
Removal of Filling Materials from Oval-shaped Canals Using Laser Irradiation: A Micro–computed Tomographic Study
Abstract
Introduction: The aim of this study was to assess the efficacy of lasers in removing filling remnants from oval-shaped canals after retreatment procedures with rotary instruments using micro–computed tomographic imaging.
Methods: The root canals of 42 mandibular canines were prepared and obturated using the warm vertical compaction technique. Retreatment was performed with rotary instruments, and the specimens were distributed in 3 groups (n = 14) according to the laser device used in a later stage of retreatment procedure: Er:YAG, Er:YAG laser–based photon-induced photoacoustic streaming, and Nd:YAG. The specimens were scanned in a micro–computed tomographic device after root canal filling and each stage of retreatment at a resolution of 13.68 μm. The percentage differences of the remaining filling material before and after laser application within and between groups were statistically compared using the paired sample t test and 1-way analysis of variance test, respectively. Significance level was set at 5%.
Results: Overall, filling residues were located mainly in the apical third and into canal irregularities after the retreatment procedures. After using rotary instruments, the mean percentage volume of the filling remnants ranged from 13%–16%, with no statistical significant difference between groups (P > .05). Within groups, additional laser application had a significant reduction in the amount of the remaining filling materials (P < .05). A comparison between groups showed that Er:YAG laser application after the use of rotary instruments had a significantly higher removal of filling remnants (~13%) than Er:YAG laser–based photon-induced photoacoustic streaming (~4%) and Nd:YAG (~3%) (P < .05).
Conclusions: None of the retreatment procedures completely removed the filling materials. The additional use of lasers improved the removal of filling material after the retreatment procedure with rotary instruments. (J Endod 2015;■:1–6)
Root canal procedures involve the use of instruments and substances to clean, shape, and disinfect the root canal system as well as materials to fill the root canal space. Although recent advances in endodontic instruments and devices have made proper root canal treatment more predictable, failure can occur. In cases in which endodontic therapy has failed, the nonsurgical approach has been the preferred treatment. The main goal of nonsurgical canal retreatment is to re-establish healthy periapical tissues by the removal of the root canal filling materials, further cleaning and shaping, and refilling. Therefore, the removal of as much filling material as possible from an inadequately prepared and/or filled root canal system is necessary to uncover remaining necrotic tissues or bacteria that might be responsible for periapical inflammation and, thus, post-treatment disease.
Traditionally, root canal retreatment has been accomplished using solvent and hand files. An attempt to use rotary nickel-titanium (NiTi) instruments specifically designed for retreatment, such as the R-Endo system (Micro-Mega, Besançon, France), has led to the development of a more efficient way to remove the bulk of the filling materials in comparison with conventional techniques. Unfortunately, several reports showed substantial amounts of filling remnants in the canal after retreatment using rotary instruments. Despite the fact that it has not been proved that the complete removal of filling materials can improve the outcome of the retreatment procedure, filling remnants can theoretically impair disinfection by avoiding irrigants to contact the persisting microorganisms. During this process, the anatomy of the root canal system must always be taken into account because the cross-sectional root canal shape has been reported to significantly influence the retreatment procedure. Although in straight canals with a round cross-section the operator may simply use rotary files of greater dimensions in order to remove filling residues, the retreatment of oval-shaped canals requires additional procedures because further enlargement may create complications such as root perforation or canal transportation.
Additional attempts to improve the removal of filling remnants have been made with ultrasonic systems, heat-carrying devices, solvents, and lasers. The application of lasers in retreatment procedures relies mainly on the thermal effect of irradiation, which presents evidence to improve the removal of filling remnants. Recently, photon-induced photoacoustic streaming (PIPS), a new laser-activated irrigation system device, has been introduced. This system uses a very low-power source (subablative) to rapidly pulse laser light energy, which is absorbed by the molecules within the irrigant. This transfer of energy results in a series of rapid and powerful shock waves capable of forcefully propelling the irrigant throughout the root canal system.
Currently, despite some types of lasers being tested as an adjunct in nonsurgical retreatment, no study has investigated the use of PIPS in a later stage of endodontic retreatment. Thus, the aim of this study was to assess the efficacy of lasers in removing filling remnants from oval-shaped canals after retreatment with rotary instruments using micro–computed tomographic (micro-CT) imaging. The null hypothesis tested was that there is no difference in the percentage of filling remnants with the additional use of laser after a first retreatment stage with rotary instruments.
