The Influence of a New Clinical Motion for Endodontic Instruments on the Incidence of Postoperative Pain
Abstract
Objectives. Previous studies showed that motor motions play an important role in determining apical extrusion of debris. Therefore a new clinical motion (MIMERACI) has been proposed. The basic idea is to progress slowly (1mm advancement), and after each 1mm, to remove the instrument from the canal, clean flutes and irrigate. The aim of the study was to prove whether the clinical use of MIMERACI technique would influence or not postoperative pain.
Materials and methods. 100 teeth requesting endodontic treatment were selected for the study and divided into two similar groups based on anatomy, pre-operative symptoms and vitality, presence or absence of periapical lesion. All teeth were shaped, cleaned and obturated by the same operator, using the same NiTi instruments. The only difference between the two groups was the instrumentation technique: tradional (group A) vs MIMERACI (group B). Assessment of postoperative pain was performed 3 days after treatment. Presence, absence and degree of pain were recorded with a visual analogue scale (VAS), validated in previous studies. Collected data statistically analyzed using one-way ANOVA post hoc Tukey test.
Results. For VAS pain scores MIMERACI technique showed signi- ficantly better results than group A (p=0,031). Overall, both incidence and intensity of symptoms were significantly lower. Flare ups occurred in 3 patients, but none treated with the MIMERACI Technique.
Conclusions. Since extruded debris can elicit more postoperative pain, results obtained by using MIMERACI technique are probably due to many factors: better mechanical removal and less production of debris and more efficient irrigation during instrumentation.
Introduction
Dentists are aware that root canal preparation procedures are not easy to perform, due to anatomical complexities and limitations of the endodontic instruments, which often result in a high risk of iatrogenic errors. Some iatrogenic errors, like instruments’ breakage, canal blockage or transportation, can dramatically affect the outcome of the treatment by impeding a valid debridement and disinfection of the root canal systems. Other errors, like apical extrusion of debris, may not have such a high impact on the outcome of the treatment, but can significantly affect patients’ postoperative discomfort. Moreover, even if less dramatic, such iatrogenic errors are very frequent. It has been shown that in the great majority of clinical cases dentine chips, pulp tissue fragments, necrotic tissue, microorganisms and intracanal irrigants may be extruded from the apical foramen during the canal instrumentation, and elicit postoperative inflamation of periapical tissue, with increased pain and or flare-ups. The incidence and relevance of these symptoms depend mainly on the quantity of extruded debris, the amount and type of bacteria inside them, the initial pathology and the host response.
While there are statistical predictors of postoperative pain (nonvital teeth, patients already in pain, asymptomatic teeth with lesions, etc.), its occurrence may not be inevitable, but to a large extent can be minimized by using proper instrumentation and irrigation techniques. Therefore, prevention is a mainly function of providing excellent treatment, more precisely by creating a well cleaned and disinfected canal, by removing the majority of inorganic and organic debris from the canal space and by using instrumentation techniques that reduce the risk of extrusion of canal contents during the process.
Pain remains one of the most significant challenges in endodontic treatment, and while some innovations show promise, effective pain management in endodontics goes far beyond technique alone. If you’re committed to delivering pain-free endodontic treatment and deepening your expertise in pain diagnosis, management and prevention, join the course "Everything about pain in endodontics. Online course from Michael Solomonov". Gain the tools and confidence to manage even the most complex pain cases!
In the last decades there has been a significant improvement in the root canal instruments with the introduction of the nickel-titatium (NiTi) alloy. Innovative designs and manufacturing processes have been proposed to produce safer and more efficient instruments, and to simplify procedures by reducing the number of nickel titanium instruments and consequently instrumentation time. More recently, new motors using reciprocation instead of continuous rotation have been commercialized, to increase resistance to brakage, but these new instruments and motions were found to have a tendency to extrude more debris and/or decrease quality of clinical debridement.
