intra-radicular elements have proven not to be necessary to guarantee the adhesion of the restorative material, and are even associated with higher rates of catastrophic failures (those llas that compromise dental integrity without the possibility of repair). Currently, there are new additive adhesive alternatives that allow extending the survival of teeth with major structural compromises or endodontically treated, and allow reducing the unfavorable factor of polymerization contraction.
Innovations such as the use of braided polyethylene fibers have been launched on the market as a dentin substitute, however they are sensitive to the technique and skill of the operator. And despite being on the market for more than a decade, they do not have enough clinical evidence to support them. Recently, resin-based materials reinforced with short fibers (everX) designed for use as a stress-bearing restorative material that exceed the toughness of direct resinous materials, especially in cases of large tooth cavities, have been launched on the market in order to restore posterior vital and non-vital teeth. It consists of a combination of a resin matrix, randomly oriented E-glass fibers and inorganic particle fillers, which provides good bonding properties and improves the cohesion of the polymer matrix. Short fiber reinforced resin has shown significantly higher fracture toughness (2.4 MPa), flexural strength (124 MPa) and flexural modulus (12.6 GPa) than all other comparable resin materials as substitutes dentinal or core reconstruction. The reinforcing effect of fiber fillers is based on the transfer of stress from the polymer matrix to the fibers, but also on the behavior of individual short fibers as polymerization stress absorbers, cracks or cracks.
The success of the use of direct restorative materials depends to a great extent on the operator factor, therefore, materials that have fewer steps or that are easier to apply could present reproducibility advantages and, above all, extend the functional life of the treated teeth. Below are two clinical cases where hybrid glass-based materials are applied to a young permanent tooth with a primary carious lesion and another using fiber-reinforced resin as a dentin substitute in an endodontically treated tooth.
Case A
A 7-year-old female patient presents to the office for manifesting sensitivity in the 4th quadrant when consuming cold drinks or food. On clinical examination, tooth 46 presents an underlying shadow in the dentin seen from the occlusal view (Fig 1), which, when using the international system for the detection and assessment of dental caries, is considered an ICDAS 4 lesion (Underlying shadow in dentin with enamel). apparently intact). When performing the radiographic examination with a bitewing exposure, a radiolucent image is appreciated that reaches the middle third of the dentin (Fig 2). Due to the severity of the lesion, without an evident cavity, it was decided to perform enamel removal with high rotation using diamond burs in order to access the decayed dentin with manual instruments, complemented with a papain-based enzymatic agent (Papacarie Duo , Formula & Açao, Sao Paulo, Brazil) (Fig 3). Before proceeding with the cleaning of the cavity, an impression of the anatomy is taken with a gingival barrier material (Gingival barrier, SDI, limited, Bayswater– Australia) fixed in a micro-applicator (Fig. 4), so that Existing anatomy can be copied using the occlusal stamping technique (Fig. 5). After opening the cavity (Fig 6), the selective removal of the decayed tissue begins with a chemical-mechanical strategy (Fig 7) until reaching firm dentin at the base and hard at the periphery (Fig 8) under relative isolation. Using Optragate (Ivoclar Vivadent, Germany) and cotton rolls, the restorative material was applied: EQUIA forte fil (GC Corporation, Tokyo – Japan) (Fig 9). The material is extruded into the cavity after mixing for 10 seconds and then the capsule is placed in a clicker (Fig. 10) which allows the material to be extruded from the floor to the margins of the cavity in a single increment. Liquid Vaseline is immediately brushed onto the occlusal impression and stamping proceeds. After waiting for an initial setting of a couple of minutes, the abutment is removed and the excess that was extruded to the sides is removed using a manual instrument (Carver, LM Arte , Finland) (Fig. 11). The remains of Vaseline are removed and the EQUIA coat (GC Corporation, Tokyo – Japan) is applied over the surface of the material to then polymerize for 20 seconds (Fig 12). Occlusion control is performed and the patient is discharged with the recommendation to avoid consuming hard foods for the next few hours (Fig 13).

