
Root canal morphology of primary molars: a micro-computed tomography study
Abstract
Aim: This was to investigate the root canal morphology of primary molar teeth using micro-computed tomography.
Methods: Primary maxillary (n = 20) and mandibular (n = 20) molars were scanned at a resolution of 16.7 lm and analysed regarding the number, location, volume, area, structured model index (SMI), area, roundness, diameters, and length of canals, as well as the thickness of dentine in the apical third. Data were statistically compared by using paired-sample t test, independent sample t test, and one-way analysis of variance with significance level set as 5 %.
Results: Overall, no statistical differences were found between the canals with respect to length, SMI, dentine thickness, area, roundness, and diameter (p ˃ 0.05). A double canal system was observed in the mesial and mesiobuccal roots of the mandibular and maxillary molars, respectively. The thickness in the internal aspect of the roots was lower than in the external aspect. Cross-sectional evaluation of the roots in the apical third showed flat-shaped canals in the mandibular molars and ribbon- and oval-shaped canals in the maxillary molars.
Conclusions: External and internal anatomy of the primary first molars closely resemble the primary second molars. The reported data may help clinicians to obtain a thorough understanding of the morphological variations of root canals in primary molars to overcome problems related to shaping and cleaning procedures, allowing appropriate management strategies for root canal treatment.
Introduction
The premature loss of primary teeth may cause changes in the chronology and sequence of eruption of permanent teeth; thus, saving teeth in children is an important concept and frequently involves endodontic treatment (Cleghorn et al. 2012). Root canal treatment in primary teeth includes the removal of the pulp tissue, debridement and preparation, irrigation, and filling of the canals. The main objective of pulp therapy in primary teeth is to maintain the integrity and health of the teeth and their supporting tissues (Cleghorn et al. 2012). To accomplish this goal, a comprehensive understanding of the root and the root canal morphology of primary teeth is of utmost importance (Hibbard and Ireland 1957; Goodacre 2003; Zoremchhingi et al. 2005; Aminabadi et al. 2008; Bagherian et al. 2010; Cleghorn et al. 2012).
The external and internal morphology of primary teeth are different in many aspects from permanent successors (Kavanagh and O’Sullivan 1998; Goodacre 2003; Johnston and Franklin 2006; Cleghorn et al. 2012). Generally, primary teeth with fully developed roots exhibit a less complex root canal system compared to permanent teeth, with one canal per root. In primary molars, the complexity of this system may increase over time due to the formation of secondary dentine and narrowing of the canal system and eventually the resorption process (Hibbard and Ireland 1957).
Traditionally, root canal anatomy of primary teeth has been described in case reports (Badger 1982; Falk and Bowers 1983; Caceda et al. 1994; Winkler and Ahmad 1997; Kavanagh and O’Sullivan 1998; Eden et al. 2002) and in ex vivo studies using injection of materials (Simpson 1973), dye perfusion (Ringelstein and Seow 1989), digital radiographs, longitudinal and transverse cross-sectioning, histology (Poornima 2008), clearing technique (Bagherian et al. 2010), scanning electron microscope (Wrbas et al. 1997), and conventional computed tomography (Zoremchhingi et al. 2005). These methodologies have been successfully used for many years in the anatomical study of the root canal system; however, most of them are invasive or only provide a two-dimensional image of a three-dimensional structure, and therefore may not accurately reflect the morphology of the object being studied. Thus, these inherent methodological limitations encouraged the search for new methods able to produce improved results (Peters et al. 2000).
In recent years, significant technological advances for imaging teeth have been introduced. Their non-invasive nature allows the use of teeth for other purposes or as controls for further treatment procedures. The development of the high-resolution X-ray micro-computed tomography (micro-CT) has gained increasing significance in the study of dental tissues. Micro-CT offers a non-invasive reproducible technique for three-dimensional assessment of the root canal system and it can be applied both quantitatively and qualitatively (Peters et al. 2000; Siqueira et al. 2010; Versiani et al. 2011, 2012, 2013).
Even though there has been a growing body of research and publications on the dental anatomy of primary teeth (Goodacre 2003; Cleghorn et al. 2012), a detailed quantitative description of the anatomy of their root canal system is still lacking. Therefore, the purpose of this study was to describe the morphometric aspects of the external and internal anatomy of primary mandibular and maxillary molars, using high-resolution three-dimensional micro-CT analysis.
Materials and methods
Sample selection
After approval from the local ethics in research committee (CAAE #0072.0.130.000-09), primary mandibular (n = 20) and maxillary (n = 20) molars, extracted for reasons not related to this study and stored in 0.1 % thymol solution, were selected. For each group of teeth, ten first and ten second primary molars were evaluated. The inclusion criteria comprised only molars with no physiological root resorption or at its initial stages, i.e. in which resorption did not exceed 1/3 of root length.
Micro-CT scanning and reconstruction
Each tooth was slightly dried, mounted on a custom attachment, and scanned in a micro-CT scanner (SkyScan 1174v2; Bruker-microCT, Kontich, Belgium) at an isotropic resolution of 16.7 lm. The X-ray tube was operated at 50 kV and 800 mA, and the scanning was performed by 180° rotation around the vertical axis with a rotation step of 1°, using a 0.5-mm-thick aluminium filter. Images of each specimen were reconstructed with dedicated software (NRecon v.1.6.6; Bruker-microCT) providing axial cross sections of the inner structure of the samples.