Materials and Methods
Sample Selection
After ethics committee approval (protocol #116/2013), 110 straight single-rooted extracted mandibular canines were initially selected on the basis of radiographs (Belmont Phot-X II; Takara Belmont Corp, Osaka, Japan) taken in both buccolingual and mesiodistal directions to detect any possible root canal obstruction. All teeth presenting apical curvature, previous endodontic treatment, resorptive defects, or more than 1 root canal were excluded. The specimens were disinfected in 0.1% thymol solution and stored in distilled water at 4◦C.
To attain an overall outline of the internal anatomy, each tooth was scanned in a micro-CT device (SkyScan 1172; Bruker-microCT, Kontich, Belgium) at an isotropic resolution of 13.68 μm, 100 kV, 100 μA, 180◦ rotation around the vertical axis, rotation step of 0.4◦, and camera exposure time of 1900 milliseconds. X-rays were filtered with a 500-μm-thick aluminum filter and a 38-μm-thick copper filter. Frame averaging of 2 and random movements were also applied to the acquisition phase for increasing signal-to-noise ratio and reducing ring artifacts. The acquired projection images were reconstructed into cross-section slices (NRecon v.1.6.9, Bruker-microCT), and 3-dimensional models of the canals were obtained. Additionally, morphologic parameters of the canals (root length, volume, surface area, and structure model index) were calculated using CTAn v.1.14.4 software (Bruker-microCT). Then, 42 mandibular canines presenting the ratio of the long to the short diameter of the canal >2 at 5 mm from the apex and >3 at 8 mm from the apex were selected. These teeth were matched to create 14 threesomes based on the morphologic aspects of the root canals. One tooth from each threesome was randomly assigned to 1 of the 3 experimental groups (n = 14). After checking the normality assumption (Shapiro-Wilk test), the degree of homogeneity (baseline) of the 3 groups with respect to the morphologic parameters of the root canals was confirmed by 1-way analysis of variance test (P > .05).
Root Canal Preparation
Root canals were accessed, and the coronal third was flared with a #3 LA Axxess Stainless Steel bur (SybronEndo, Orange, CA) followed by irrigation with 5 mL 2.5% sodium hypochlorite (NaOCl). Patency was confirmed by inserting a size 10 K-file (Dentsply Maillefer, Baillagues, Switzerland) through the apical foramen before and after completion of root canal preparation. For all groups, a glide path was created by scouting a stainless steel size 15 K-file (Dentsply Maillefer) up to the WL, which was established by deducting 1 mm from the canal length. The root canals were then serially enlarged by a single experienced operator with Revo-S NiTi rotary instruments (Micro-Mega) driven by a torque-controlled motor (W&H, Bürmoos, Austria) using a gentle in-and-out motion in a crown-down manner. SC1, SC2, and SU instruments were used up to the WL, resulting in an apical third shaped to a size 25, 0.06 taper. Then, the sequence was completed using apical preparation instruments (AS 30, 35, and 40) up to the WL. Apical enlargement was finished manually with a size 45 K-File (Mani Co, Tokyo, Japan). Between each preparation step, irrigation was performed using disposable syringes with a 30-G NaviTip needle (Ultradent, South Jordan, UT) inserted 1 mm short of the WL in a total of 20 mL 2.5% NaOCl per canal. A final rinse with 5 mL 17% EDTA (pH = 7.7), delivered at a 1-mL/min rate for 5 minutes, followed by a 5-minute 5-mL rinse with bidistilled water was performed. Then, canals were dried with absorbent paper points (Dentsply Maillefer).
Root Canal Filling
Root canals were obturated using the warm vertical compaction technique (BeeFill 2in1; VDW, Munich, Germany). After coating the canal walls with a thin layer of sealer (AH Plus; Dentsply DeTrey GmbH, Konstaz, Germany), a size 45, 0.02 taper gutta-percha master cone (Aceone-Endo; Aceonedent Co, Geonggi-Do, Korea) coated with sealer was fit with tug back to the WL. The sequential removal of thermoplasticized gutta-percha and vertical condensation of the remaining filling materials were completed when an ISO size 60 hot plugger (BeeFill Downpack, VDW) was 3–4 mm from the WL. The canals were then backfilled using the BeeFill Backfill unit (VDW) according to the manufacturer’s instructions. Radiographs were taken in both buccolingual and mesiodistal directions to confirm the adequacy of root canal filling. If voids were observed in the obturation mass, the specimen was replaced by another one with similar canal morphology. Then, the specimens were stored at 37◦C and 100% relative humidity for 1 week to allow the complete setting of the sealer.
