
Accumulated Hard Tissue Debris Produced during Reciprocating and Rotary Nickel-Titanium Canal Preparation
Abstract
Introduction: This study compared the amount of hard tissue debris produced after different apical enlargement with single-file reciprocating systems (WaveOne [Dentsply Maillefer, Baillaigues, Switzerland] and Reciproc [VDW, Munich, Germany]) and a conventional multifile rotary system (BioRaCe [FKG Dentaire, La Chaux-de-Fonds, Switzerland]) using micro–computed tomographic imaging.
Methods: Thirty moderately curved mesial roots of mandibular molars presenting 2 independent root canals were selected and scanned at an isotropic resolution of 14.16 mm. The sample was assigned to 3 groups (n = 10) with respect to the root length and degree of curvature of the mesial root according to the system used for the root canal preparation: Reciproc, WaveOne, and BioRaCe. Second and third scans were taken after the root canals were prepared up to ISO sizes 25 and 40, respectively. The matched images of the mesial canals, before and after preparation, were examined from the furcation level to the apex to evaluate the amount of hard tissue debris (%). Data were statistically compared using a general linear model for repeated-measures with a significance level set at 5%.
Results: Instrumentation systems per se did not influence the amount of hard tissue accumulation (P > .05), whereas a significant reduction in the percentage of hard tissue debris was observed after sequential enlargement in all groups (P < .05).
Conclusions: None of the systems yielded root canals completely free from packed hard tissue debris. The increased final apical size resulted in significantly less debris accumulation for both reciprocating and rotary systems.
In 2011, Paque et al reopened the discussion about the substantial amount of debris packed in the fins, isthmuses, irregularities, and ramifications of the root canal system after preparation using an innovative approach based on micro–computed tomographic (micro-CT) imaging. Micro-CT imaging allows monitoring the accumulation and removal of radiopaque structures in the main space of the root canal and its recesses and isthmuses during and after instrumentation while preserving the sample integrity
Hard tissue debris accumulation has been considered an undesirable side effect of the shaping procedures and may be considered more clinically relevant than the smear layer per se because it could easily harbor bacterial contents away from the disinfection procedures. It has been shown that the currently used irrigation systems and solutions are unable to render root canals completely free from packed hard tissue debris, which raises the need for preparation protocols that reduce debris buildup.
The introduction of new preparation systems based on the use of only 1 instrument through a reciprocating motion has raised new perspectives for the mechanical preparation of the root canal space. The reciprocating working motion consists on a forward counterclockwise rotation to cut dentin and a shorter clockwise rotation to relieve the instrument. Overall, research findings on reciprocating systems report a decrease in preparation time, increased cyclic fatigue life, and similar shaping ability compared with multiple-file systems. In the literature, it remains controversial whether the use of reciprocating movement per se is able to influence the final amount of packed hard tissues debris in the root canal. Likewise, the impact of further apical enlargement on the accumulation of hard tissue debris is still unknown.
Within this background, the current study was designed to compare the volume of hard tissue debris accumulated in mesial root canals of mandibular molars prepared by single-file reciprocating systems (WaveOne [Dentsply Maillefer, Baillaigues, Switzerland] and Reciproc [VDW, Munich, Germany]) and a conventional multifile rotary system (BioRaCe [FKG Dentaire, La-Chaux-de- Fonds, Switzerland]) at 2 different apical sizes using micro-CT technology. The following hypotheses were tested:
- Single-file reciprocating systems produce less hard tissue debris accumulation than a conventional multifile system.
- Single-file reciprocating systems produce similar hard tissue accumulation.
- Larger apical preparation is an effective antidebris strategy.