Quantitative analysis
DataViewer v.1.4.4 software (Bruker-microCT) was used to evaluate the length (in millimetres) of the root from the apex, and the length of the main root canals from the apical foramen to the level of the cementoenamel junction. Three-dimensional evaluation of the root canals (volume, surface area, and structure model index) was performed from the apex to the canal orifice using CTAn v.1.12 software (Bruker-microCT). Volume was calculated as that of binarised objects within the volume of interest. For the measurement of the surface area of the 3D multilayer dataset, two components to surface measured in 2D were used: first, the perimeters of the binarised objects on each cross-sectional level, and second, the vertical surfaces exposed by pixel differences between adjacent cross sections. Structure model index (SMI) involves a measurement of surface convexity in a 3D structure. SMI is derived as 6.(S’.V)/S2), where S is the object surface area before dilation and S’ is the change in surface area caused by dilation. V is the initial, undilated object volume. An ideal plate, cylinder and sphere have SMI values of 0, 3 and 4, respectively (Peters et al. 2000).
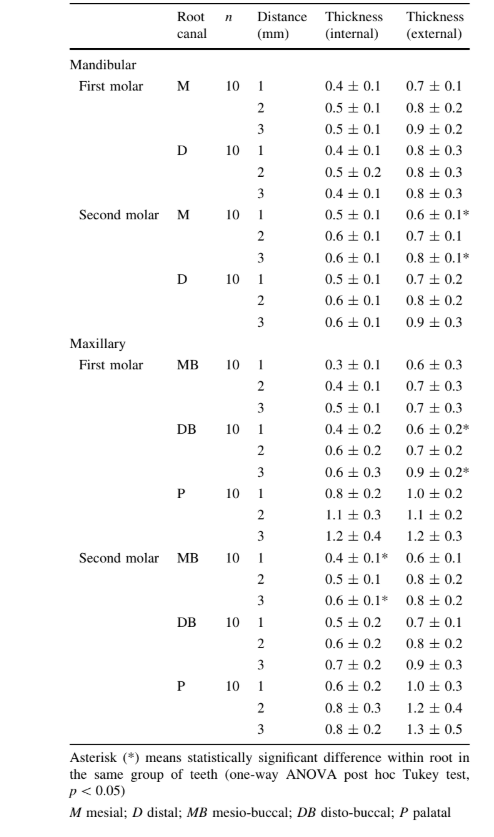
The smallest thickness of dentine in the internal and external aspects of the roots, at 1, 2 and 3 mm from the apical resorption bevel, were also recorded. Measurements of the dentine thickness were taken from the external limit of the root canal to the surface of the root. At these same levels, CTAn v.1.12 software (Bruker-microCT) was used for the two-dimensional evaluation (area, roundness, major diameter, and minor diameter) of the root canal. Area was calculated using the Pratt algorithm (Pratt 1991). The cross-sectional appearance, round or more ribbon shaped, was expressed as roundness. Roundness of a discreet 2D object is defined as 4A/(p.(dmax)2), where ‘‘A’’ is the area and ‘‘dmax’’ is the major diameter. The value of roundness ranges from 0 to 1, with one signifying a circle. The major diameter was defined as the distance between the two most distant pixels in that object. The minor diameter was defined as the longest chord through the object that can be drawn in the direction orthogonal to that of the major diameter.
Qualitative analysis
Three-dimensional models and cross sections of the root canals were reconstructed based on micro-CT scans and generated by the binarisation process using CTAn v.1.12 software (Bruker-microCT). CTVol v.2.2.1 (Bruker-microCT) and DataViewer v.1.4.4 (Bruker-microCT) software were used for visualisation and qualitative evaluation of the specimens.
Statistical analysis
Three-dimensional parameter results and the average length of roots and root canals were statistically compared using paired-sample t test within group and independent sample t test between groups, respectively. Considering that the data of dentine thickness and two-dimensional parameters at 1, 2 and 3 mm from the resorption bevel were normally distributed (Shapiro–Wilk test; p ˃ 0.05), they were presented as means and standard deviations (SD), and statistically compared using one-way analysis of variance post hoc Tukey test. Statistical analysis was performed using SPSS v.17.0 for Windows (SPSS Inc, Chicago, IL, USA) with a significance level set at 5 %.
Results
Quantitative analysis
Tables 1 and 2 show the mean (±SD) of the three- and two-dimensional data, respectively, in each root of the primary molars. Overall, in both groups of teeth no statistical differences were found between root canals of the first and second molars with respect to length, SMI, and the two-dimensional analysed parameters (area, roundness, major diameter, and minor diameter) (p ˃ 0.05). Distal and palatal canals of the mandibular and maxillary molars, respectively, presented a significant higher volume than the other canals in the same group of teeth (p ˂ 0.05). Generally, root canals of the second primary molar canals had higher surface area than the first molars (p ˂ 0.05).