Root Canal Retreatment
The retreatment procedure was performed with R-Endo NiTi rotary instruments driven by a torque-controlled motor (W&H) set to 340 rpm with circumferential filing action. The R-Endo Re instrument (15 mm; size 25, 0.12 taper) was used up to 3 mm beyond the canal orifice followed by the R1 instrument (15 mm; size 25, 0.08 taper) to the beginning of the middle third. Then, R2 (19 mm; size 25, 0.06 taper) and R3 (23 mm; size 25, 0.04 taper) instruments were used to the apical third. Considering that the teeth were not decoronated with the purpose of making a sufficient reservoir for the laser activation of the irrigants, R-Endo instruments were not able to reach the WL. Therefore, retreatment was further accomplished manually using a size 45 K-file (Dentsply Maillefer) to the WL. Each canal was irrigated with 5% NaOCl solution between files in a total of 20 mL per canal. The instruments were replaced after 4 canals, and retreatment was considered completed when the WL was reached, no material was observed between the flutes of the instruments, and the irrigating solution appeared clear of debris after the final rinse. Then, apex was sealed with 2 layers of nail varnish, and a flip of a coin was used to define which experimental group would be treated with each of the following additional applications of laser irradiation:
Group 1 (n = 14): Irradiation with an Er:YAG laser (2,940 nm, Fidelis AT; Fotona, Ljubljana, Slovenia) at 1 W, 20 Hz, and 50 mJ per pulse in the very short pulse mode (VSP) delivered with a 14-mm-long optic fiber plain tip (Ø = 300 μm). The laser was activated after the tip of the optic fiber was placed 3 mm from the WL. Then, the tip was withdrawn gently from the apical to the coronal region with helical movement and reintroduced to the apex.
Group 2 (n = 14): Irradiation with an Er:YAG laser (2940 nm, Fotona) at 1 W, 20 Hz, and 50 mJ per pulse in the VSP mode delivered with a 14-mm-long tapered PIPS fiber tip (Ø = 300 μm). The tip was placed at the access opening in the pulpal chamber, remaining stationary.
Group 3 (n = 14): Irradiation with an Nd:YAG laser (1064 nm, Fotona) at 1 W, 20 Hz, and 50 mJ per pulse in the VSP mode delivered with an optic fiber plain tip (Ø = 320 μm). Laser irradiation was applied as in group 1.
In all groups, irradiation was performed after the air and water spray of the laser units were set to ‘‘off’’ and the root canal was filled with 5% NaOCl solution. Ten-second intervals of laser-activated irrigation were followed by 10 seconds of no activation (‘‘resting’’) in between. These intervals were repeated 6 times (for a total of 60 seconds) using a volume of 5 mL 5% NaOCl. Then, the same irrigation protocol and laser irradiation were performed using 17% EDTA as irrigant solution. After the laser application, a final rinse was performed with 15 mL distilled water.
During the experimental procedure, 3 high-resolution micro-CT scans were accomplished per tooth following the aforementioned parameters: (1) after root canal filling, (2) after retreatment with R-Endo instruments, and (3) after laser application. The volume of interest was selected extending from the incisal edge to the apex, resulting in the acquisition of 1200 to 1500 transverse cross-sections per tooth. The original gray scale images were processed with a slight Gaussian low-pass filtration for noise reduction, and an automatic segmentation threshold was used to separate root dentin from the filling materials using CTAn v.1.14.4 software (Bruker-microCT). Separately, and for each slice, regions of interest were chosen to allow the calculation of the volume of the filling materials (in mm3). The remaining filling materials after the retreatment procedures were expressed as a percentage of the total initial root filling volume using the formula VA * 100/VB, where VB and VA mean the volume (in mm3) of the filling material before and after each retreatment stage, respectively. Polygonal surface representations of the teeth and the filling materials were also constructed for qualitative evaluation (CTVol v.2.2.1, Bruker-microCT).