Since motor motion plays such an important role in determining apical extrusion of debris, also clinical motion (which is the way clinicians use an instrument inside the canal) may have such a role. Therefore, a new clinical motion, which is designed to improve safety and efficiency of NiTi instrumentation has been proposed: the “MIMERACI” technique (Fig. 1). The motion works for both continuous rotation and reciprocation, because the resulting motion of any NiTi reciprocating is a non continuous rotatation.
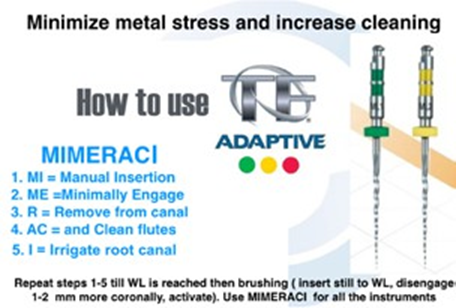
MIMERACI is acronym which stands for: MI = Manual insertion, ME = Minimal Engagement, R = Remove (instrument from canal) AC = And Clean flutes I = Irrigate.
The basic idea is to progress slowly (maximum 1 mm advancement) inside the canal, and after each 1 mm progression to remove the instrument from the canal, clean flutes and irrigate. In such a way the instrument has a minimal engagement, produces less debris, and most of the produced debris, which are entrapped within flutes, are predictably removed “outside“ the canal by cleaning flutes with a sponge. Moreover an increased amount and frequency of irrigation will remove debris eventually pushed apically and/or left inside canal in the coronal/middle parts, before instrument is reaching the apex. Manual insertion allows a controlled engagement, since the instrument will only cut and progress one mm deeper when activated. The MIMERACI approach is one step, which must be repeated many times till the instrument reaches the working length, aiming at reducing metal stress and improving root canal debridement. In the present study the MIMERACI technique is compared with a traditional instrumentation technique, using the same NiTi instruments and the same motor motion. The null hypothesis is that MIMERACI technique would not influence the quantity of the extruded debris that elicit postoperative pain.
Materials and methods
The present study follows the same methodology used by authors in previous clinical studies, which compared the influence of different motor motions and instruments in the post operative pain. One hundred permanent, premolar and molar teeth requiring endodontic treatment, were included in the study. Patients ranged in age from 18 to 76 years (average 47,9 years), and all were in good health, as determined from a written health history and oral interview. Patients who had in the previous days taken antibiotics or analgesics were excluded. Age, gender, tooth location, pulp vitality and radiographically visible lesions were recorded. An electric pulp-testing device (Elements pulp vitality tester, Sybron endo, Orange, Ca) was used pre operatively to assess pulp vitality in all teeth. Only non-vital, necrotic teeth were included in the study.
Before initiating treatment, each tooth was examined according to clinical complaints, including the presence or absence of pain. Overall, 64 patients had symptomatic (preoperative pain, spontaneous or after chewing) and 36 had asymptomatic teeth, respectively. Of the 100 teeth previously diagnosed as nonvital, 79 showed periapical lesions.
A single clinician evaluated all patients, using radio- graphic and clinical findings, and the same clinician was assigned for treatment of all cases. This procedure was performed to eliminate or minimize interpersonal variability in the treatment between clinicians.