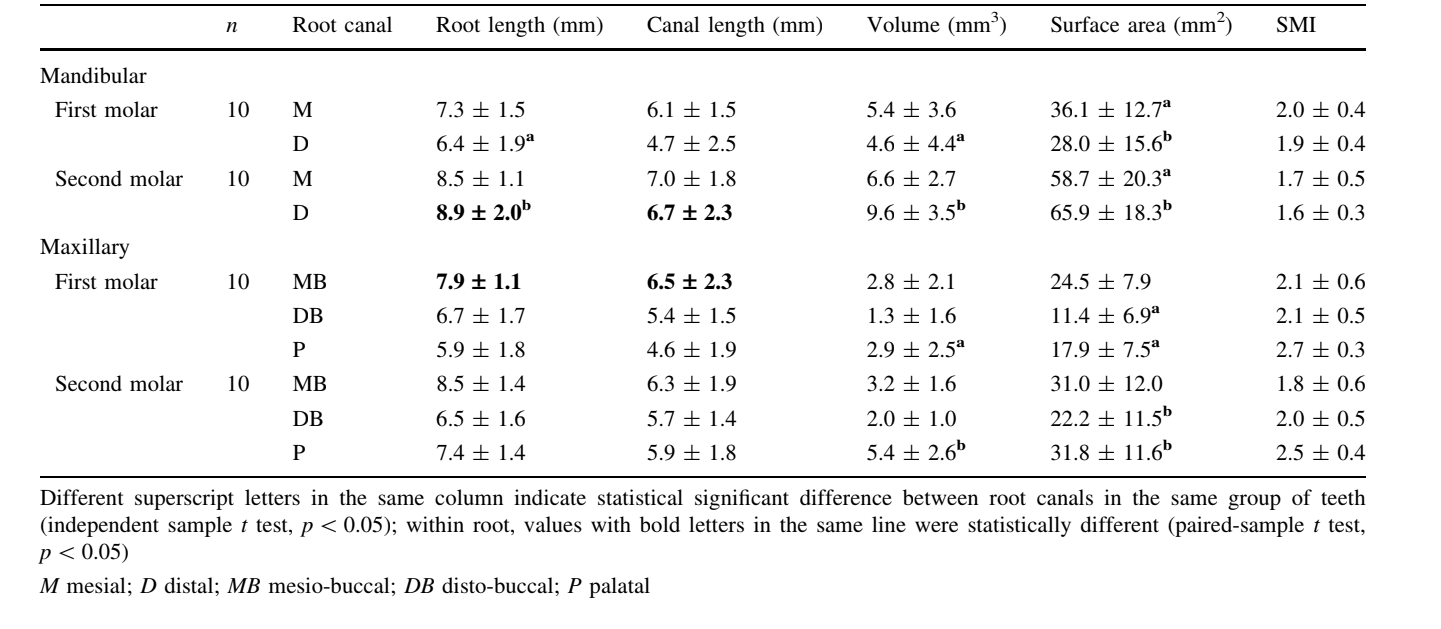
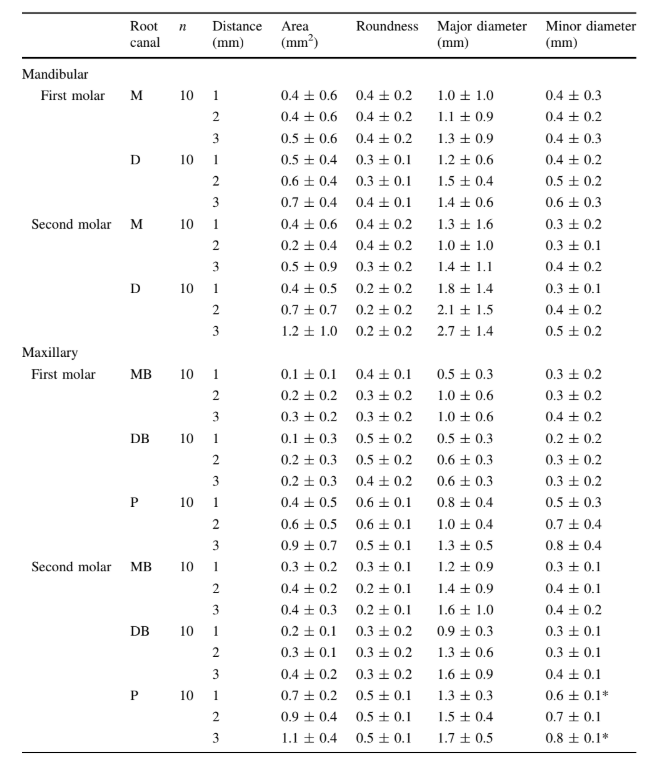
Table 3 summarises the mean dentine thickness in the apical third of each molar root. No statistical difference was observed in the comparison of the dentine thickness, in either internal or external aspect of each root, between the first and second molars (p ˃ 0.05). The lowest mean values of dentine thickness were observed in the internal aspect of the roots, in both molar groups. In general, the highest mean thickness of dentine was observed in the distal and palatal roots of the mandibular and maxillary molars, respectively, in all evaluated levels.
Qualitative analysis
The analysis of the external anatomy of the mandibular first and second molars showed that all specimens had two roots, wider in the buccal–lingual dimension, narrower mesio-distally, and often fluted. Deep caries with no pulp exposure were observed in 20% of the sample. Early apical root resorption was observed in only one specimen from each group of teeth. On the other hand, surface resorption at the internal aspect of the roots was observed in most of the teeth (n = 15). Bevelled resorption in the apex of both roots resulted in a thinner thickness of the dentine walls compared to the middle and cervical thirds. Three-dimensional models of the mandibular molars confirm that the configuration of the root canal system was consistent with the external morphology of the root (Fig. 1a–c). A single root canal was observed in 10 % of the mesial roots, while a single distal canal system was detected in 60 and 50 % of the first and second molars, respectively. In the mesial and distal roots, the maximum number of orifices observed in the root canal cross sections was 8 and 5, respectively. At the furcation level, the mesial root of the mandibular first molars showed two orifices in eight samples, whilst all other roots presented only one orifice. Ribbon-shaped canal systems with one or two canals in the mesial root and one in the distal root were present in 40 and 30 % of the first and second molars, respectively. In the latter, a ribbon-shaped canal that separates into two or more canals from below the cemento-enamel junction was also observed.