Statistical Analysis
The Shapiro-Wilk and Levene tests were used to evaluate the assumption of normality and the equality of variance among the data sets. Considering that the percentage volumes of the remaining filling materials were normally distributed (P > .05), they were presented as means and standard deviations and statistically compared using the 2-way analysis of variance test. The percentage differences of the remaining filling material before and after laser application within and between groups were statistically compared using the paired sample t test and the 1-way analysis of variance test, respectively. For all groups, the significance level was set at P < .05 (SPSS v11.0 for Windows; SPSS Inc, Chicago, IL).
Results
Table 1 summarizes the means and standard deviations of the percentage remaining filling materials of the experimental groups after the use of rotary instruments as well as additional laser irradiation. Overall, none of the retreatment procedures completely removed the filling materials from the root canals.
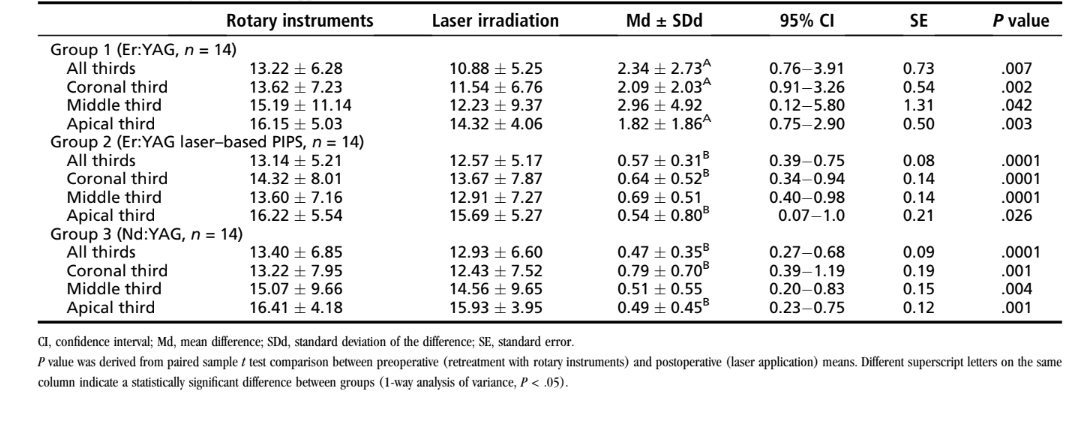
After using rotary instruments, the mean percentage volume of the filling residue ranged from 13%–16%, with no statistical significant difference between groups (P > .05). Despite qualitative analysis showing filling remnants located mostly in canal irregularities in the apical third (Fig. 1), no statistically significant interaction between the independent variables (rotary instruments and the root canal thirds) on the amount of the filling residue (P > .05) was observed.
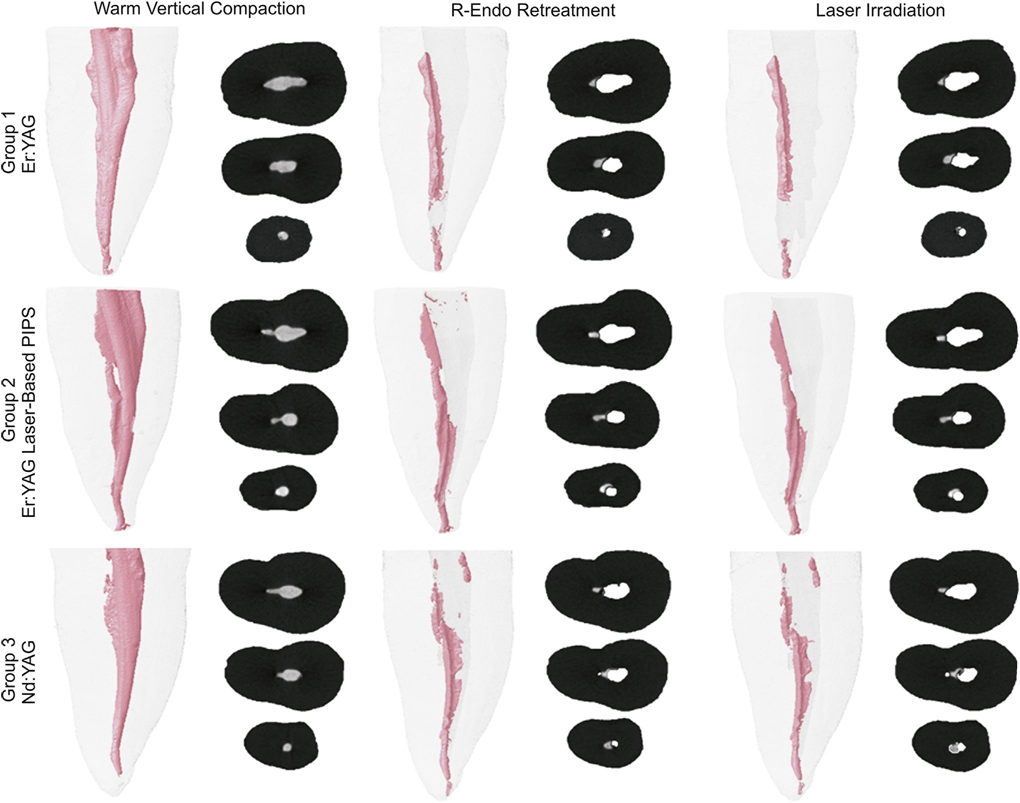
warm vertical compaction technique, retreatment with R-Endo instruments, and additional laser application with different devices followed by the respective
cross-sections from the coronal, middle, and apical thirds of the roots in which the filling materials are depicted in gray.
The paired sample t test indicated that the additional application of lasers caused a significant reduction in the amount of the remaining filling materials (P < .05). A comparison between groups showed that Er:YAG laser irradiation after retreatment with rotary instruments resulted in a significantly higher removal of filling remnants (~13%) than Er:YAG laser–based PIPS (~4%) and Nd:YAG (~3%) (P < .05).
Discussion