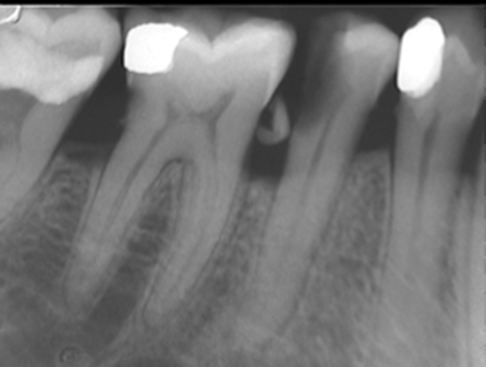
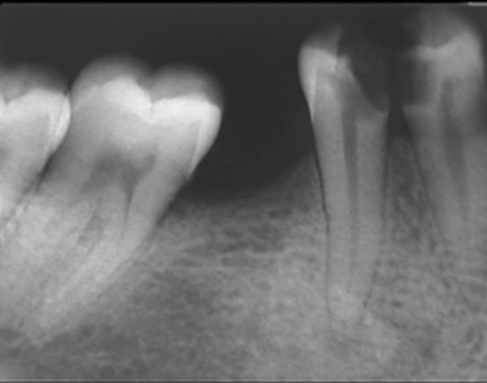
The teeth were assigned into two groups of 50 teeth each, trying to make the groups very similar, concerning the number of root canals, presence of initial pain and periapical lesions (Fig. 2,4). After isolation and access, the canals of all teeth were prepared using two different instrumentation techniques, irrigated with 5% NaOCl and 17% EDTA, and obturated with guttapercha and a zinc oxide eugenol sealer using warm vertical compaction. For all teeth an initial manual glide-path with stainless steel k-files up to size #15 was performed .The teeth in group 1 (n = 50) were shaped using TF Adaptive motor (Kerr Endodontics, Orange, Ca) and TF Adaptive ML1 and ML2 instruments (25.08 and 35.06), using a crown-down technique. Instruments’ clinical motion was performed using the following manufacturers instructions as reported at www.kerrdental.eu: “Slowly Advance. Apply single controlled motion. Wait until the files engages dentine and then withdraw file from the canal. Repeat process until the file reaches the working length”. The teeth in group 2 (n = 50) were shaped with the same instruments, sequence and Adaptive motor, but a MIMERACI technique, as previously described, was used for all instruments.
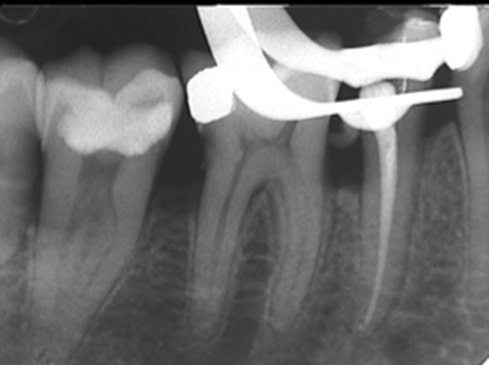
All canals were shaped, cleaned and obturated in a single-visit (Fig. 3,5). Although no systemic medication was prescribed, the patients were instructed to take mild analgesics (400 mg of Ibuprofen), if they experienced pain. The assessment of postoperative pain was carried out at 3 days after initial appointment by one independent evaluator without knowledge of visit group under examination. The presence or absence of pain, or the appropriate degree of pain was recorded as none, slight, moderate, or severe, by using a visual analogue scale (VAS), validated in previous studies:
- No pain: the treated tooth felt normal. Patients don’t have any pain.
- Mild pain: recognizable, but not discomforting, pain, which required no analgesics.
- Moderate pain: discomforting, but bearable, pain (analgesics, if used, were effective in relieving the pain).
- Severe pain: difficult to bear (analgesics had little or no effect in relieving the pain).
VAS pain scores were compared using one-way ANOVA post hoc Tukey test. A value of p < 0.05 was required for statistical significance.

Results
Results are shown in Table 1. For VAS pain scores a statistically significant difference was found between the two groups (p=0,031). MIMERACI instrumentation technique showed significantly better results. When evaluating patients experiencing moderate or severe pain the incidence and intensity of symptoms was significantly lower with the MIMERACI technique. Overall, flare ups occurred in only 3 patients, but none treated with the MIMERACI Technique.
Discussion
It is quite a common experience during endodontic instrumentation hands-on courses on extracted teeth, that participants visualize the creation of the “endodontic worm”, a tubular mass of canal debris produced primarily by debris propelled through the apical foramen by forceful instrumentation, improper irrigation, and a lack of recapitulation. In clinical practice this worm of debris includes bacteria, dentin chips, irrigants, and inflamed or dead pulp, that when pushed into the periapical tissues may elicitate postoperative pain.