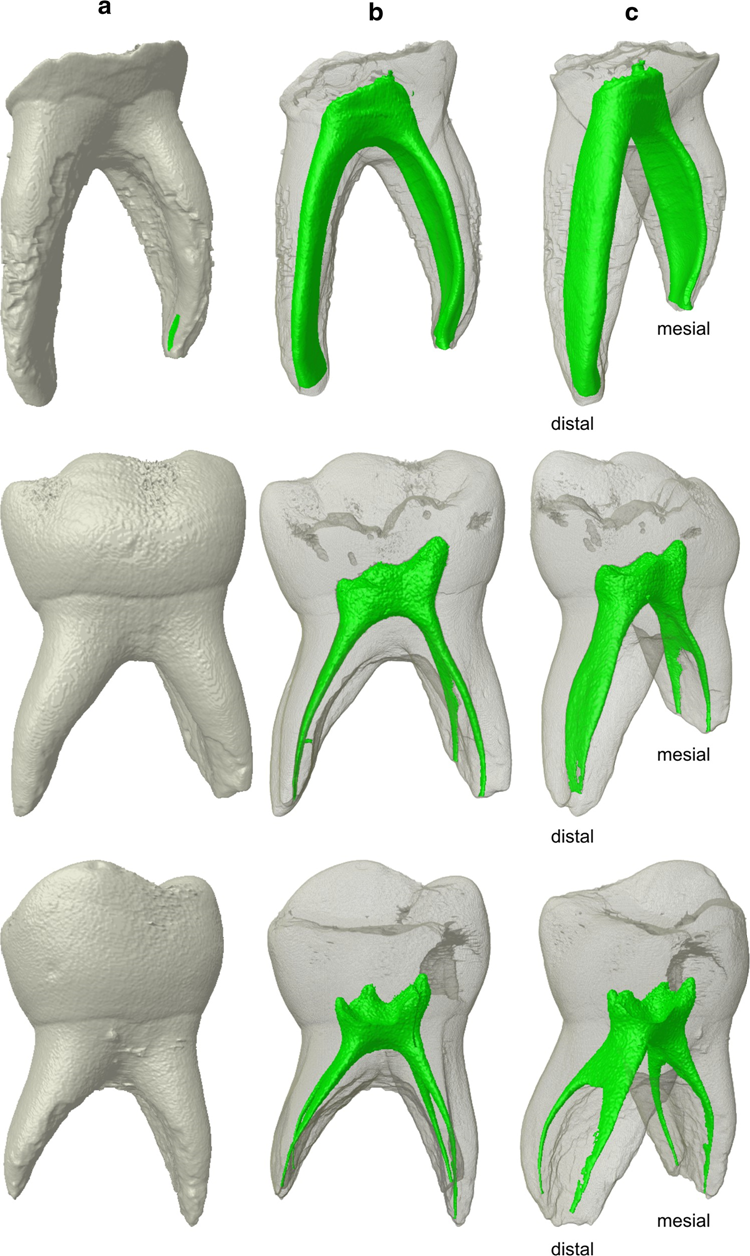
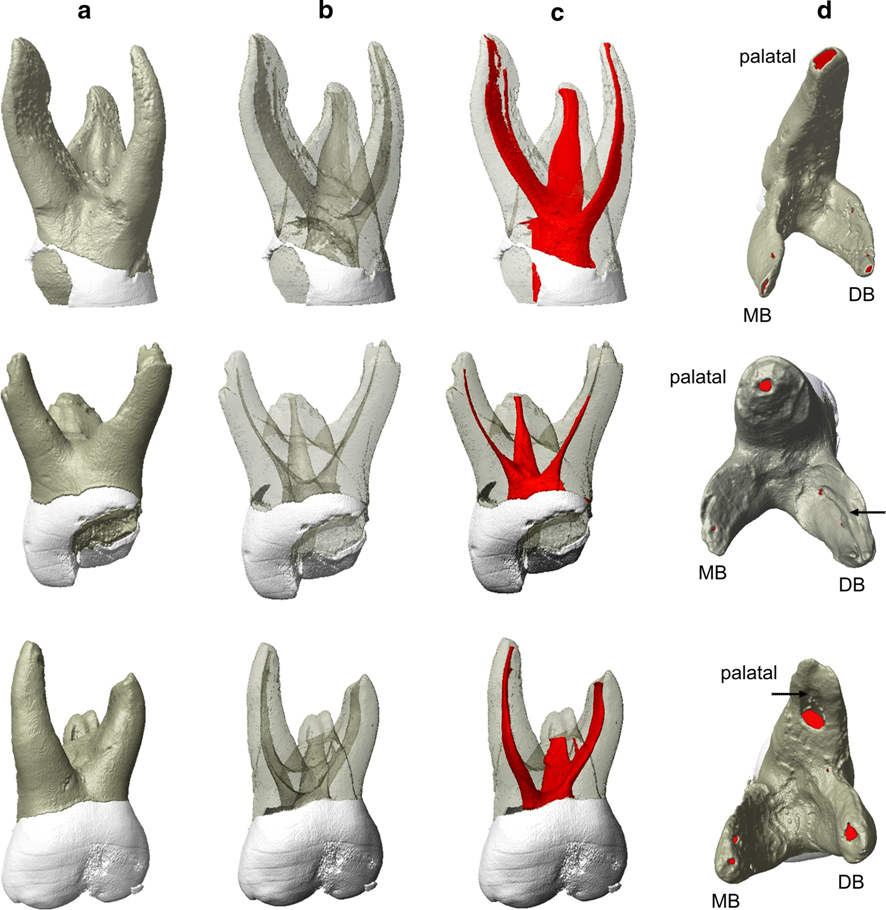
Figure 2 shows exemplary 3D models of the external (Fig. 2a) and internal anatomy (Fig. 2b–c) of three primary maxillary molars. Generally, three canal systems were present, one in each root. Two canals were observed in the mesio-buccal (MB) root of two maxillary first molars. At the furcation level, the MB root of the maxillary first molars showed two orifices in two samples, whilst all other roots presented only one orifice. The analysis of the external anatomy showed that six specimens from each group of teeth had three widely separated roots, while four presented fusion between the disto-buccal (DB) and palatal roots. Deep caries with no pulp exposure were observed in 30 % of the sample. Early bevelled apical root resorption was observed in two MB roots of the second molars, and three MB and two DB roots of the first molars. The apical resorption of the roots resulted in a thinner thickness of the dentine walls compared to the middle and cervical thirds and, in some cases, exposure of the root canal (Fig. 2d). Surface resorption at the internal aspect of the roots was observed in most of the specimens (n = 17).