Materials and Methods
Sample Size Estimation
A repeated measures analysis of variance, within-between interaction was selected from the F tests family in G*Power 3.1.7 software for Windows (Heinrich Heine, Universität Düsseldorf). Because of the lack of previous studies evaluating hard tissue debris accumulation after canal preparation with reciprocating instruments at different apical enlargements, the effect size for this study was established from the medium convention (0.2526, derived from n2 = 0.06). An alpha-type error of 0.05, power beta of 0.95, correlation among repeated measures of 0.7, nonsphericity correction of 1, number of groups (within subjects) of 2, and number of measurements (between subjects) of 3 were also specified. Twenty-six teeth were indicated as the total sample size required to observe significant differences.
Specimen Selection
From a pool of 300 mandibular first molar teeth, moderately curved mesial roots (10◦–20◦) were selected applying Schneider’s method in digitized buccolingual radiographs using AxioVision 4.5 software (Carl Zeiss Vision GmbH, Hallbergmoos, Germany). In addition, the inclusion criteria comprised only mandibular molars presenting 2 independent root canals in the mesial root (Vertucci type II configuration system) in which the final apical gauging allowed for an ISO size 10 hand K-file (Dentsply Maillefer) to be placed to the working length (WL). Based on these criteria, 44 mesial molar roots were selected. After resection of the distal root at the furcation level, 14 teeth were discarded, and 30 mesial roots were disinfected in 0.5% chloramine T, stored in distilled water at 4◦C, and used within 6 months after extraction.
The specimens were randomly assigned (http://www.random.org) into 3 experimental groups (n = 10) according to the system used for the chemomechanical preparation: Reciproc, WaveOne, and BioRaCe. After checking for normality assumption (P > .05, Shapiro-Wilk test), the degree of homogeneity of the groups, with respect to the root length and degree of curvature of the mesial root, was statistically confirmed (P > .05, 2-way analysis of variance). For the experimental procedures, the apex of the mesial roots was sealed with hot glue, and the roots were embedded into a thin film of polyvinyl siloxane.
Root Canal Preparation
Root canals were accessed and patency confirmed by inserting a size 10 hand K-file through the apical foramen before and after completion of root canal preparation. For all groups, a glide path was created by scouting a stainless steel size 15 K-file (Dentsply Maillefer) up to the WL, which was established by deducting 1 mm from the canal length. In each group, instruments were driven with the VDW Silver motor (VDW GmbH) according to each manufacturer’s instructions, and a single experienced operator performed all preparations.
Group 1: Reciproc System
Reciproc R25 (25/0.08) (VDW GmbH) was introduced into the canal until resistance was felt and then activated in reciprocating motion. The instrument was moved in an apical direction using an in- and-out pecking motion of about 3 mm in amplitude with a light apical pressure. After 3 pecking motions, the instrument was removed from the canal, and its flutes were cleaned off. This procedure was performed until the instrument reached the WL. Afterward, the Reciproc R40 instrument (40/0.06) (VDW GmbH) was used with the same protocol.
Group 2: WaveOne System
WaveOne Primary (25/0.08) and Large (40/0.08) instruments (Dentsply Maillefer) were used to the WL following the same protocol described for group 1.
Group 3: BioRaCe System
BioRaCe instruments (FKG Dentaire) were used in a crown-down manner according to the manufacturer’s instructions using the following sequence: BR0 (25/0.08), BR1 (15/0.05), BR2 (25/0.04), BR3 (25/0.06), BR4 (35/0.04), and BR5 (40/0.04) instruments. The motor was adjusted to 500–600 rpm and 1 N/cm2. After 4 gentle in- and-out motion strokes, the instrument was removed from the canal and cleaned until the WL was reached.
After the glide path and each nickel-titanium file, root canals were irrigated with 2 mL 5.25% NaOCl for 1 minute delivered by a VATEA peristaltic pump (ReDent-Nova, Ra’anana, Israel) at a 2-mL/min rate connected to a 30-G Endo-Eze Tip (Ultradent Products Inc, South Jordan, UT) inserted up to 2 mm from the apical foramen. Aspiration was performed with a SurgiTip (Ultradent Products Inc) attached to a high-speed suction pump. After canal preparation to size 40, an additional rinse with either 18 mL/9 min (for the rotary group) or 24 mL/ 12 min (for the reciprocating groups) NaOCl was performed to equalize the amount and time of irrigant used within the groups. A final rinse with 5 mL 17% EDTA (pH = 7.7) delivered at a 1-mL/min rate for 5 minutes followed by a 5-minute 5-mL rinse with bidistilled water was performed for both groups. Hence, a total volume of 40 mL irrigant was used per canal in a total time of 25 minutes. Then, canals were dried with absorbent paper points (Dentsply Maillefer).
