
Critical appraisal of some methodological aspects of using micro-CT technology in the study of dentinal microcracks in endodontics
We would like to take this opportunity to comment on the recently accepted paper entitled ‘Comparison of ProTaper, RaCe, and Safesider instruments in the induction of dentinal microcracks: A micro-CT study’ (Ceyhanhi et al. 2015). The authors evaluated the incidence of dentinal microcracks after root canal preparation with three instrumentation systems using micro-computed tomography (micro-CT). Firstly, it would be worth stressing the positive aspects of using this highly accurate contemporary non-destructive methodology to enhance the overall understanding of the relationship between intracanal procedures and the development of dentinal defects:
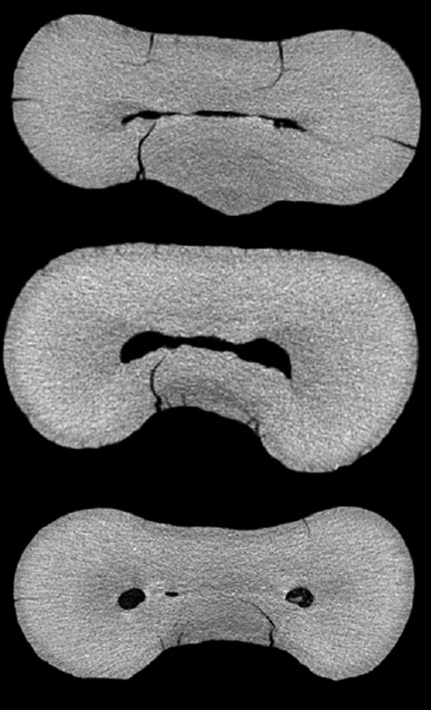
- It allows the assessment of the specimens before the experimental procedures; thus, pre-existing cracks can be detected (Fig. 1);
- Three-dimensional (3D) spatial location of dentinal cracks is possible with or without the use of contrast agents;
- The same specimen can be evaluated at different stages of the root canal treatment and serve as its own control;
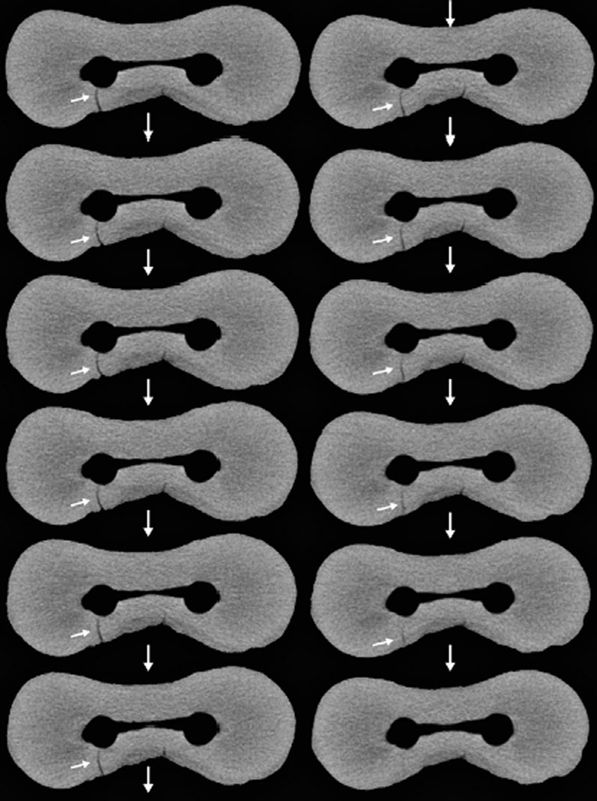
- The presence of dentinal defects can be correlated with other outcomes of mechanical instrumentation (Fig. 2) (De-Deus et al. 2014, 2015).