Table 1. Overall incidence of post operative pain. | ||||
Group | No pain | Mild | Moderate | Severe |
A | 22(44%) | 13(26%) | 12(24% ) | 3(6%) |
B | 26(52%) | 15(30%) | 9(18 %) | 0(0%) |
This worm is more likely to occur when reciprocation motion is used, because the flutes are designed to remove debris only in one direction. Therefore, while the cutting angle removes debris coronally, the releasing angle tends to push debris apically. However, the tendency to push debris apically also depends on many other factors: single-file technique, dimensions of instrument, cutting tip, and different reciprocating angles. In previous studies, reciprocating single-file techniques (Reciproc and WaveOne) were found to produce a more significant inflamatory response and pain when compared to a rotary nickel-titanium crown down instrumentation technique. WaveOne (Dentsply-Maillefer, Ballagues, Switzerland) and Reciproc (VDW, Munchen, Germany) techniques use a quite rigid, single-file of increased taper (usually 07/08 taper, size 25) with 16 mm working part. Since instruments are used without any preliminar coronal enlargement, progression to the apex often results in a greater engagement of flutes and, consequently, more debris are entrapped, requiring more torque or applied pressure to reach the working length. This can be minimized by a cutting tip, which decreases the operative torque needed, but the cutting tip produces more apical debris. In many cases, in order to reach working length, these reciprocating instruments are used with force directed apically, which makes an effective piston to propel debris from a patent apical foramen.
The TF Adaptive technique was proposed in order to maximize the advantages of reciprocation, while minimizing disadvantages, including the apical extrusion of debris by using a unique, patented motion, which was developed to channel more debris coronally. Moreover, TFA uses more flexible instruments with a non-cutting pilot tip and shorter working part, and a sequence which is designed to make progression to working length less stressful. In a previous study TFA instrumentation technique was found to elicit similar post-operative pain when compared to continuous rotation. No statistical significant differences were found between the two techniques for both incidence and intensitivity of postoperative pain. On the contrary both techniques were found to produce less post-operative pain when compared to the Reciproc technique.
Besides all these improvements which are due to products’ innovations, also clinicians may contribute in reducing postoperative pain. This goal can be achieved by clinically using the instruments with an operative technique which tends to minimize debris production and improve debris removal. The MIMERACI technique is designed to achieve both these goals, starting from minimizing files’ engagement and consequently production of debris. A frequent withdrawing the file from the canal after such a small engagement, keeps most of the debris entrapped within the flutes. Cleaning the flutes outside the canal by using a sponge or a suction device makes debris removal more predictable and effective. Irrigating so often helps both dissolution and removal of debris left inside canals, due to an increased volume and efficacy of the refreshed irrigating solution. The manual insertion is also important because it helps clinicians to feel blade engagement in an easier and safer way. It also helps controlling the minimal (1mm) advancement inside the canal, allowing a predictable engagement which minimize mechanical stress. This could be also achieved with the insertion of a file rotating, but speed would reduce tactile feedback, control and increase the tendency of the instrument to screw in.
Are you interested in an effective alternative to traditional techniques in endodontic treatment? Lasers are revolutionizing dentistry, offering innovative solutions that excel in their ablation, penetrability, and disinfection capabilities, making them a game-changer. Discover why lasers are the future of dentistry by enrolling in the "Laser Therapy in Endodontics and Restorative Dentistry" course and learn the techniques for laser root canal disinfection and laser-assisted endodontics for management of resorption, perforations, and broken instruments.
Results from the present study rejected the null hypothesis and showed that MIMERACI technique significantly reduced postoperative pain, probably due to a combination of many factors: better mechanical removal of debris, more efficient irrigation during instrumentation and less production of debris. All these factors could reduce the risk of apical extrusion of the debris, but also the risk of pushing and packing debris laterally, thus making canal debridement and disinfection more effective. These preliminar positive clinical findings should be also correlated with further in vitro studies aiming at showing in extracted teeth less extrusion of debris or less remnants of debris inside canal space.