Micro-CT Scanning
Three high-resolution scans were accomplished per tooth:
- Before treatment
- After root canal preparation up to ISO size 25
- After root canal preparation up to ISO size 40
Teeth were placed inside a custom-made epoxy resin holder (Ø = 18 mm) and adapted into a sample holder of a micro-CT device (Sky- Scan 1173; Bruker-microCT, Kontich, Belgium). Scanning procedures were performed at an isotropic resolution of 14.16 mm, 70 kV, 114 mA, 360◦ rotation around the vertical axis, rotation step of 0.5◦, and camera exposure time of 250 milliseconds. Acquired projection images were reconstructed into cross-sectional slices (NRecon v.1.6.9; Bruker-microCT) using standardized parameters for beam hardening (40%) and ring artifact correction of 10 as well as similar contrast limits. The volume of interest was selected extending from the furcation level to the apex of the root, resulting in the acquisition of 700 to 900 transverse cross sections per tooth.
Quantitative Tridimensional Image Analysis
Evaluation procedures have been described elsewhere in details. Image stacks, before and after canal preparation, were registered using an automatic superimposition, and volumes of matched root canals before and after preparation were calculated. Material with density similar to dentin in instrumented canal regions, which were previously occupied by air, was considered to be debris. Accumulated hard tissue debris was calculated as the percentage volume of the original canal anatomy after intersecting the stacks of original and instrumented root canal space. All image analysis operations were undertaken using the ImageJ software v.1.49n implementation (Fiji, Madison, WI) interface . Subsequently, the images obtained after debris quantification were 3-dimensionally rendered using the plugin 3D Viewer (Internationale Medieninformatik, HTW Berlin, Berlin, Germany) and qualitatively evaluated with CTVol v.2.2.1 software (Bruker-microCT).
Statistical Analysis
Raw data normal distribution was confirmed using the Shapiro-Wilk test (P > .05). Because of the dependent nature of the study design, a general linear model for repeated measures (SPSS for Windows v17.0; SPSS Inc, Chicago, IL) was selected for analysis. File sizes were tested as the within-subject effects, whereas instrumentation systems were set as between-subject effects. Significance was established at a = 5%.
Results
Figure 1 displays the overall percentage volume of hard tissue debris. The mean percentage volume of hard tissue debris after preparation to instrument ISO size #25 ranged from 0.116–0.227 mm3, whereas after additional enlargement with instrument ISO size #40 it varied from 0.022–0.079 mm3. The mean and standard deviation percentage volume of hard tissue debris for size 25 files (Reciproc = 19.01 [ 15.39], BioRaCe = 28.74 [ 23.60], and WaveOne = 18.84.
