Oval-shaped canal retreatment with self-adjusting file: a micro-computed tomography study
Abstract
Objectives: The aim of this study was to assess the efficacy of removing the filling material from oval-shaped canals with rotary retreatment files, with or without the additional use of self-adjusting file (SAF), using micro-computed tomography.
Materials and methods: Oval-shaped canals from 20 maxillary premolars were prepared and assigned to two groups (n =10), according to the obturation technique: cold lateral condensation (CLC) or vertical condensation (VC). Then, retreatment procedure was performed with retreatment rotary instruments followed by SAF. The specimens were scanned after each procedure and the volume of the filling material calculated. Median and interquartile range (IQR) percentages of the remaining filling material after each retreatment technique were statistically compared by Wilcoxon and Mann–Whitney U tests with a significance level of 5 %.
Results: The median percentage volume of the filling residue after rotary retreatment procedure was 1.59 (IQR=1.26) and 0.42 (IQR=0.86) in the CLC and VC groups, respectively (p <0.05). After the use of SAF, the median percentage was 1.26 (IQR=0.75) and 0.12 (IQR=0.53) in the CLC and VC groups, respectively (p <0.05). Statistically significant difference was also observed within the group after the additional use of SAF (p <0.05).
Conclusions: None of the retreatment procedures completely removed the filling material. The additional use of the SAF improved the removal of filling material after the retreatment procedure with rotary instruments.
Clinical relevance: Filling material left after retreatment procedure may harbour necrotic tissue and bacteria, which could lead to a persistent disease and reinfection of the root canal system. The additional use of self-adjusting file after the conventional retreatment procedures may improve root canal cleanliness, allowing a better action of the irrigating solution.
Introduction
The primary goals of endodontic treatment are to debride and disinfect the root canal space to the greatest possible extent, and to seal the canals as effectively as possible, aiming to establish or maintain healthy periapical tissues. Although initial root canal therapy has been shown to be a predictable procedure with a high degree of success, failure can occur. Lack of healing is attributed to persistent intraradicular infection residing in uninstrumented canals, dentinal tubules, or in the complex irregularities of the root canal system.
Previously treated teeth with persistent infection might be preserved with nonsurgical retreatment, which attempts to re-establish healthy periapical tissues by regaining access to the root canal system through removal of the original obturation, further cleaning, and re-filling. Many techniques have been advocated for the removal of filling material in root canal-treated teeth. Traditionally, root canal retreatment has been accomplished using solvent and hand files, and recently, this procedure has been replaced using rotary nickel– titanium (NiTi) files specially designed for retreatment procedures. Nevertheless, despite the development of new instruments and devices, none of them could render a root canal system completely free of root filling residue.
In oval-shaped canals, rotary files have failed to perform adequate cleaning and shaping, leaving untouched fins or recesses on the buccal and/or lingual aspects of the central canal area prepared by the instrument. Other untoward effect of root canal preparation with rotary files is the accumulation of debris in canal fins, isthmuses, and ramifications which might compromise the quality of root filling. In such cases, even warm gutta-percha obturation methods will fail to adequately seal the root canal. The self-adjusting file system (SAF; ReDent-Nova, Ra’anana, Israel) has been suggested to eliminate some of the limitations of rotary instruments because of its scraping motion with simultaneous irrigation and its ability to touch a higher percentage of root canal walls. In this way, the SAF is expected to be effective as a second stage in a two-stage procedure for removing remaining root filling material.
Most of earlier ex vivo studies used destructive and two-dimensional methods to determine the amount of remaining filling material after retreatment procedure. However, these methods were not able to precisely evaluate the volume of remaining filling material after the retreatment procedures. In contrast, the non-destructive and non- invasive technique of micro-computed tomography allows the reconstruction and volumetric evaluation of tooth tissues as well as the root canal filling materials, overcoming the limitations of the conventional methods. Thus, the aim of this paper was to assess the efficacy of removing the filling material from oval-shaped canals with rotary retreatment files, with or without the additional use of SAF, using micro-computed tomography (μCT). The null hypothesis was that there is no difference in the percentage of remaining filling residues after the retreatment procedure with or without the additional use of SAF.