Fig 1

Fig 2
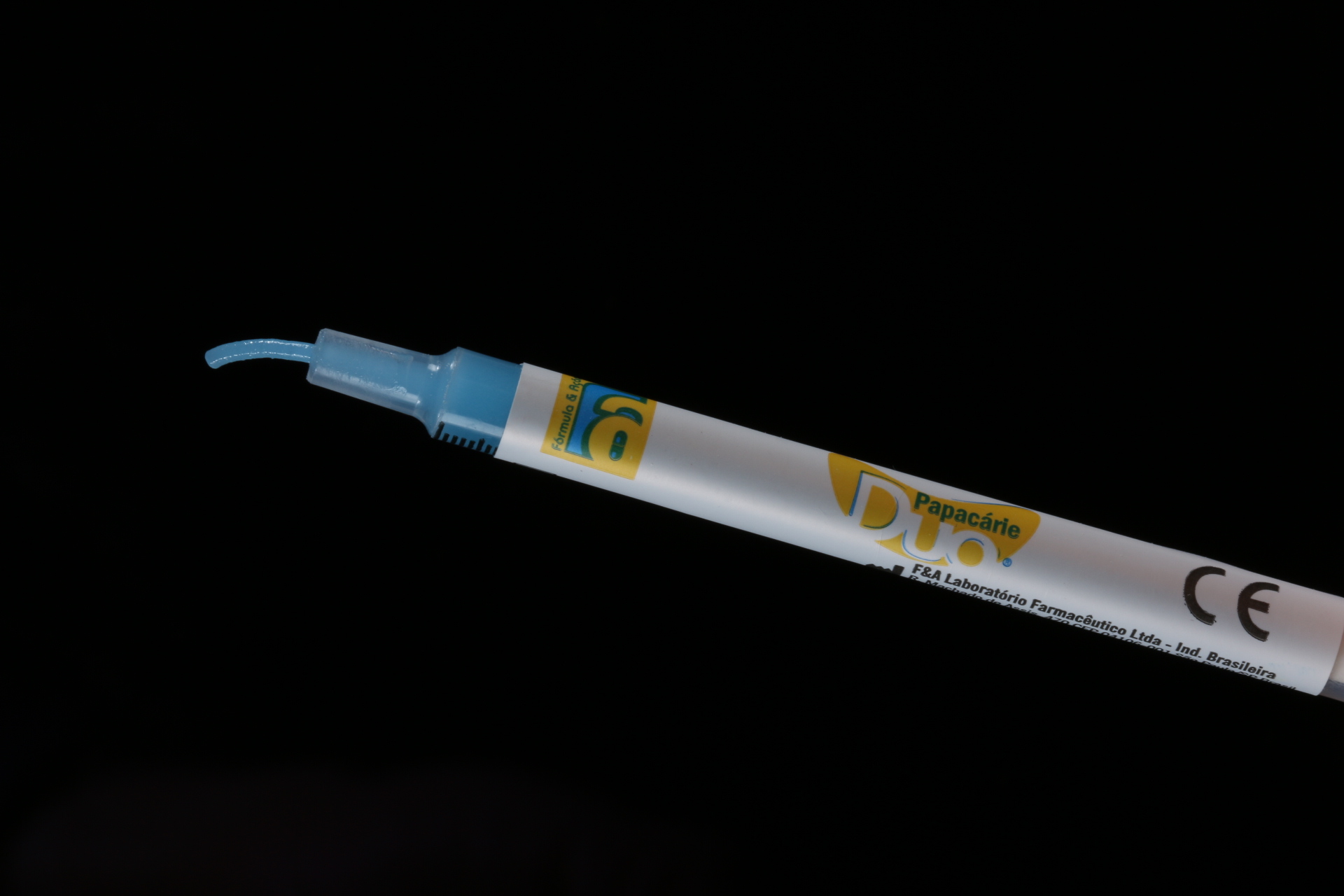
Fig 3

Fig 4