Controversial results regarding the efficacy of rotary instruments on the root canal retreatment procedures can be found in the literature and may be explained by methodological differences among the studies such as sample selection, evaluation methods, experimental design (ie, number of files, time of the procedure, speed and torque of the motor, taper and size of instruments, and amount of irrigants), and the additional use of heat or solvents. Regarding the latter, no solvent was applied in this study with the purpose to eliminate a possible confounding factor. Softened root filling material by solvents could be pushed further into the irregularities along the root canal walls and dentinal tubules, making its removal more difficult.
The present results support previous studies in which no retreatment protocol was able to completely remove filling material from within the root canal space. A relatively large amount of filling remnants left in the canal after the first stage of the retreatment with rotary instruments in all experimental groups (~13%), mostly in the apical third, was observed (Fig. 1). These results are not surprising and may be explained by the following:
- The dimensions of the canal after shaping procedure (up to size 45), which was bigger than the size of the retreatment rotary instruments (size 25)
- The resistance to displacement of the sealer used herein (AH Plus) because of its high bond strength to the dentin
- The oval-shaped cross-sectional geometry of the root canals, which favored melted residues to be pushed into canal irregularities
As previously stated by other authors, these findings suggest the need of a supplementary method for removing the remaining filling material after retreatment with rotary instruments.
Recently, the Self-Adjusting File cleaning-shaping-irrigation system (ReDent-Nova, Ra’anana, Israel) was successfully used after rotary instruments as an effective second stage of root canal retreatment. Similarly, laser devices with different wavelengths seem promising for being used in a later retreatment stage for filling remnants removal. In the present study, the use of lasers resulted in a significant reduction in the amount of remaining filling material after retreatment with R-Endo rotary instruments. Among the tested devices, a significantly higher percentage removal of filling materials was observed with the Er:YAG laser in comparison with Er:YAG laser–based PIPS and Nd:YAG. Consequently, the null hypothesis tested was rejected.