Materials and methods
Sample selection
After ethics committee approval (protocol #218/2012), 60 straight one-rooted maxillary premolars with fully formed apices were selected from a pool of extracted teeth, decoronated slightly above the cementoenamel junction, and stored in labelled individual plastic vials containing 0.1 % thymol solution. Teeth were extracted for reasons not related to this study and initially selected on the basis of radiographs taken in both bucco-lingual and mesio-distal directions to detect any possible root canal obstruction. In order to attain an overall outline of internal anatomy as well as the calculation of volume and surface area of the root canals, these teeth were pre-scanned at a resolution of 68 μm using a μCT scanner (SkyScan 1172; Bruker-microCT, Kontich, Belgium) at 90 kV and 112 μA. Axial cross sections of the inner structure of the samples were acquired after reconstruction procedure (NRecon v.1.6.3 software; Bruker-microCT) and, based on a slice-by-slice assessment taking the root apex as a reference point, the slices at 5- and 8-mm coronal of the apex were determined and the root canal at those levels outlined. The minimum and maximum diameters of the root canal were measured mesio-distally and bucco-lingually, respectively, using DataViewer v.1.4.4 soft- ware (Bruker-microCT). Based on these pre-scans set of images, 28 premolars with a canal ratio of long to short diameter of more than 2, at 5-mm level, and 3, at 8-mm level, were selected. All teeth presenting isthmus, apical curvature, or more than one root canal were excluded.
The specimens were then pair-matched on the basis of the three-dimensional morphological dimensions and anatomical configuration of the root canal system. One specimen from each pair was randomly assigned to one of the two experimental groups (n =10). After checking for normality assumption (Shapiro-Wilk test), the degree of homogeneity (baseline) of the two groups, with respect to the volume and surface area of the root canal, was assessed using Student t test, with a confidence level set at 5 %.
Root canal preparation
After being washed in running water for 24 h, apical patency was determined by inserting a size 10 K-file into the root canal until its tip was visible at the apical foramen, and the working length (WL) was set 1.0 mm short of this measurement. The root canals were serially enlarged with Revo-S NiTi rotary (Micro-Mega, Besançon, France) instruments. This system is composed of two instruments for apical penetration (SC1 and SC2), and a recapitulating and cleaning instrument (SU). These instruments were used in a crown-down manner up to the WL resulting in an apical third shaped to a size 25, 0.06 taper. Then, the sequence was completed using apical preparation instruments (AS 30, 35, and 40) up to the WL. Apical enlargement was finished by hand with a size 45 K-File (Mani Co, Tokyo, Japan). To avoid fracture, two canals were pre- pared with one set of instruments which were driven using a torque-controlled motor (W&H, Bürmoos, Austria) set to 300 rpm using a gentle in-and-out motion. The instruments were withdrawn when resistance was felt and changed for the next instrument. During preparation procedure, the canals were flushed with 2 mL of 5 % NaOCl between each instrument, delivered in a syringe with a 30-gauge needle placed 1 mm short of the WL. In addition, to achieve a degree of uniformity and reduce interoperator variables, all procedures were conducted by the same operator. After preparation, a final rinse with 2 mL of saline solution was performed, and the root canals were dried with paper points.
Root canal filling
A flip of a coin was used to define which of the experimental groups (n =10) would be treated with each of the following root canal filling techniques: cold lateral condensation (CLC) or vertical condensation (VC).
For all specimens, a size 40, 0.02 taper K-file (Mani, Inc., Tochigi, Japan) was used to place AH Plus sealer (Dentsply De Trey GmbH, Konstanz, Germany) at large amount into the root canal. In the CLC group, a prefitted size 45, 0.02 taper gutta-percha cone (Diadent Group International, Chongchong Buk Do, Korea) was inserted into the full working length. Lateral compaction was achieved using size F accessory gutta-percha cones (Diadent Group International) until a size 25 finger spreader (VDW, Antaeos, Munich, Germany) could penetrate no more than 3 mm into the canal. A heated instrument was used to cut the coronal surplus, after which the filling was vertically compacted. In the VC group, thermoplasticized gutta-percha was injected into the canal in small increments using the Dia-Gun Obturation System (North Fraser Way, Burnaby, BC, Canada). Pressure with an adequate plugger (Medesy SRL, Maniago, Italy) was performed to compact the gutta-percha apically and into the canal irregularities. The roots were radiographed in both bucco-lingual and mesiodistal directions to confirm the adequacy of the filling. If voids were observed in the obturation mass, the specimen was replaced. The samples were then stored (37 °C, 100 % humidity) for 3 weeks to allow the complete setting of the sealer.