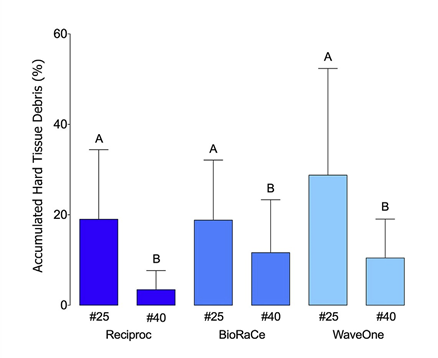
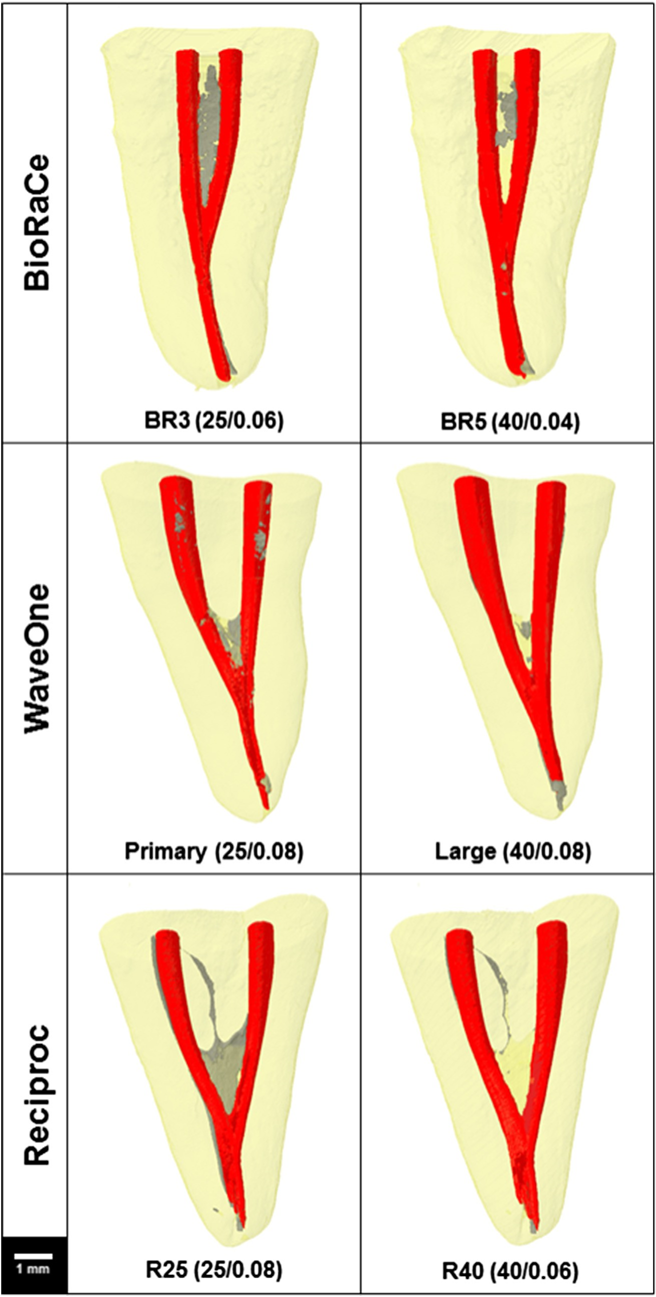
[ 13.26]) and size 40 files (Reciproc = 3.46 [ 4.21], BioRaCe = 10.46 [ 8.60], and WaveOne = 11.63 [ 11.71]) are provided in Figure 1. Instrumentation systems did not influence the amount of hard tissue debris accumulation (P [systems] = .236), whereas a highly significant reduction in the percentage of accumulated hard tissue debris was observed after apical enlargement (P [file] = .000), which is valid for all file systems (P [file * systems] = .388). Sphericity was met at Mauchly’s W = 1.0. Three-dimensional representative reconstructions of the mesial root canals of mandibular molars before and after preparation with different systems visually agreed with the quantitative results (Fig. 2).