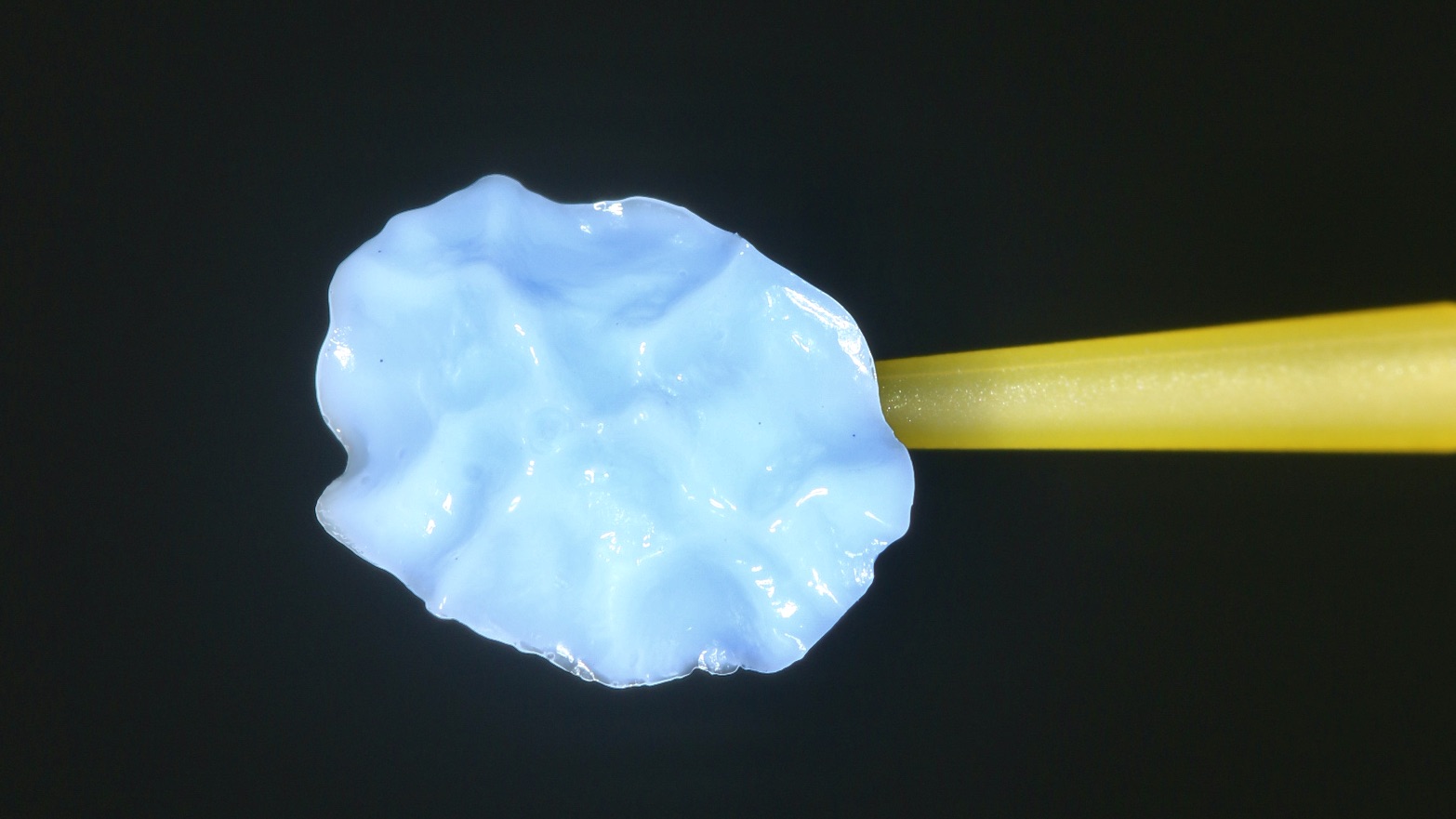
Fig 5

Fig 6

Fig 7

Fig 8

Fig 9

Fig 10