μCT evaluation
Each tooth was slightly dried, mounted on a custom attachment, and the analysis of the filling materials undertaken using a μCT system (SkyScan 1172; Bruker-microCT, Kontich, Belgium). The lengths of the teeth were scanned at 90 kV, 112 μA, at an isotropic pixel size of 12.5 μm resulting in the acquisition of 900–1,100 transverse cross sections per tooth. The scanning was performed by 180° rotation around the vertical axis; camera exposure time of 2,600 ms, rotation step of 0.6°, frame averaging of 2 and medium filtering of the data were applied. X-rays were filtered with 500-μm aluminium and a 38-μm-thick copper filter. A flat field correction was taken on the day, prior to scanning to correct for variations in the pixel sensitivity of the camera. Images were reconstructed using NRecon v.1.6.3 (Bruker-microCT) with a beam hardening correction of 15 %, smoothing of 3, no ring artefact correction, and an attenuation co-efficient range of −0.002 to 0.15, providing axial cross sections of the inner structure of the samples.
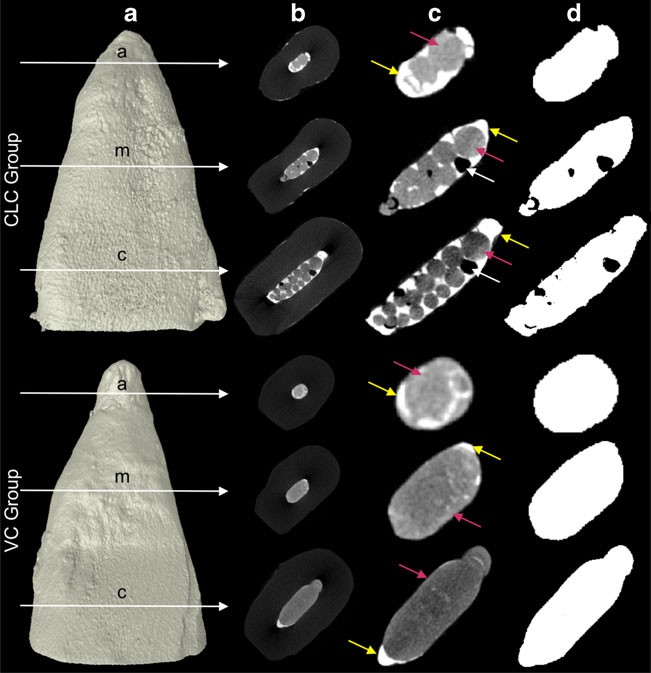
For the calculation of the volume (mm3) and surface representations of the filling materials, the original grayscale images were processed with a slight Gaussian low-pass filtration for noise reduction, and an automatic segmentation threshold was used to separate root dentine from the filling materials, using CTAn v.1.12 software (Bruker-microCT). This process entails choosing the range of grey levels necessary to obtain an image composed only of black and white pixels. The high contrast of the filling materials to the dentine yielded excellent segmentation of the specimens (Fig. 1). Separately and for each slice, regions of interest were chosen to allow the calculation of the volume (in mm3) of the filling materials. Then, a polygonal surface representation was constructed. CTVol v.2.2.1 software (Bruker-microCT) was used for visualization and qualitative evaluation of the root canal filling.
Root canal retreatment
R-Endo retreatment rotary instruments (Micro-Mega, Besançon, France) were used with a rotary electric motor (W&H, Bürmoos, Austria) in a gentle in-and-out motion at 340 rpm with circumferential filing action. R-Endo Re NiTi rotary instrument (size 25, 0.12 taper) was used up to 3 mm beyond the canal entrance, followed by R1 instrument (size 25, 0.08 taper) to the beginning of the middle third. Then, R2 (size 25, 0.06 taper) were used to the end of the middle third and R3 (size 25, 0.04 taper) up to the working length. The canals were irrigated after each instrument with 2.5 mL of 5 % NaOCl. The instruments were replaced after five canals, and retreatment procedure was considered completed when the working length was reached, no material was observed between the flutes of the files, and the irrigating solution appeared clear of debris. After the retreatment procedure, the canals were gently dried with paper points and the specimens submitted to the μCT evaluation applying the aforementioned parameter settings.