Unlike Nd:YAG lasers, the output of an Er:YAG laser has a water- mediated photomechanical interaction based on photothermal and photoablation mechanisms. Although the photothermal effect may have resulted in the carbonization of filling material, the photoablation mechanism probably affected the dentinal surface, facilitating the detachment of the filling remnants from the canal walls and their subsequent removal by the irrigation procedure. Additionally, the Er:YAG laser has been proven to promote composite resin ablation. Thus, it also may be hypothesized that its irradiation resulted in partial melting and vaporization of the resin-based sealer used herein. Er:YAG laser–based PIPS harnesses the power of the laser irradiation to create photoacoustic shock waves within the irrigant solution, causing the movement of fluids in the canal because of a secondary cavitation effect. However, subablative power levels emanating from the pulsed low-energy laser minimize its thermal effects, explaining the less than ideal ability of this laser in removing filling remnants from the root canal. Conversely, the heating effect of the Nd:YAG laser beam is probably the reason for the low percentage of filling removal in this group. The pulsed Nd:YAG laser beam probably affected the surrounding dentin, causing its fusion and promoting the melt of the filling remnants and increasing their retention to the root canals walls.
The main role of laboratory-based studies is to develop well-controlled conditions that are able to reliably compare certain factors. The main confounding factor of ex vivo studies is the anatomy of the root canal system under investigation. Consequently, the results might show the effect of canal anatomy rather than the variable of interest. In the present study, several attempts have been made to create a reliable anatomic baseline to ensure the comparability of the groups, which probably eliminated potentially significant anatomic biases that could interfere with the results. The similar behavior of the R-Endo rotary instruments in all groups observed after the first stage of the retreatment procedure was probably caused by the sample distribution based on the 3-dimensional morphologic parameters of the canals. The evaluation method also plays an important role on the outcome of studies on root canal retreatment. In earlier studies, the evaluation of the remaining filling materials was mostly accomplished by sectioning the specimens or a comparative analysis of radiographic images. These methods have been successfully used for many years; however, they do not allow for a precise quantification of the volume of the filling materials. In contrast, algorithms used in the nondestructive micro-CT technology allow the 3-dimensional reconstruction as well as an accurate mathematical calculation of the volume of the materials within the root canal space, overcoming the limitations of the conventional methods.
This study showed that laser irradiation may be absorbed by the current filling materials, thus confirming its ability for removing remnants after root canal retreatment. However, it must be pointed out that multiple factors can influence the various types of laser tissue interactions for each wavelength of emission. Most types of interactions are strongly dependent on the inherent optical absorption properties of different materials and tissues. In endodontic retreatment, the laser light interaction with matter may not be energy dependent because of the heterogeneous nature of the root canal materials or obstacles. Therefore, the adequate control of energy, density, and pulse duration in regard to the canal environment for root canal retreatment still needs to be achieved.
Among the experimental groups, the Er:YAG laser was the only device that presented some potential for being used in a later stage of the retreatment procedure. However, considering the 95% confidence interval of each group, the effect size of the difference of the percentage volume of the remaining filling materials after R-Endo and laser application was small, suggesting that the improvement in the removal of filling materials by the laser may not be substantial in real terms. Moreover, in a clinical setup, the interactions involved between laser energy within the root canal can cause an increase in the temperature to the point that the tooth may be lost or even damaging the soft tissue that connects the tooth to the surrounding bone.
Conclusions
Under the limitations of this ex vivo study, neither retreatment protocols were able to render root canals free of root filling remnants.
The additional use of lasers improved the removal of filling materials after canal retreatment with rotary instruments.
Authors: Ali Keleş, PhD, Hakan Arslan, Aliye Kamalak, Merve Akçay, Manoel D. Sousa-Neto, Marco Aurélio Versiani
References:
Siqueira JF Jr. Reaction of periradicular tissues to root canal treatment: benefits and drawbacks. Endod Topics 2005;10:123–47.
Hammad M, Qualtrough A, Silikas N. Three-dimensional evaluation of effectiveness of hand and rotary instrumentation for retreatment of canals filled with different materials. J Endod 2008;34:1370–3.
Torabinejad M, Corr R, Handysides R, Shabahang S. Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod 2009;35: 930–7.
Rechenberg DK, Paqué F. Impact of cross-sectional root canal shape on filled canal volume and remaining root filling material after retreatment. Int Endod J 2013;46: 547–55.
Friedman S, Stabholz A, Tamse A. Endodontic retreatment—case selection and technique. 3. Retreatment techniques. J Endod 1990;16:543–9.
Taşdemir T, Er K, Yildirim T, Celik D. Efficacy of three rotary NiTi instruments in removing gutta-percha from root canals. Int Endod J 2008;41:191–6.