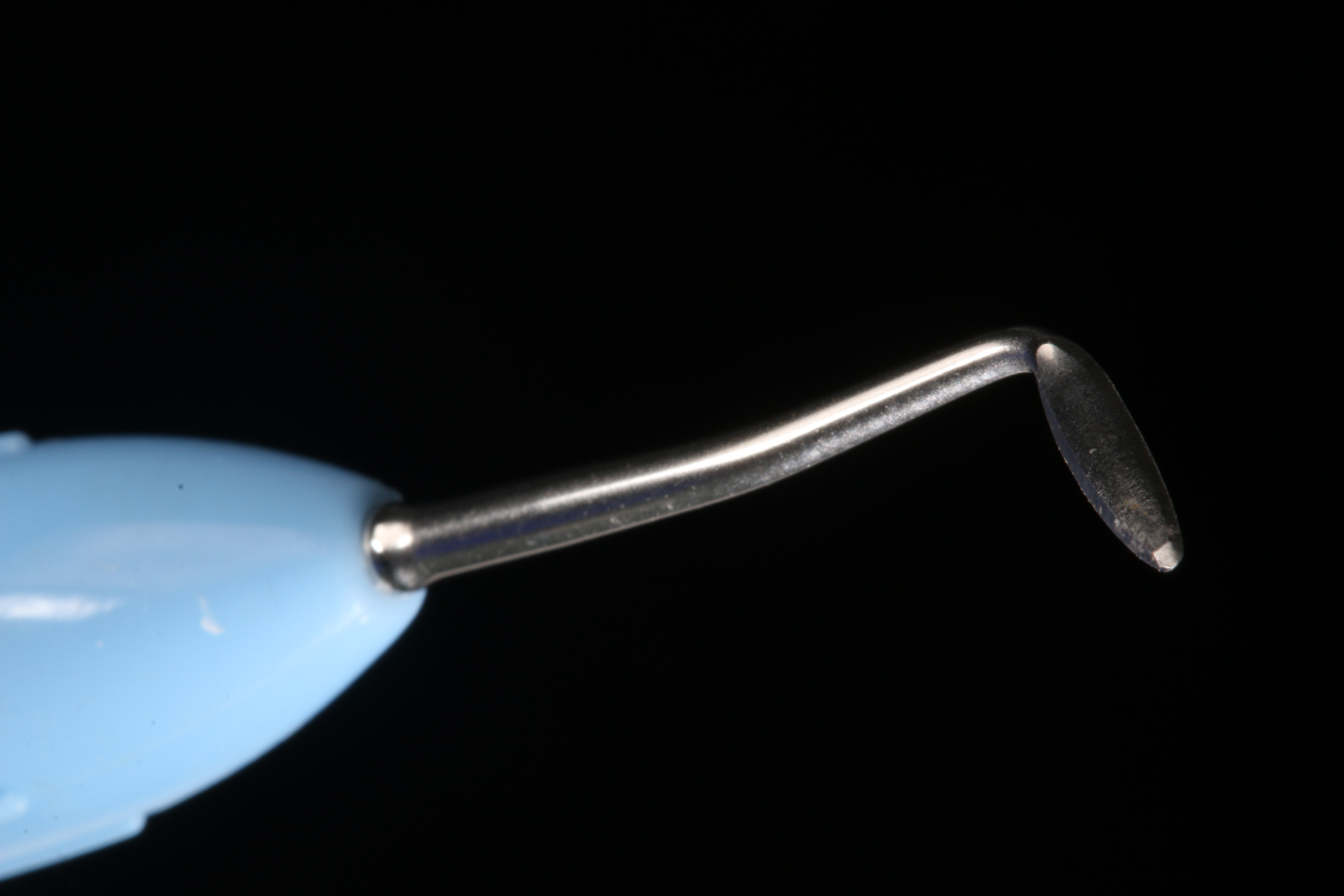
Fig 11
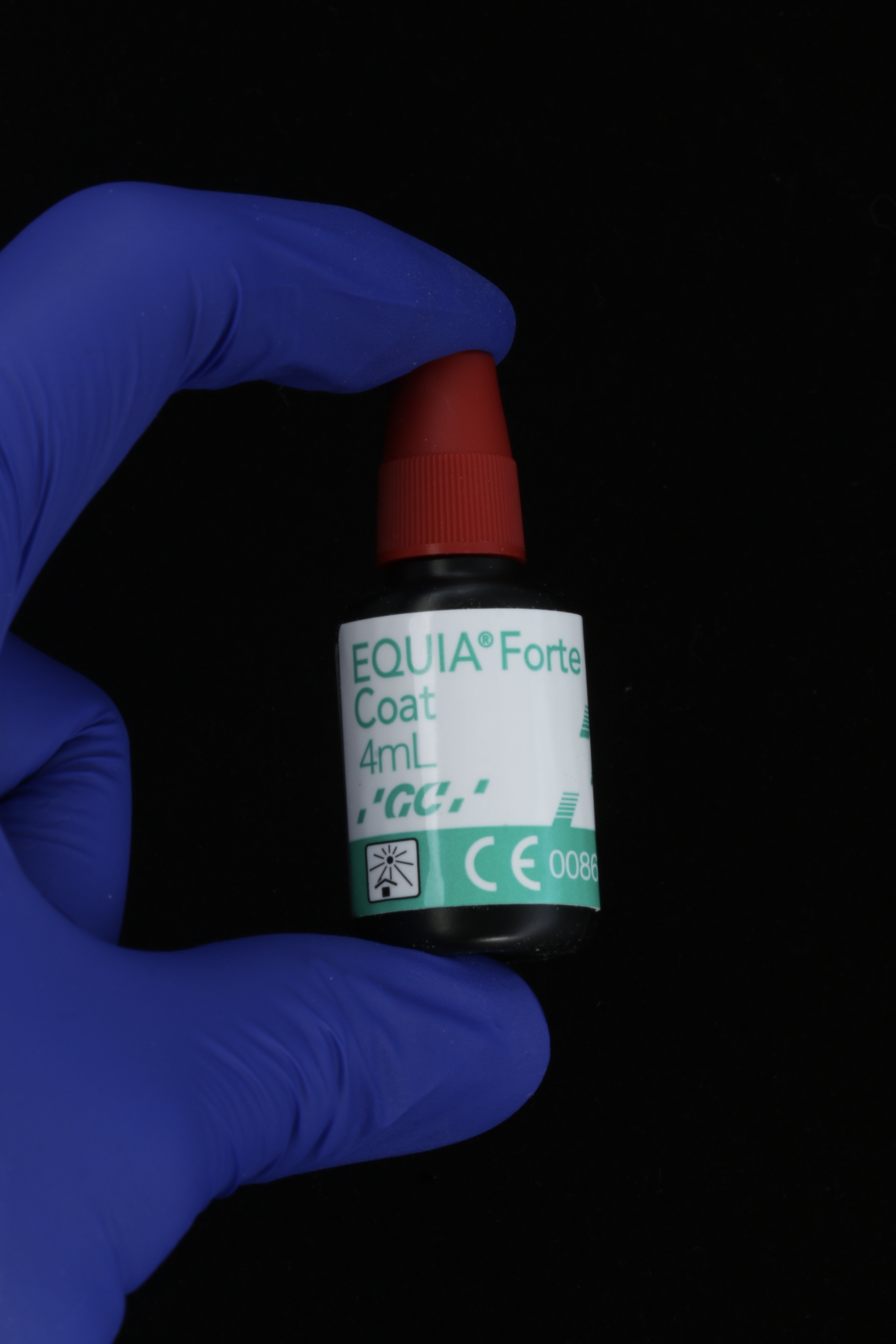
Fig 12