Then, a 2.0-mm-diameter SAF (ReDent-Nova) was operated for 2 min using a vibrating handpiece RDT3-NX head (ReDent-Nova) adapted with a low speed handpiece (NSK, Tokyo, Japan) at a frequency of 83.3 Hz (5,000 rpm) and amplitude of 0.4 mm. The instrument was used with a manual in-and-out motion to the WL. Continuous irrigation at a flow rate of 5 mL/min with 15 % EDTA for 1 min followed by 5 % NaOCl for 1 min was applied throughout the procedure using a special irrigation apparatus (VATEA; ReDent-Nova). Then, the canals were dried with paper points and the specimens submitted to a final μCT scanning.
The percentage of filling material left in the root canal was calculated according to the following formula: V B×100/VA, where VB and VA mean the volume (in mm3) of the filling material before and after the retreatment procedure, respectively.
Statistical analysis
The volume of the filling materials after the obturation procedure was expressed in cubic millimetres. Considering that these data were normally distributed (Shapiro-Wilk test; p >0.05), they were presented as means and standard deviations and statistically compared using Student t test. The remaining filling materials after the retreatment procedures were expressed as a percentage of the total initial root filling volume. Because normality assumptions could not be verified (Shapiro-Wilk test; p <0.05), percentage of filling material left in the root canal was presented as median values and interquartile ranges (IQR). Statistical analysis was performed using the Wilcoxon test within group and Mann–Whitney U test between groups, with a significance level of 5 % (SPSS v11.0 for Windows; SPSS Inc., Chicago, IL, USA).
Results
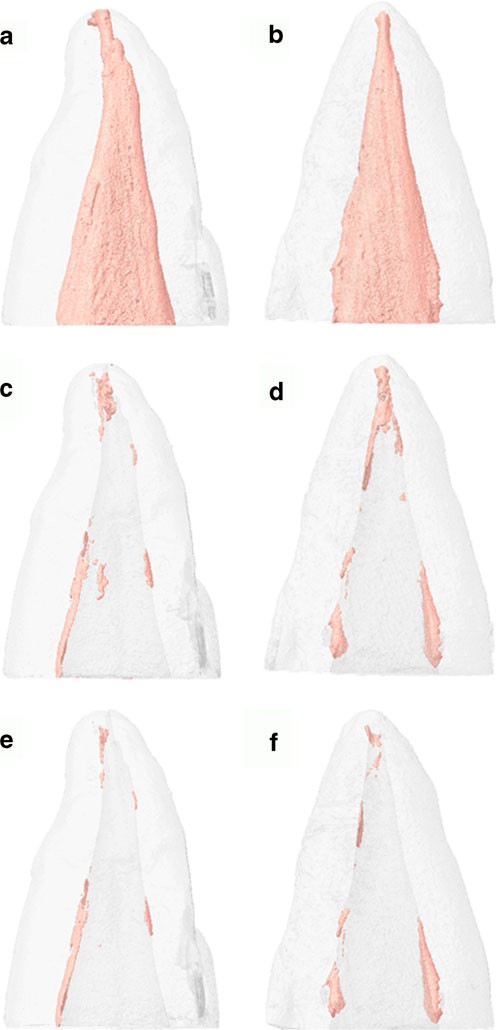
No statistical difference was observed between the mean volume of the filling materials in the CLC (18.28±4.11 mm3) and VC (17.48±3.85 mm3) groups before the retreatment procedures (p >0.05). None of the retreatment procedures used in this study completely removed the filling material from root canals, except in one specimen in the CLC group after the additional use of SAF. Overall, filling residues were located mainly into root canal irregularities, fins and recesses after the retreatment procedures (Fig. 2).