Abramovitz I, Relles-Bonar S, Baransi B, Kfir A. The effectiveness of a self-adjusting file to remove residual gutta-percha after retreatment with rotary files. Int Endod J 2012;45:386–92.
Somma F, Cammarota G, Plotino G, et al. The effectiveness of manual and mechanical instrumentation for the retreatment of three different root canal filling materials. J Endod 2008;34:466–9.
Zmener O, Pameijer CH, Banegas G. Retreatment efficacy of hand versus automated instrumentation in oval-shaped root canals: an ex vivo study. Int Endod J 2006;39: 521–6.
Ünal GC, Kaya BU, Tac¸ AG, Keçeci AD. A comparison of the efficacy of conventional
and new retreatment instruments to remove gutta-percha in curved root canals: an ex vivo study. Int Endod J 2009;42:344–50.
de Chevigny C, Dao TT, Basrani BR, et al. Treatment outcome in endodontics: the Toronto study—phases 3 and 4: orthograde retreatment. J Endod 2008;34: 131–7.
Simsek N, Keleş A, Ahmetoglu F, et al. Comparison of different retreatment techniques and root canal sealers: a scanning electron microscopic study. Braz Oral Res [Epub ahead of print], http://dx.doi.org/10.1590/1807-3107BOR-2014. vol28.0006, 2014;28.
Wu MK, Wesselink PR. A primary observation on the preparation and obturation of oval canals. Int Endod J 2001;34:137–41.
Keleş A, Alcin H, Kamalak A, Versiani MA. Oval-shaped canal retreatment with self-adjusting file: a micro-computed tomography study. Clin Oral Investig 2014;18: 1147–53.
Solomonov M, Paqué F, Kaya S, et al. Self-adjusting files in retreatment: a high-resolution micro-computed tomography study. J Endod 2012;38:1283–7.
Voet KC, Wu MK, Wesselink PR, Shemesh H. Removal of gutta-percha from root canals using the self-adjusting file. J Endod 2012;38:1004–6.
Ruddle CJ. Nonsurgical retreatment. J Endod 2004;30:827–45.
Blum JY, Peli JF, Abadie MJ. Effects of the Nd:YAP laser on coronal restorative materials: implications for endodontic retreatment. J Endod 2000;26:588–92.
Farge P, Nahas P, Bonin P. In vitro study of a Nd:YAP laser in endodontic retreatment. J Endod 1998;24:359–63.
Tachinami H, Katsuumi I. Removal of root canal filling materials using Er:YAG laser irradiation. Dent Mater J 2010;29:246–52.
Vidučić D, Jukić S, Karlović Z, et al. Removal of gutta-percha from root canals using an Nd:YAG laser. Int Endod J 2003;36:670–3.
Lloyd A, Uhles JP, Clement DJ, Garcia-Godoy F. Elimination of intracanal tissue and debris through a novel laser-activated system assessed using high-resolution micro- computed tomography: a pilot study. J Endod 2014;40:584–7.
Deleu E, Meire MA, De Moor RJ. Efficacy of laser-based irrigant activation methods in removing debris from simulated root canal irregularities. Lasers Med Sci [Epub ahead of print], http://dx.doi.org/10.1007/s10103-013- 1442-y; 2013.
Horvath SD, Altenburger MJ, Naumann M, et al. Cleanliness of dentinal tubules following gutta-percha removal with and without solvents: a scanning electron microscopic study. Int Endod J 2009;42:1032–8.
Kimura Y, Wilder-Smith P, Matsumoto K. Lasers in endodontics: a review. Int Endod J 2000;33:173–85.
Mohammadi Z. Laser applications in endodontics: an update review. Int Dent J 2009;59:35–46.
Correa-Afonso AM, Pécora JD, Palma-Dibb RG. Influence of pulse repetition rate on temperature rise and working time during composite filling removal with the Er:YAG laser. Photomed Laser Surg 2008;26:221–5.
Versiani MA, Pécora JD, Sousa-Neto MD. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int Endod J 2013;46: 800–7.
Cohen J. Statistical Power and Analysis for the Behavioral Sciences, 2nd ed. Hillsdale, NJ: Lawrence Erlbaum Associates; 1988.
American Association of Endodontists: AAE Position Statement on Use Lasers in Dentistry. Chicago: AAE; 2012