Nevertheless, as with any other methodological approach, micro-CT technology has also limitations:
- Scanning and reconstruction procedures take a considerable time;
- The technique is not suitable for clinical use;
- The equipment is expensive and;
- The complexity of the technical procedures requires a steep learning curve and an in-depth knowledge of dedicated software.
Recently, several authors have raised important concerns regarding the development of dentinal defects due to motor-driven rotary nickel-titanium instrumentation; however, the literature reveals that there is a lack of consensus on microcrack formation after canal preparation with rotary or reciprocating instruments, with the reported incidence of cracks varying from 0% to 80%. This wide range variation may be explained by differences in the methodological procedures, the experience of the operator, and the output quality of the observational tool. The latter is of critical relevance as it must allow reliable visualization of the dentinal defects and, consequently, it has a major impact on the accuracy of the results. When using micro-CT technology, the output quality of the acquired images is directly related to the high spatial and temporal resolution of the micro-CT scanner, as well as, the adoption of adequate input parameters for the scanning and reconstruction procedures. These factors make reliable dentinal surface examination challenging but, in the end, they lead to the expected and required overall trustworthiness of the study.
Based on the aforementioned considerations, we would like to point out some aspects of the above-mentioned study that might impact on its conclusions:
- According to the authors, the root canals ‘were instrumented up to size 30 for all systems’; however, in the Safesider group, previous preparation of the root canal was performed to the working length with manual files from size 08 to 35;
- Despite the use of a 3D technology, the methodology surprisingly followed the conventional sectioning approach. For instance, 700–900 CT slices [.. .] were obtained per root”, but only 10 sections were evaluated in each specimen, which represent <1.5% of the total acquired images. One of the advantages of micro-CT imaging over root sectioning and microscopy observation is that hundreds of slices can be analyzed per tooth. Therefore, there is no rationale to justify evaluating only a few slices per specimen when the entire root was screened;
- The authors’ approach also does not allow the differentiation between genuine dentinal defects from artefact or noise (false-positive output) created in a single slice during image acquisition or reconstruction, which can only be achieved by performing sequential analysis of the cross-section slices throughout the longitudinal axis of the root (Fig. 2);
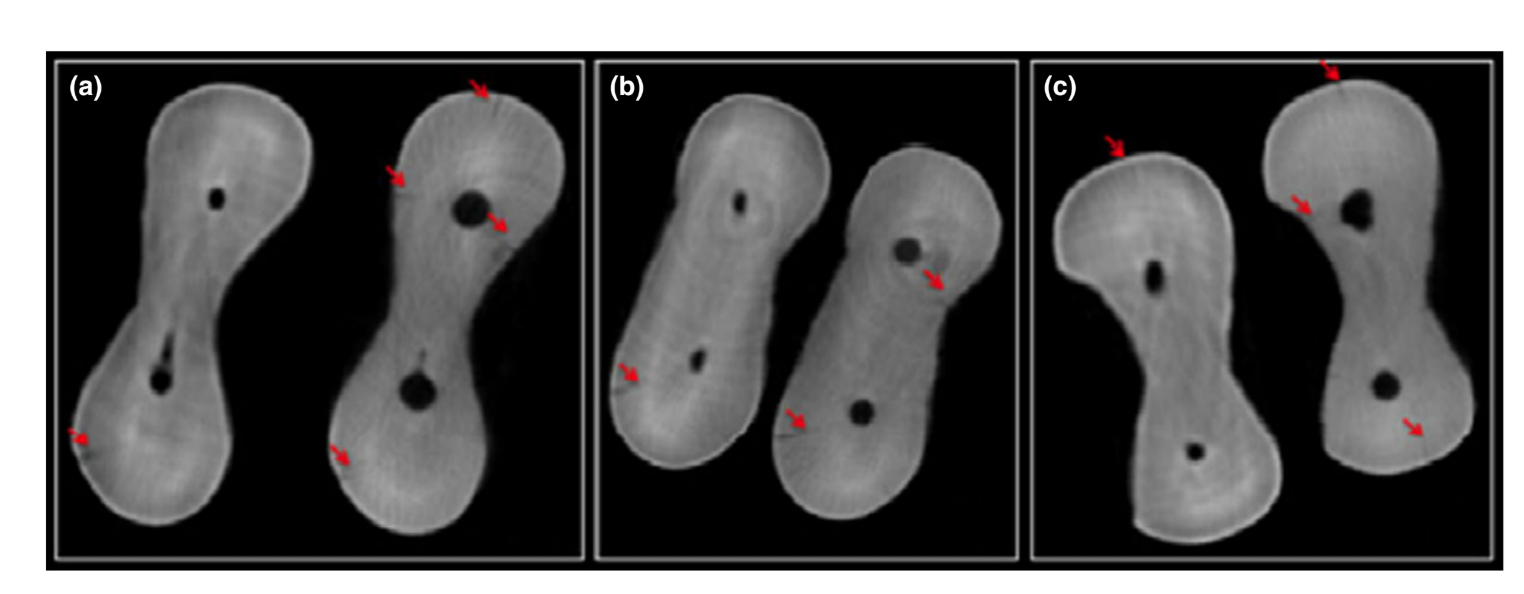