Fig 13
Case B
A 64-year-old female patient presents to the office with a secondary carious lesion around a resin-based restoration on the occlusal and distal surfaces in an endodontically treated tooth (Fig 14), the upper left first premolar (tooth 24). Due to the secondary lesion and the poor condition of the restoration, it is suggested to replace it with a new direct restoration in composite resin using EverX Flow (GC Corporation, Tokyo – Japan) as a dentin substitute (Fig 15). Proceed with absolute isolation using a rubber dam upon removal of the restoration, preserving the remaining dental structure (Fig. 16). We proceed to clean the margins of the preparation with high-speed multi-laminate burs and manual instruments, in enamel and dentin. Sandblasting is carried out with 30 µm aluminum oxide particles at 2 bar pressure (Fig. 17) and then selective acid etching is carried out on the enamel margins for 15 seconds. Immediately after thorough rinsing and removing excess water, a Solare Bond universal adhesive system (GC Corporation, Tokyo – Japan) is applied over the entire cavity (Fig. 18), agitating vigorously on dentin and gently on enamel margins. for 10 to 20 seconds, proceed with the evaporation of solvents and photopolymerization of the adhesive is carried out for 40 seconds. To avoid exposing the fiber-reinforced resin to the oral environment, the distal wall is reconstructed in two increments, using a metal matrix (Omnimatrix, Ultradent Products, Oregon – USA) (Fig. 19). After removing excess resin, polishing the wall with discs and rubbers (Fig. 20), 2mm horizontal increments are made using the following sequence: first 2mm increment of EverX (Figs. 21, 22), light-curing for 40 seconds, second EverX increment of 2mm (Fig. 23), light-curing for 40 seconds, third increment of 2mm with Gradia AO3 resin (GC Corporation, Tokyo – Japan) (Figs. 24), light-curing for 40 seconds, fourth increment with Gradia resin A2 (GC Corporation, Tokyo – Japan), light-curing for 40 seconds, application of ocher/brown pigments in pits and fissures, light-curing on for 40 seconds (Fig 25). After finishing and polishing sequence (rubbers, felts and diamond paste) the dam is removed to control occlusion and wear of premature contact points.