Discussion
The present study was unable to detect significant differences in the amount of hard tissue debris in the mesial root canals of mandibular molars prepared by the 2 single-file reciprocating systems (Reciproc and WaveOne) and a standard multifile rotary system (BioRaCe). Thus, the first hypothesis was rejected. Despite differences in the cross-sectional designs, tapers, and dynamics of movement of the tested instruments, the similarity of the results observed herein might be regarded as a consequence of the use of the BioRaCe system as the reference rotary nickel-titanium technique because this system comprises instruments with more positive cutting edges; therefore, this aggressive angle may produce a larger amount of debris. However, these results are not in accordance with Robinson et al, who reported that a rotary system yielded cleaner canals with significantly less debris accumulation (~10%) than a reciprocating system. Similar to the present study, Robinson et al used mesial canals of mandibular molars and found ~19% of hard tissue debris accumulation with the WaveOne Primary. However, by using the ProTaper Universal system as a standard for comparison in which the instruments present cutting edges of negative angles, a much lower amount of debris compared with the BioRaCe system can be speculated to understand the difference between the 2 studies. Also, Paqu´e et al found ~10% of accumulated hard tissue debris in mesial canals of mandibular molars after the use of the ProTaper system, which may help in confirming the reproducibility and reliability of the current micro-CT technology. It is also worth noting that, even though we have used 8 times more volume of irrigant than Robinson et al, it seems that the hard debris packed into fins and isthmuses remained largely unaffected, probably because of their dense packing by the instruments. This underscores the need for irrigation systems that enhance the energy of the solutions inside the canal in order to improve the dislocation force over packed debris.
Interestingly, the second hypothesis was accepted because no statistical difference in the mean percentage volume of debris was observed between Reciproc and WaveOne systems. It would be expected that the marked differences between them related to the cross-sectional design, core size, and taper would have resulted in different hard tissue debris accumulation patterns. However, it seems that the similarities between these systems such as the reciprocation movement, M-wire alloy, and tip size have prevailed in generating the consonant results observed herein.
Undoubtedly, hard tissue debris accumulation is an undesired side effect of the currently available shaping technology because they can potentially harbor bacteria within the root canal system and also negatively interfere with the adhesion and sealability of the root canal filling materials. Several antidebris strategies have been proposed to improve the final cleansing of the root canal space, some of them related to the use of chelating agents or irrigating protocols and others to the mechanical shaping of the root canal itself. Regarding the latter, apical enlargement and increased canal taper have been recommended because these approaches are expected to both optimize the removal of infected dentin and improve the irrigation efficiency. Consequently, the third hypothesis of this study was sustained because root canal enlargement significantly reduced the overall amount of packed hard tissue debris for the tested systems by 34%. Logical reasoning dictates that the higher the number of instruments used for canal preparation, the greater the amount of debris produced and packed within the canal space. However, this rationale was not confirmed in this study and might be explained by the interplay between the enlargement itself, which aided in reducing the amount of packed debris, and the improved ability to remove debris using a conventional irrigation protocol in larger apical preparations because of better apical flush of the irrigant.
According to the manufacturers of the reciprocation systems, if the root canal is considered narrow, as mesial canals of mandibular molars, the instrument of choice is R25 for Reciproc and the Primary for WaveOne. The first step of root canal preparation was performed herein accordingly in both experimental groups. However, clinically speaking, it is of note that there are no scientifically established guidelines to set the optimal final size canal preparation. Therefore, different philosophies regarding the optimal canal preparation size and shape were proposed, resulting in some controversy as to whether apical enlargement is indeed necessary. For example, the Scandinavian approach always recommends larger apical preparations, whereas Herbert Schilder–based thinking recommends more conservative apical enlargement
Consequently, the present study was designed considering that both systems have larger instruments that could be used as a sequence of an initial and smaller instrument in order to increase the enlargement of the root canal space.