Authors: G. Gambarini , D. Di Nardo, G. Miccoli, F. Guerra, R. Di Giorgio, G. Di Giorgio, G. Glassman, L. Piasecki, L. Testarelli
References:
- Plotino G, Grande NM, Cordaro M, et al. Measurement of the trajectory of different NiTi rotary instruments in an artificial canal specifically designed for cyclic fatigue tests. Oral Surg 2009; 108:152-6
- Plotino G, Grande NM, Cordaro M, et al. Review of cyclic fatigue testing of nickel-titanium rotary instruments J Endod 2009; 35:1469-76
- Gambarini G, Gerosa R, De Luca M, et al. Mechanical properties of a new and improved nickel-titanium alloy for endodontic use: an evaluation of file flexibility. Oral Surg 2008; 105:798-800
- Berutti E, Paolino DS, Chiandussi G, et al. Root canal anatomy preservation of WaveOne reciprocating files with or without glide path. J Endod 2012; 38:101-4
- Bürklein S, Schfer E. Apically extruded debris with reciprocating single-file and full-sequence rotary instrumentation systems. J Endod 2012; 38:850-2
- Oginni A, Udoye C. Endodontic flare-ups: comparison of incidence between single and multiple visit procedures in patients attending a Nigerian teaching hospital. BMC Oral Health 2004; 4:4-6
- Siqueira JF, Jr Rocas IN, Favieri A, et al. Incidence of postoperative pain after intracanal procedures based on an antimicrobial strategy. J Endod 2002; 28:457-60
- Plotino G, Grande NM, Melo MC, et al. Cyclic fatigue of NiTi rotary instruments in a simulated apical abrupt curvature. Int Endod J 2010; 43:226-30
- Al-Sudani D, Grande NM, Plotino G, et al. Cyclic fatigue of nickel-titanium rotary instruments in a double (S-shaped) simulated curvature. J Endod 2012; 38:987-989
- Testarelli L, Plotino G, Al-Sudani D, et al. Bending properties of a new nickel-titanium alloy with a lower percent by weight of nickel. J Endod 2011; 37(9):1293-5
- Kim HC, Kwak SW, Cheung GS, et al. Cyclic fatigue and torsional resistance of two new nickel-titanium instruments used in reciprocation motion: Reciproc versus WaveOne. J Endod 2012; 38:541-4
- Pedullà E, Grande NM, Plotino G, et al. Cyclic fatigue resistance of two reciprocating nickel-titanium instruments after immersion in sodium hypochlorite. Int Endod J 2013 Feb;46(2):155-9
- Plotino G, Grande NM, Testarelli L, et al. Cyclic fatigue of Reciproc and WaveOne reciprocating instruments. Int Endod J 2012; 45:614-618
- De-Deus G, Barino B, Zamolyi RQ, et al. Suboptimal debridement quality produced by the single-file F2 ProTaper technique in ovalshaped canals. J Endod 2010; 36:1897-900
- Gambarini G, Al Sudani D, Di Carlo S, et al. Incidence and intensivity of postoperative pain and periapical inflammation after endodontic treatment with two different instrumentation techniques. Europ J Inflam 2102; 10:99-103
- Gambarini G, Testarelli L, De Luca M, et al. The influence of three different instrumentation techniques on the incidence of postoperative pain after endodontic treatment. Annali di Stomatologia 2013; IV (1):138-41
- Kustarci A, Akdemir N, Siso SH, et al. Apical extrusion of intracanal debris using two engine driven and step-back instrumentation techniques: an in-vitro study. Eur J Dent 2008; 2:233–9
- Elmsallati EA, Wadachi R, Suda H. Extrusion of debris after use of rotary nickel-titanium files with different pitch: a pilot study. Aust Endod J 2009; 35(2):65–8
- Vaudt J, Bitter K, Neumann K, et al. Ex vivo study on root canal instrumentation of two rotary nickel-titanium systems in comparison to stainless steel hand instruments. Int Endod J 2009;42:22–33