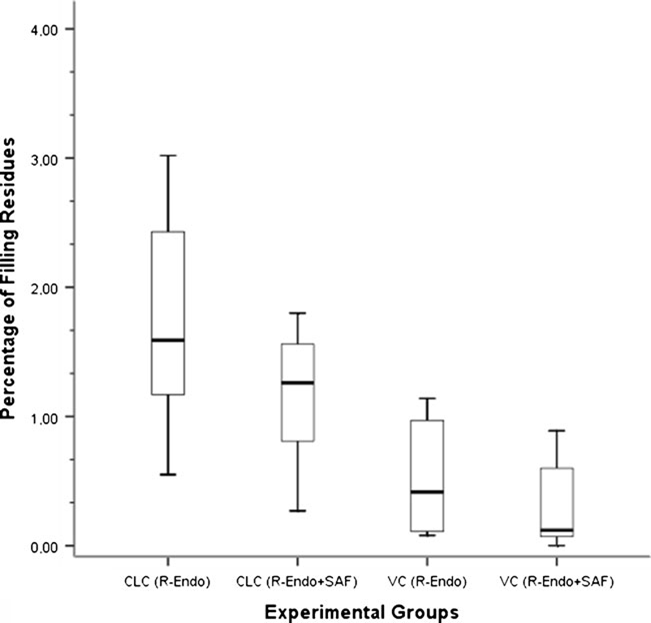
The median percentage volume of the filling residue after R-Endo retreatment procedure was 1.59 (IQR=1.26) and 0.42 (IQR=0.86) in the CLC and VC groups, respectively (p <0.05). Among the specimens in the VC group, 60 % presented with root filling residue less than 0.5 % of the original root filling volume (ranging from 0.08 to 1.14 %), whilst in CLC group the percentage of filling residue ranged from 0.55 to 3.02 %.
After the use of SAF, the median percentage volume of the filling residue was 1.26 (IQR=0.75) and 0.12 (IQR=0.53) in the CLC and VC groups, respectively, with statistically significant difference (p <0.05). Among the specimens in the VC group, 70 % presented with root filling residue less than 0.5 % of the original root filling volume (ranging from 0 to 0.89 %). In the CLC group, the percentage of filling residue ranged from 0.27 to 1.80 %, with only one specimen presenting residue less than 0.5 % of the original filling volume.
Statistical difference was also observed within group after the additional use of SAF (p <0.05) (Fig. 3). Considering that the additional use of SAF significantly improved the removal of filling material after the retreatment procedure with R-Endo instruments, the null hypothesis was rejected.
Discussion
The first attempts to use rotary NiTi files in retreatment procedures have led to the development of a more efficient way to remove the bulk of the filling material in comparison with manual techniques. Unfortunately, several reports have indicated that substantial amounts of root canal filling material still remain in the canal after retreatment procedures using mechanized methods, with or without the additional use of a solvent. In contrast to the clinical situation, in the present study, no solvent was applied during the retreatment procedure with the purpose to eliminate a possible confounding factor.
Recently, new instruments specially designed for this purpose have been introduced, including the R-Endo retreatment files. According to the manufacturer, root canal retreatment using R-Endo system allows an efficient removal of the previous filling material. In the present study, the finding that root canal filling remnants were left in the canal after the first stage in which R-Endo retreatment files were used alone is not surprising and is consistent with the aforementioned studies. Considering the tip size of the R-Endo instruments (size 25) and the enlargement of the canal up to size 45, it could not have been expected that these instruments would be able to remove all of the filling material from the root canal, even if used in a circumferential motion.
The recent introduction of SAF system has offered a new potential approach to the later stages of root canal filling removal. SAF is supposed to adapt to the cross section of the canal and to have a scrubbing effect on the canal walls. In the present study, a 2.0-mm- diameter instrument was selected because it was previously demonstrated that SAF with a 1.5-mm diameter was less effective in large canals. Although SAF cannot be considered as an instrument capable of removing the bulk of root filling material, in the present study, the supplementary use of SAF resulted in a significant reduction in the amount of root canal filling residue left after using R-Endo instruments.