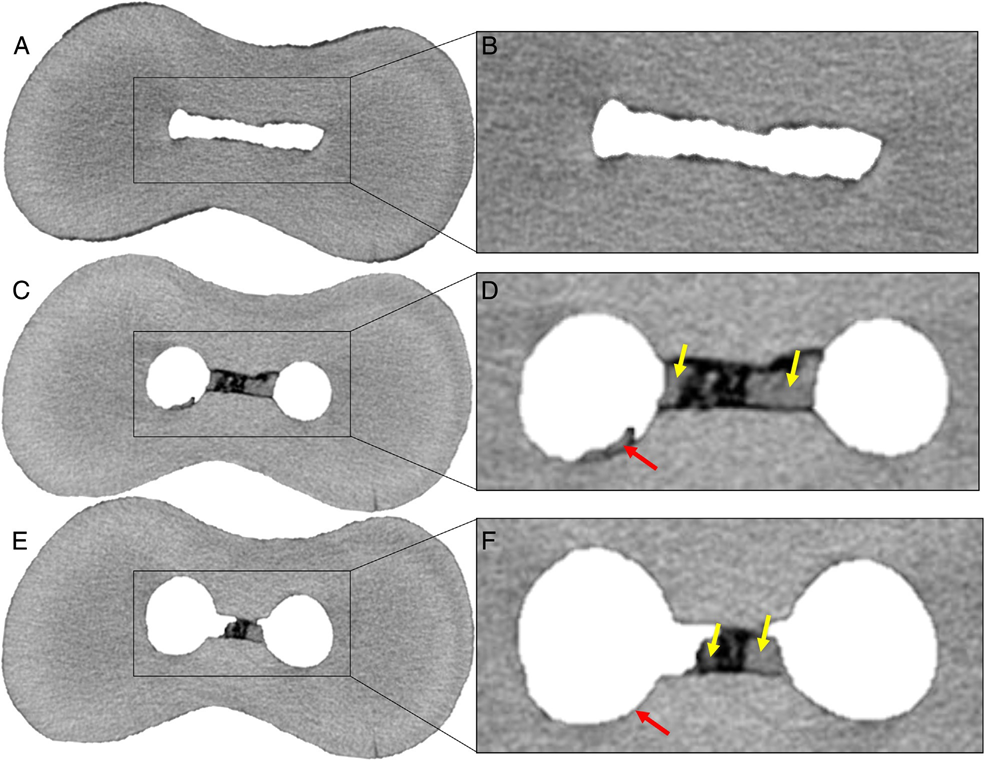
The significant reduction in the percentage volume of accumulated hard tissue debris after apical enlargement is the most important outcome of the present study, as seen in Figure 3. However, even after apical enlargement, none of the tested systems yielded root canals completely free from packed hard tissue debris. Thus, before proposing apical enlargement as an additional antidebris strategy, the possibility of root weakening, strip perforation, and an increase in instrument fracture risk, especially in severely curved canals using an enlargement approach, should be evaluated further. In fact, this output, taken together with other studies using the nondestructive and reliable micro-CT approach, underlines the less than ideal ability of the current available devices and solutions to completely clean the root canal space. This clearly indicates the need for the development of new protocols and instruments able to optimize the root canal space cleaning.
Authors: Gustavo De-Deus, Juliana Marins, Emmanuel Joao Nogueira Leal Silva, Erick Souza, Felipe Gon¸calves Belladonna, Claudia Reis, Alessandra Silveira Machado, Ricardo Tadeu Lopes, Marco Aurelio Versiani, Sidnei Paciornik and Aline Almeida Neves
References
- Paqu´e F, Laib A, Gautschi H, Zehnder M. Hard-tissue debris accumulation analysis by high-resolution computed tomography scans. J Endod 2009;35:1044–7.
- Robinson JP, Lumley PJ, Claridge E, et al. An analytical Micro CT methodology for quantifying inorganic dentine debris following internal tooth preparation. J Dent 2012;40:999–1005.
- Robinson JP, Lumley PJ, Cooper PR, et al. Reciprocating root canal technique induces greater debris accumulation than a continuous rotary technique as assessed by 3-dimensional micro-computed tomography. J Endod 2013;39: 1067–70.
- De-Deus G, Marins J, Neves AA, et al. Assessing accumulated hard-tissue debris using micro-computed tomography and free software for image processing and analysis. J Endod 2014;40:271–6.
- Versiani MA, Steier L, De-Deus G, et al. Micro–computed tomography study of oval- shaped canals prepared with the Self-adjusting File, Reciproc, WaveOne, and Pro- Taper Universal systems. J Endod 2013;39:1060–6.
- Endal U, Shen Y, Knut A, et al. A high-resolution computed tomographic study of changes in root canal isthmus area by instrumentation and root filling. J Endod 2011;37:223–7.