Fig 14

Fig 15
 Fig 16
Fig 16

Fig 17
Fig 18

Fig 19

Fig 20

Fig 21
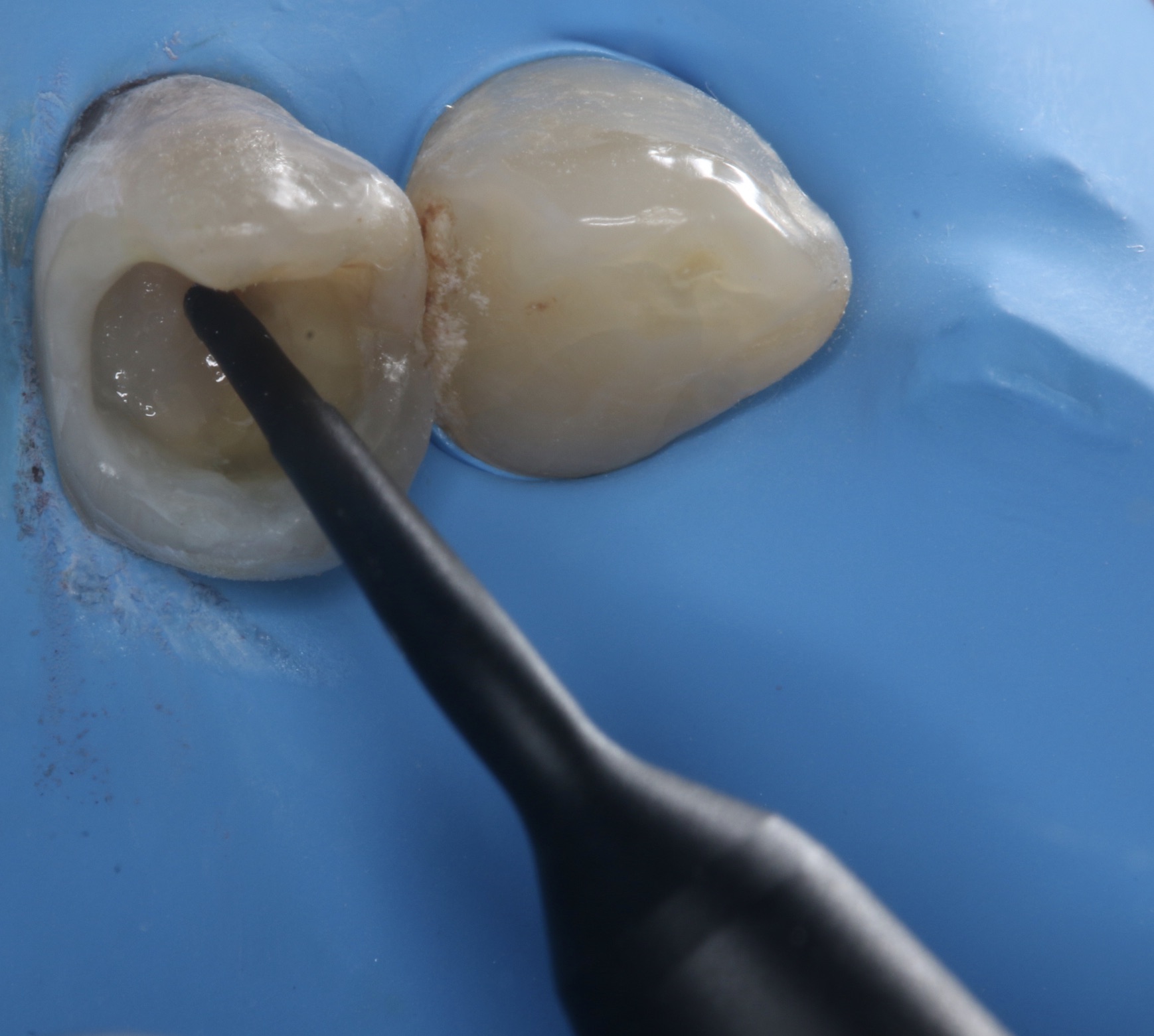
Fig 22

Fig 23
Fig 24
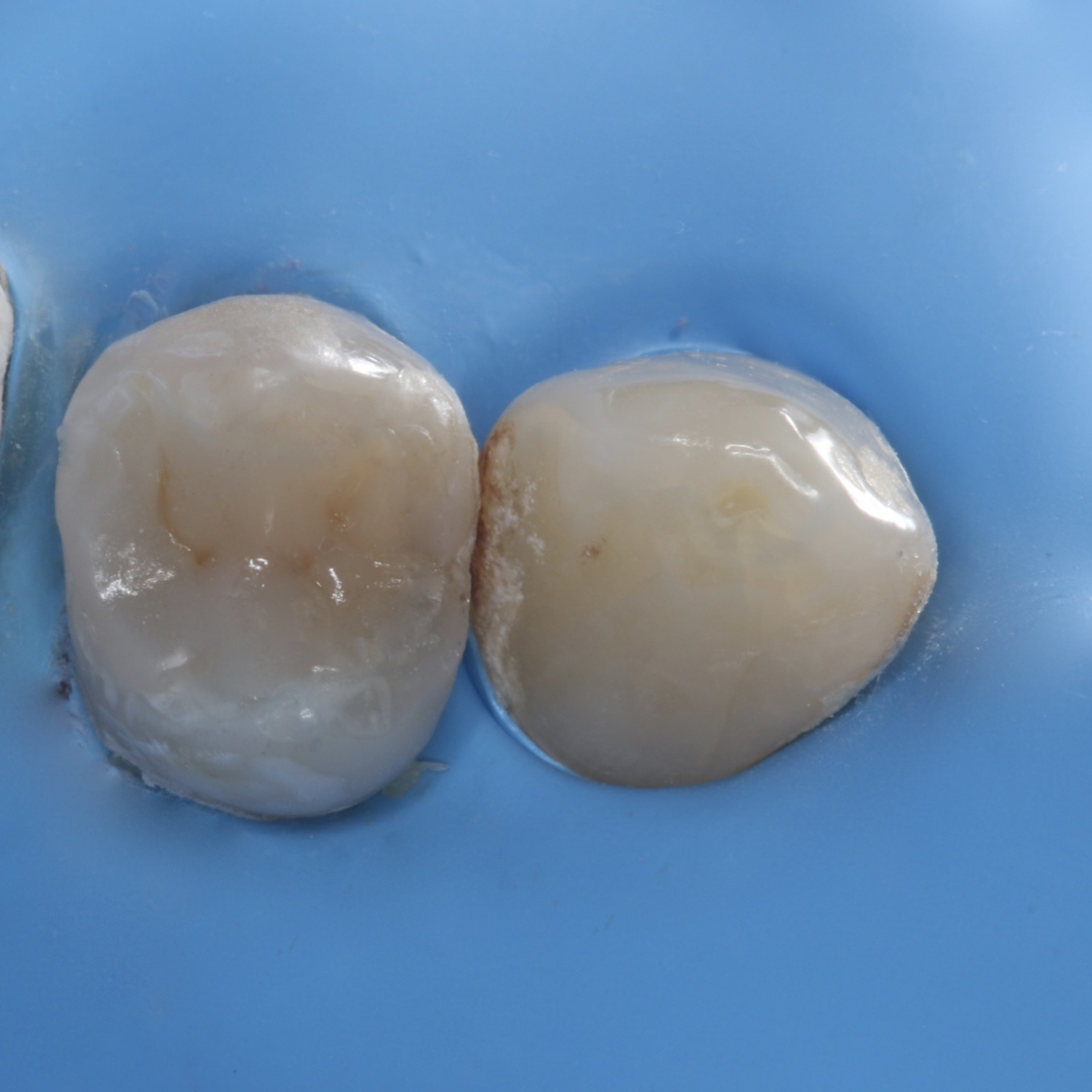
Fig 25
Final comments:
The control of dental caries disease has a purely behavioral approach (reduction of free sugars in the diet and daily disorganization of the dental biofilm), and the treatment of caries lesions should incorporate conservative strategies with bioactive materials (that promote remineralization) and / or biomimetic (that resemble the dental structures they seek to replace). New dental materials based on hybrid glasses and fiber-reinforced resins offer a simplification of clinical procedures and offer more affordable alternatives for patients.