The present results may be compared with those reported recently. Abramovitz et al. and Voet et al. evaluated the efficacy of a two-stage procedure in which the SAF file was used to remove the remaining root filling material after the application of ProTaper retreatment files in curved canals of mandibular and maxillary molars, respectively. Both studies have found that the use of the SAF after rotary instruments resulted in a significant reduction in the amount of filling residue. However, these studies used two-dimensional analyses (radiograph and root sectioning, respectively) which do not allow calculation of the volume of remaining gutta-percha, if compared with a three-dimensional evaluation using μCT technology. Similarly, using μCT to compare the efficacy of removing filling material with ProTaper retreatment files, or with a size 25, 0.06 taper ProFile instrument followed by the use of SAF, Solomonov et al. have found that the later left significantly less root filling residue, which is in agreement with this study.
The present results also revealed significant lower percentage of remaining filling material in the specimens of VC group compared with CLC group. It may be explained because of the higher bond strength of the filling materials to root dentine observed in root canals obturated using lateral compaction with AH Plus and gutta-percha cones, which makes the removal of the filling residues more difficult. In the lateral compaction technique, the gutta-percha is not mixed with the sealer, which remains in direct contact with the dentine (Fig. 1c). Then, AH Plus sealer would be able to penetrate deeper into the micro-irregularities owing to its flowability and long polymerization time, contributing to enhance the mechanical interlocking between sealer and dentine. In addition, the cohesion amongst the sealer molecules increases the resistance to displacement of the material from dentine surfaces, which is translated into greater adhesion and may explain the present results.
On the other hand, the use of a thermomechanical compaction technique resulted in a nonhomogenous mixture, suggesting that the plasticized solid filling material penetrated into the sealer, forming a non-uniform structure (Fig. 1c). Scanning electron microscopy studies have also demonstrated that, upon cooling, the solid material shrinks and pulls the sealer, leaving craters that may contribute to weaken the adhesive interface. Moreover, heating AH Plus sealer can accelerate the polymerization, reducing its flow rate. Therefore, it may be speculated that penetration of thermoplasticized gutta-percha into the canal micro-irregularities and dentinal tubules promotes only mechanical interlocking because gutta-percha without sealer probably results in lower adhesion.
Whilst in straight canals with a round cross-section the operator may simply use rotary files of greater dimensions to remove the residues, the retreatment of oval-shaped canals is still a challenge. Besides, the further enlargement of oval canals using larger files may create complications such as perforation or transportation. In this type of root canal anatomy, the use of SAF may be considered as a safe supplementary procedure to improve the removal of remnants from the root canals.
Under the limitations of this ex vivo study, neither retreatment protocols were able to render all canals free of root filling remnant. However, the additional use of SAF improved the removal of filling material from oval-shaped canals after the retreatment procedure with R-Endo instruments.
Authors: Ali Keleş, Hatice Alcin, Aliye Kamalak, Marco A. Versiani
References:
- Siqueira JF Jr (2005) Reaction of periradicular tissues to root canal treatment: benefits and drawbacks. Endod Topics 10:123–147. doi:10.1111/j.1601-1546.2005.00134.x
- Torabinejad M, Corr R, Handysides R, Shabahang S (2009) Outcomes of nonsurgical retreatment and endodontic surgery: a systematic review. J Endod 35:930–937. doi:10.1016/j.joen.2009.04.023
- Horvath SD, Altenburger MJ, Naumann M, Wolkewitz M, Schirrmeister JF (2009) Cleanliness of dentinal tubules following gutta-percha removal with and without solvents: a scanning electron microscopic study. Int Endod J 42:1032–1038. doi:10.1111/j.1365- 2591.2009.01616.x