- Paqu´e F, Boessler C, Zehnder M. Accumulated hard tissue debris levels in mesial roots of mandibular molars after sequential irrigation steps. Int Endod J 2011; 44:148–53.
- Paqu´e F, Al-Jadaa A, Kfir A. Hard-tissue debris accumulation created by conventional rotary versus self-adjusting file instrumentation in mesial root canal systems of mandibular molars. Int Endod J 2012;45:413–8.
- Burklein S, Hinschitza K, Dammaschke T, et al. Shaping ability and cleaning effectiveness of two single-file systems in severely curved root canals of extracted teeth: Reciproc and WaveOne versus Mtwo and ProTaper. Int Endod J 2012;45:449–61.
- Kiefner P, Ban M, De-Deus G. Is the reciprocating movement per se able to improve the cyclic fatigue resistance of instruments? Int Endod J 2014;47:430–6.
- Stern S, Patel S, Foschi F, et al. Changes in centring and shaping ability using three nickel-titanium instrumentation techniques analysed by micro-computed tomography (mCT). Int Endod J 2012;45:514–23.
- Gergi R, Osta N, Bourbouze G, et al. Effects of three nickel titanium instrument systems on root canal geometry assessed by micro-computed tomography. Int Endod J 2015;48:162–70.
- Schneider SW. A comparison of canal preparations in straight and curved root canals. Oral Surg Oral Med Oral Pathol 1971;32:271–5.
- Schneider CA, Rasband WS, Eliceiri KW. NIH Image to ImageJ: 25 years of image analysis. Nat Methods 2012;9:671–5.
- Junior EC, da Fonseca TS, da Frota MF, et al. Cleaning capacity of hybrid instrumentation technique using reamer with alternating cutting edges system files: histological analysis. Contemp Clin Dent 2014;5:203–8.
- You SY, Kim HC, Bae KS, et al. Shaping ability of reciprocating motion in curved root canals: a comparative study with micro-computed tomography. J Endod 2011;37: 1296–300.
- Nair PN, Henry S, Cano V, et al. Microbial status of apical root canal system of human mandibular first molars with primary apical periodontitis after ‘‘one-visit’’ endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2005;99:231–52.
- Hu X, Ling J, Gao Y. Effects of irrigation solutions on dentin wettability and roughness. J Endod 2010;36:1064–7.
- Fornari VJ, Silva-Sousa YT, Vanni JR, et al. Histological evaluation of the effectiveness of increased apical enlargement for cleaning the apical third of curved canals. Int Endod J 2010;43:988–94.
- de Melo Ribeiro MV, Silva-Sousa YT, Versiani MA, et al. Comparison of the cleaning efficacy of Self-adjusting File and rotary systems in the apical third of oval-shaped canals. J Endod 2013;39:398–401.
- Boutsioukis C, Gogos C, Verhaagen B, et al. The effect of apical preparation size on irrigant flow in root canals evaluated using an unsteady Computational Fluid Dynamics model. Int Endod J 2010;43:874–81.
- Boutsioukis C, Gogos C, Verhaagen B, et al. The effect of root canal taper on the irrigant flow: evaluation using an unsteady Computational Fluid Dynamics model. Int Endod J 2010;43:909–16.
- Lumley PJ. Cleaning efficacy of two apical preparation regimens following shaping with hand files of greater taper. Int Endod J 2000;33:262–5.
- Albrecht LJ, Baumgartner JC, Marshall JG. Evaluation of apical debris removal using various sizes and tapers of ProFile GT files. J Endod 2004;30:425–8.
- Falk KW, Sedgley CM. The influence of preparation size on the mechanical efficacy of root canal irrigation in vitro. J Endod 2005;31:742–5.
- Usman N, Baumgartner JC, Marshall JG. Influence of instrument size on root canal debridement. J Endod 2004;30:110–2.
- Peters O. Current challenges and concepts in the preparation of root canal systems: a review. J Endod 2004;30:559–67.