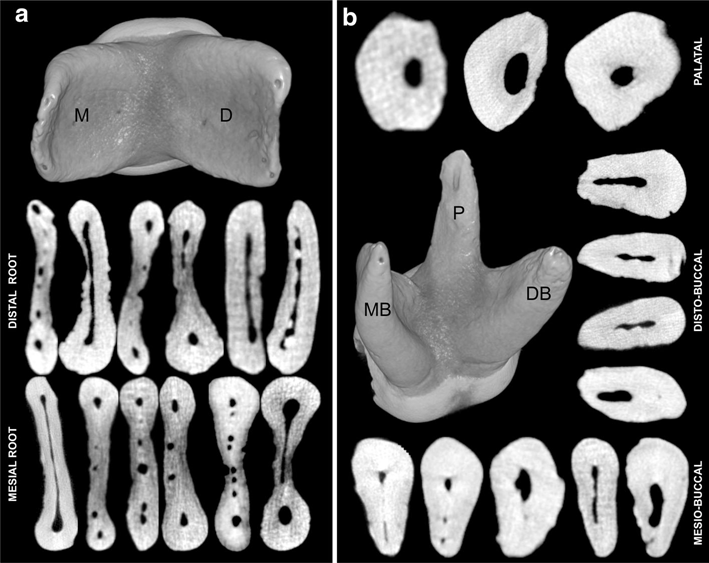
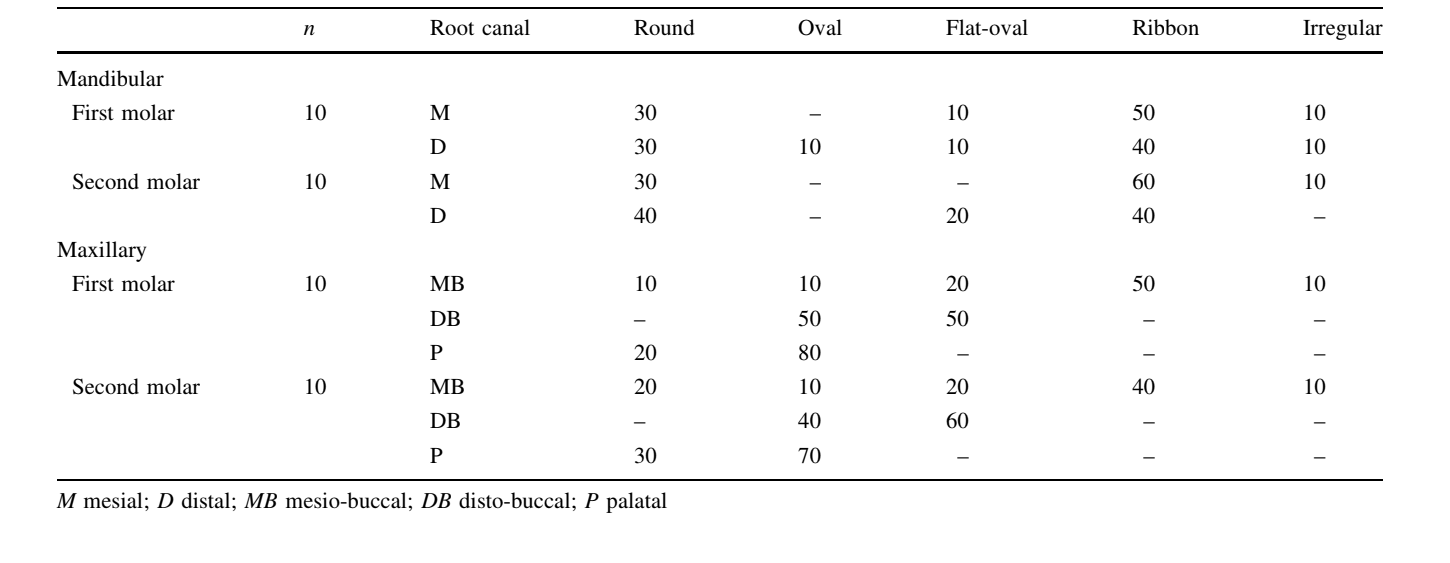
Exemplary cross sections of the roots of the mandibular and maxillary primary molars showed the complexity and the large dimensions of the root canal system in the apical third (Fig. 3). In the mandibular molars, mesial canal cross sections were significantly flatter and irregularly tapered in the mesio-distal plane. The presence of thin isthmuses, interconnecting branches, and multiples orifices were observed. Round-shaped canals were observed when the main canal split into multiple canals throughout the root, which occurred in 60 and 70 % of the first and second molars, respectively. In the maxillary molars, evaluation of the cross sections of the roots showed generally ribbon- or oval-shaped canals with large dimensions. However, in both mandibular and maxillary molars, the cross-sectional appearance of the canals varied in different levels of the root. Table 4 summarises the percentage frequency of root canal shape in each root of the primary maxillary and mandibular molars.