- In the study, the ‘long axes of the roots were adjusted to be perpendicular to the beam to provide scans in the same sagittal positions’; unfortunately, this procedural step does not warrant the sample to be placed exactly at the same position before and after the experimental setup. This is clearly depicted at Fig. 3 (Figure 1 in the study), in which images acquired before and after preparation are dissimilar in all groups. Actually, the use of dedicated software to co-register the image stacks with an average error less than a voxel is a crucial analytical step to allow a precise analysis of the same image at the same point of the root before and after intracanal procedures. This step was not followed in this study, which increases the possibility that different cross-sections were compared, leading to erroneous interpretation;
- The exceedingly noisy images showed in Fig. 3 (Figure 1 in the study) can interfere with the evaluation process, hindering a trustworthy interpretation of the occurrence and propagation of dentinal damage, resulting in an underestimation of the problem, or the detection of false positive cracks, which may lead to overestimation of the problem. For example, despite the fact that the roots were previously ‘inspected under a stereomicroscope [...] with 109 magnification to exclude external defects or cracks’; all representative cross-sections in Fig. 1 had ‘cracks’ on the root surface before canal preparation;
- Based on the limitations of the X-ray penetration depth (maximum output of 50 kV) and the detector resolution (1.3 Mp CCD) of the micro-CT scanner used in the study, as well as, the smooth dentinal surface aspect (Fig. 3), it may be inferred that different filters were used during the reconstruction process, which may lead to the distortion of the image at some level. Taking into account that the scanning and reconstruction parameters used in the study were not reported, the reliability of the results and the reproducibility of the method, the main principles of the scientific method, cannot be tested by other research groups.
Considering that most readers of the International Endodontic Journal may not be able to critically appraise these detailed methodological factors behind this new technological resource used for the evaluation of dentinal defects related to endodontic procedures, it would be advisable to consider the abovementioned issues and concerns regarding this paper.
Authors: G. De-Deus, F. G. Belladonna, E. J. N. L. Silva, E. M. Souza, M. A. Versiani
References:
- Ceyhanhi KT, Erdilek N, Tatar I, Celik D (2015) Comparison of ProTaper, RaCe, and Safesider instruments in the induction of dentinal microcracks: a micro-CT study. International Endodontic Journal Doi: 10.111 1/iej.12497. [Epub ahead of print].
- De-Deus G, Silva EJ, Marins J et al. (2014) Lack of causal relationship between dentinal microcracks and root canal preparation with reciprocation systems. Journal of Endodontics 40, 1447–50.
- De-Deus G, Belladonna FG, Souza EM et al. (2015) Micro- computed tomographic assessment on the effect of ProTaper Next and Twisted File Adaptive systems on dentinal cracks. Journal of Endodontics 41, 1116–9.