- Friedman S, Stabholz A, Tamse A (1990) Endodontic retreatment - case selection and technique. 3. Retreatment techniques. J Endod 16:543–549. doi:10.1016/S0099-2399(07)80219-6
- Abramovitz I, Relles-Bonar S, Baransi B, Kfir A (2012) The effectiveness of a self-adjusting file to remove residual gutta-percha after retreatment with rotary files. Int Endod J 45:386–392. doi:10.1111/j. 1365-2591.2011.01988.x
- Somma F, Cammarota G, Plotino G, Grande N, Pameijer C (2008) The effectiveness of manual and mechanical instrumentation for the retreatment of three different root canal filling materials. J Endod 34:466–469. doi:10.1016/j.joen.2008.02.008
- Zmener O, Pameijer CH, Banegas G (2006) Retreatment efficacy of hand versus automated instrumentation in oval-shaped root canals: an ex vivo study. Int Endod J 39:521–526. doi:10.1111/j.1365-2591. 2006.01100.x
- Solomonov M, Paqué F, Kaya S, Adiguzel O, Kfir A, Yigit-Ozer S (2012) Self-adjusting files in retreatment: a high-resolution micro- computed tomography study. J Endod 38:1283–1287. doi:10.1016/j. joen.2012.06.019
- Taşdemir T, Er K, Yildirim T, Çelik D (2008) Efficacy of three rotary NiTi instruments in removing gutta-percha from root canals. Int Endod J 41:191–196. doi:10.1111/j.1365-2591.2007.01335.x
- Voet KC, Wu MK, Wesselink PR, Shemesh H (2012) Removal of gutta-percha from root canals using the self-adjusting file. J Endod 38:1004–1006. doi:10.1016/j.joen.2012.03.003
- Rechenberg DK, Paqué F (2013) Impact of cross-sectional root canal shape on filled canal volume and remaining root filling material after retreatment. Int Endod J 46:547–555. doi:10.1111/iej.12027
- Paqué F, Peters OA (2011) Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the self-adjusting file. J Endod 37:517–521. doi:10.1016/j.joen.2010.12.011
- Versiani MA, Pécora JD, Sousa-Neto MD (2011) Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 37:1002–1007. doi:10.1016/j.joen.2011.03.017
- Wu MK, Wesselink PR (2001) A primary observation on the prepa- ration and obturation of oval canals. Int Endod J 34:137–141. doi:10. 1046/j.1365-2591.2001.00361.x
- Ribeiro MVM, Silva-Sousa YT, Versiani MA, Lamira A, Steier L, Pécora JD, Sousa-Neto MD (2013) Comparison of the cleaning efficacy of self-adjusting file (SAF) and rotary systems in the apical third of oval-shaped canals. J Endod 39:398–410. doi:10.1016/j.joen. 2012.11.016
- Robinson JP, Lumley PJ, Claridge E, Cooper PR, Grover LM, Williams RL, Walmsley AD (2012) An analytical micro CT methodology for quantifying inorganic dentine debris following internal tooth preparation. J Dent 40:999–1005. doi:10.1016/j.jdent.2012.08. 007
- Metzger Z, Zary R, Cohen R, Teperovich E, Paqué F (2010) The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. J Endod 36:1569–1573. doi:10.1016/j.joen.2010.06.003
- Versiani MA, Pécora JD, de Sousa-Neto MD (2012) Root and root canal morphology of four-rooted maxillary second molars: a micro- computed tomography study. J Endod 38:977–982. doi:10.1016/j. joen.2012.03.026
- De-Deus G, Di Giorgi K, Fidel S, Fidel RAS, Paciornik S (2009) Push-out bond strength of Resilon/Epiphany and Resilon/Epiphany self-Etch to root dentin. J Endod 35:1048–1050. doi:10.1016/j.joen. 2009.04.024
- Carneiro SM, Sousa-Neto MD, Rached FA Jr, Miranda CE, Silva SR, Silva-Sousa YT (2013) Push-out strength of root fillings with or without thermomechanical compaction. Int Endod J 45:821–828. doi:10.1111/j.1365-2591.2012.02039.x
- Resende LM, Rached-Junior FJA, Versiani MA, Souza-Gabriel AE, Miranda CES, Silva-Sousa YTC, Sousa Neto MD (2009) A comparative study of physicochemical properties of AH Plus, Epiphany, and Epiphany SE root canal sealers. Int Endod J 42:785–793. doi:10. 1111/j.1365-2591.2009.01584.x
- Sousa-Neto MD, Silva Coelho FI, Marchesan MA, Alfredo E, Silva- Sousa YT (2005) Ex vivo study of the adhesion of an epoxy-based sealer to human dentine submitted to irradiation with Er : YAG and Nd : YAG lasers. Int Endod J 38:866–870. doi:10.1111/j.1365-2591. 2005.01027.x
- Tay FR, Loushine RJ, Lambrechts P, Weller RN, Pashley DH (2005) Geometric factors affecting dentin bonding in root canals: a theoretical modeling approach. J Endod 31:584–589. doi:10.1097/01.don. 0000168891.23486.de