Discussion
Although detailed descriptions of the external and internal anatomical configuration of primary molars have been already reported using conventional methodologies (Hibbard and Ireland 1957; Simpson 1973; Badger 1982; Falk and Bowers 1983; Ringelstein and Seow 1989; Salama et al. 1992; Caceda et al. 1994; Winkler and Ahmad 1997; Wrbas et al. 1997; Kavanagh and O’Sullivan 1998; Fuks 2000; Eden et al. 2002; Goodacre 2003; Zoremchhingi et al. 2005; Aminabadi et al. 2008; Poornima and Subba Reddy 2008; Song et al. 2009; Bagherian et al. 2010; Liu et al. 2010; Cleghorn et al. 2012), no study has been undertaken to evaluate quantitatively their root canal system using high-resolution micro-computed tomography.
Primary mandibular molars have been usually described as having two grooved and divergent roots that flare to accommodate the developing permanent premolars (Hibbard and Ireland 1957; Zoremchhingi et al. 2005; Bagherian et al. 2010). In the literature, a considerable variation in number and shape of canal systems has been described in this group of teeth (Hibbard and Ireland 1957; Salama et al. 1992; Zoremchhingi et al. 2005; Aminabadi et al. 2008; Bagherian et al. 2010; Cleghorn et al. 2012). Anatomical anomalies, such as additional roots, dens invaginatus, and taurodontism, have also been reported, mostly in mandibular second molars (Badger 1982; Falk and Bowers 1983; Winkler and Ahmad 1997; Eden et al. 2002; Zoremchhingi et al. 2005; Johnston and Franklin 2006; Song et al. 2009; Bagherian et al. 2010; Liu et al. 2010). Overall, it may be inferred that the external and internal anatomy of the primary mandibular first molar closely resembles the primary mandibular second molar (Goodacre 2003; Cleghorn et al. 2012). Most studies have found either one or two canals in each of the mesial and distal roots (Hibbard and Ireland 1957; Zoremchhingi et al. 2005; Aminabadi et al. 2008; Bagherian et al. 2010). The incidence of double ribbon-shaped canal system has been reported to range from 24 to 100 % in the mesial root, and from 22.2 to 60 % in the distal root (Zoremchhingi et al. 2005; Aminabadi et al. 2008; Bagherian et al. 2010); however, two canals in the mesial root and one canal in the distal root comprised the most commonly reported anatomical configuration in primary mandibular molars (Cleghorn et al. 2012). In the present study, this configuration was observed in 50 and 40 % of the first and second mandibular molars, respectively. The lowest length of the distal roots was not reflected in the volume and surface area of the canal, which showed higher values than the mesial canal. An explanation can be found in the analysis of the 2D parameters, which showed the highest mean values of area, major and minor diameters in the distal canals of both molar types. Goodacre (2003) calculated the mean dimensions of primary teeth based on several studies and found that the mean lengths of the mesial and distal roots of the first and second molars were 10.5 and 8.9 mm, and 11.4 and 10.5 mm, which were higher than the present results. Primary maxillary molars have been described as having three divergent and separated roots that flare to accommodate the developing permanent premolars (Hibbard and Ireland 1957; Goodacre 2003; Zoremchhingi et al. 2005; Bagherian et al. 2010). Overall, it may be inferred that the external and internal anatomy of the primary maxillary first molar roots closely resembles the primary maxillary second molar roots (Hibbard and Ireland 1957; Goodacre 2003; Cleghorn et al. 2012). Despite the fact that anatomical anomalies have been also reported in this group of teeth, such as additional roots and taurodontism (Caceda et al. 1994; Kavanagh and O’Sullivan 1998; Johnston and Franklin 2006), they were not observed in this sample. The incidence of fusion between palatal and DB roots was observed in 40 % of the teeth, while in the literature it was reported as being 77.7 % (Bagherian et al. 2010), 53.5 % (Zoremchhingi et al. 2005), and 29 % (Hibbard and Ireland 1957) of the sample. Some variations in the number and shape of canal systems have also been described in the primary maxillary molars (Hibbard and Ireland 1957; Goodacre 2003; Zoremchhingi et al. 2005; Bagherian et al. 2010; Cleghorn et al. 2012). Most studies have found only one root canal in each root of both molar types (Hibbard and Ireland 1957; Zoremchhingi et al. 2005; Aminabadi et al. 2008; Bagherian et al. 2010). However, the incidence of a double canal system in the MB root was reported in 6.7 % (Zoremchhingi et al. 2005), 7.4 % (Bagherian et al. 2010), and 35 % (Hibbard and Ireland 1957) of the sample and, in the DB root, in 3.7 % of the specimens (Bagherian et al. 2010). In the present study, a double canal system was observed only in the MB root of two maxillary first molars. A previous study has found that the mean lengths of the MB, DB and palatal roots of the primary maxillary first molar were 8.8, 8.2 and 7.8 mm, respectively, and in the maxillary second molars 10.8, 9.7 and 10.8 mm, respectively (Goodacre 2003), which were higher than the present results. The lowest dimension of the palatal root in the maxillary first molar (5.96 mm) reflected the volume and surface area of the canal, which were significantly lower than the palatal canal of the second molar. The surface area of the DB canal in the second molar showed significantly higher values than in the first molar, despite the similar mean length between them. An explanation can be found in the analysis of the 2D parameters, which showed higher values of area, major and minor diameters in the DB canal of the second molar.
The SMI describes the plate- or cylinder-like geometry of an object. If a perfect plate is enlarged, the surface area does not change, yielding an SMI of zero. However, if a rod is expanded, the surface area increases with the volume and the SMI is normed, so that perfect rods are assigned an SMI score of 3 (Peters et al. 2000). In the mandibular molars, the mean SMI values varied from 1.69 to 2.06 indicating that the root canal system of the mesial and distal canals, in both molars, had flat cone-shaped geometry. In the maxillary molars, the mean SMI values of the canals in most of the specimens were higher than 2.08 indicating a conical shape geometry. The cross-sectional appearance of the root canal in the apical third was evaluated using the so-called morphometric parameter of roundness. In mandibular molars, mean roundness ranged from 0.31 to 0.49, which means that the root canal was more flat shaped. In the maxillary molars, the lowest range of values observed in the MB root of the second molar (0.26–0.33) indicated a ribbon-shaped canal and reflected its SMI data (1.81 ± 0.61). On the other hand, DB and P root canals, as well as MB canal of the first molar, were more oval shaped considering that the roundness ranged from 0.38 to 0.63.
The wide range of variations reported in the literature regarding the anatomy of the root canal system of primary molars, in comparison to the present results, has been mostly related to the diversity in sample origin, racial factors, the relatively small number of teeth in each group, the presence of initial apical root resorption in some specimens and, of course, to the methodological approach (Cleghorn et al. 2012). On the other hand, the micro-CT experimental model presented here overcomes several limitations displayed by the aforementioned conventional methods, as it provides useful 2D and 3D information related to the root canal space without changing the original sample. Unfortunately, these morphometric analyses cannot be compared to others because of the lack of similar reports in the literature to date.
Effective root canal debridement relies on accurate determination of the working length and adequate apical canal enlargement, which allow for better irrigation in the apical area, optimising root canal disinfection (Fornari et al. 2010). In the present study, major and minor diameters of the root canals in the apical third indicated that the debridement at this level could be improved with instruments up to an ISO size 100. However, considering the shape of the root canals, the reduced thickness of the dentine walls, and the difficulty in predicting the location of the canal terminus accurately in primary teeth (Beltrame et al. 2011), using instruments of this size would definitely lead to stripping or perforations of the roots. Clinically, 2D data results have definite implications for shaping and cleaning procedures, because only the minor diameter is evident on radiographs. Thus, clinicians must be aware of the anatomical configuration of the canals which, combined with the presence of thin isthmuses in the apical region, would compromise adequate cleaning and shaping, leaving untouched fins on the buccal and/or lingual aspects of the canal.
The introduction of nickel–titanium rotary file systems has resulted in a marked progress in the mechanical preparation of the root canal space (Hülsmann et al. 2005). However, shaping root canals with these systems has failed in debriding flat- and oval-shaped canals, leaving untouched fins or recesses on the buccal and/or lingual extensions (Versiani et al. 2011, 2013). Besides, large tapered rotary files should be avoided in primary mandibular molars considering their internal anatomical configuration. Recently, Self-Adjusting File (SAF; ReDent-Nova, Ra’anana, Israel) cleaning–shaping–irrigation system was introduced. This innovative instrument consists of a hollow and lightly abrasive nickel–titanium file composed of a metal lattice, which adapts itself to round, oval, or even long-oval cross sections of root canals. During its operation, which lasts 4 min, SAF removes dentine with a back- and-forth grinding motion by scrubbing the canal walls with a continuous irrigation provided by a peristaltic pump, i.e. it simultaneously performs the mechanical and chemical preparation of the root canal space (Metzger et al. 2010). Previous reports have shown that the SAF system was advantageous in promoting cleaning, shaping, and disinfection of oval-shaped canals in permanent teeth compared to rotary files (Siqueira et al. 2010; Versiani et al. 2011, 2013; Ribeiro et al. 2013), and may be an alternative for shaping procedures in primary molar teeth to be evaluated in further studies.
Conclusion
Under the limitations of this ex vivo study, it was possible to conclude that external and internal anatomy of the primary first molars closely resembles the primary second molars. Considering the morphology of the canals in the apical third, a careful selection of instruments including the use of additional disinfection supplements such as passive ultrasonic irrigation or negative apical pressure is advisable. The reported data may help clinicians to obtain a thorough understanding of the variations in root canal morphology of primary molars to overcome problems related to shaping and cleaning procedures.
Authors: A. C. Fumes, M. D. Sousa-Neto, G. B. Leoni, M. A. Versiani, L. A. B. da Silva, R. A. B. da Silva, A. Consolaro
References:
- Aminabadi NA, Farahani RM, Gajan EB. Study of root canal accessibility in human primary molars. J Oral Sci. 2008;50: 69–74.
- Badger GR. Three-rooted mandibular first primary molar. Oral Surg Oral Med Oral Pathol. 1982;53:547.
- Bagherian A, Kalhori KA, Sadeghi M, Mirhosseini F, Parisay I. An in vitro study of root and canal morphology of human deciduous molars in an Iranian population. J Oral Sci. 2010;52:397–403.
- Beltrame AP, Triches TC, Sartori N, Bolan M. Electronic determination of root canal working length in primary molar teeth: an in vivo and ex vivo study. Int Endod J. 2011;44:402–6.
- Caceda JH, Creath CJ, Thomas JP, Thornton JB. Unilateral fusion of primary molars with the presence of a succedaneous supernumerary tooth: case report. Pediatr Dent. 1994;16:53–5.
- Cleghorn BM, Boorberg NB, Christie WH. Primary human teeth and their root canal systems. Endod Topics. 2012;23:6–33.
- Eden EK, Koca H, Sen BH. Dens invaginatus in a primary molar: report of case. ASDC J Dent Child. 2002;69:49–53.
- Falk WV, Bowers DF. Bilateral three-rooted mandibular first primary molars: report of case. ASDC J Dent Child. 1983;50:136–7.
- Fornari VJ, Silva-Sousa YT, Vanni JR, et al. Histological evaluation of the effectiveness of increased apical enlargement for cleaning the apical third of curved canals. Int Endod J. 2010;43:988–94.
- Fuks AB. Pulp therapy for the primary and young permanent dentitions. Dent Clin N Am. 2000;44:571–96.
- Goodacre CJ. Atlas of the human dentition. 2nd ed. Loma Linda: Loma Linda School of Dentistry; 2003.
- Hibbard ED, Ireland RL. Morphology of the root canals of the primary molar teeth. J Dent Child. 1957;24:250–7.
- Hülsmann M, Peters OA, Dummer PMH. Mechanical preparation of root canals: shaping goals, techniques and means. Endod Topics. 2005;10:30–76.
- Johnston NJ, Franklin DL. Dental findings of a child with Wolf-Hirschhorn syndrome. Int J Paediatr Dent. 2006;16:139–42.
- Kavanagh C, O’Sullivan VR. A four-rooted primary upper second molar. Int J Paediatr Dent. 1998;8:279–82.
- Liu JF, Dai PW, Chen SY, et al. Prevalence of 3-rooted primary mandibular second molars among Chinese patients. Pediatr Dent. 2010;32:123–6.
- Metzger Z, Teperovich E, Zary R, Cohen R, Hof R. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy - a new concept of endodontic files and its implementation. J Endod. 2010;36:679–90.
- Peters OA, Laib A, Ruegsegger P, Barbakow F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res. 2000;79:1405–9.
- Poornima P. Subba Reddy VV. Comparison of digital radiography, decalcification, and histologic sectioning in the detection of accessory canals in furcation areas of human primary molars. J Indian Soc Pedod Prev Dent. 2008;26:49–52.
- Pratt WK. Digital image processing. 2nd ed. New York: Wiley; 1991. Ribeiro MVM, Silva-Sousa YT, Versiani MA, et al. Comparison of the cleaning efficacy of self-adjusting file and rotary systems in the apical third of oval-shaped canals. J Endod. 2013;39: 398–410.
- Ringelstein D, Seow WK. The prevalence of furcation foramina in primary molars. Pediatr Dent. 1989;11:198–202.
- Salama FS, Anderson RW, McKnight-Hanes C, Barenie JT, Myers DR. Anatomy of primary incisor and molar root canals. Pediatr Dent. 1992;14:117–8.
- Simpson WJ. An examination of root canal anatomy of primary teeth. J Can Dent Assoc. 1973;39:637–40.
- Siqueira JF Jr, Alves FR, Almeida BM, de Oliveira JC, Roças IN. Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. J Endod. 2010;36:1860–5.
- Song JS, Kim SO, Choi BJ, et al. Incidence and relationship of an additional root in the mandibular first permanent molar and primary molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;107:e56–60.
- Versiani MA, Pécora JD, Sousa-Neto MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod. 2011;37:1002–7.
- Versiani MA, Pécora JD, Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars: a micro-computed tomography study. J Endod. 2012;38:977–82.
- Versiani MA, Steier L, De-Deus G, et al. Micro-computed tomography study of oval-shaped canals prepared with the Self-adjusting File, Reciproc, WaveOne, and Protaper Universal systems. J Endod. 2013;39:1060–6.
- Winkler MP, Ahmad R. Multirooted anomalies in the primary dentition of Native Americans. J Am Dent Assoc. 1997;128: 1009–11.
- Wrbas KT, Kielbassa AM, Hellwig E. Microscopic studies of accessory canals in primary molar furcations. ASDC J Dent Child. 1997;64:118–22.
- Zoremchhingi, Joseph T, Varma B, Mungara J. A study of root canal morphology of human primary molars using computerized tomography: an in vitro study. J Indian Soc Pedod Prev Dent. 2005;23:7–12.