
Treatment protocol for unilateral posterior crossbite
Machine translation
Original article is written in RU language (link to read it) .
Posterior crossbite during the period of mixed dentition must be corrected as early as possible, as this ensures the correct positioning of the bones, teeth and temporomandibular joint during the growth and development of the entire dental system. This article reports on a 9-year-old patient with a functional unilateral posterior crossbite who was treated with a modified Hyrox expansion screw. The article discusses a simple, inexpensive and effective treatment protocol. The pathology was corrected by actively loosening the screw for 15 days, using it for retention for 5 months and observing for 5 years after the end of treatment.
Learn more about this topic in the webinar Unilateral crossbite: etiology and principles of treatment .
The consistency of the result during long-term treatment largely depends on early diagnosis and timely elimination of the etiological factor, as well as on the use of the correctly selected device.
Posterior crossbite can be defined as a transversal discrepancy between the jaws; this phenomenon is observed in children with both primary and mixed dentition with a prevalence of 7 to 23%. This type of malocclusion is common, so correcting it is an important task for pediatric dentists.
This prevalence of the disease makes this malocclusion a particularly important challenge for practicing pediatric dentists.
Children suffering from this malocclusion have a narrowed craniofacial complex.
The etiology is multifactorial and includes mouth breathing, muscle dysfunction, and/or long-term sucking habits. Among all cases of posterior crossbite, 97% of individuals present to us with premature fissure-tubercle contacts during habitual movements of the lower jaw, which creates a lateral displacement, establishing a functional unilateral crossbite. Tomographic studies have shown condylar asymmetry in children with posterior decussation, but symmetry is restored after treatment. If this condition is not treated, the condyle may undergo restructuring as the child grows to compensate for the asymmetry. Self-correction is rare; it is believed that during the correction of malocclusion during the period of growth and development, problems associated with the craniomandibular skeleton are solved. Most cases of functional posterior bite require a maxillary expansion device.
Although a large number of articles have been published on this issue, the purpose of this article is to report a simple, inexpensive, and effective protocol for the treatment of functional posterior bite by today's clinicians.
Case Description
The patient is a boy aged 9 years and 10 months with a complaint of an aesthetic defect when smiling; was examined in the preventive orthodontics program at the Arazatuba Dental School of the State University of São Paulo.
Diagnostics
Initial intraoral assessment revealed that the patient was in the first stage of mixed dentition. There was a lack of space for a permanent maxillary right lateral incisor. The posterior chiasm extended from the primary canine to the permanent first molar, and on the left side there was only the primary canine in the chiasm. There was excessive lingual inclination of both the maxillary and mandibular alveolar processes, as well as slight midline deviation in the position of centric occlusion (Fig. 1).

Fig.1
On the right, despite the decussation, the normal sagittal relationship of the primary canines, a slight mesial inclination of the second primary molar and the position of the first permanent molar according to the first class of the Engle classification are shown (Fig. 2).

Fig.2
On the left side, a normal sagittal relationship of the primary canines was revealed, despite their complete decussation, and the primary and permanent molars were in a normal position (Fig. 3).

Fig.3
Moderate crowding was detected between the permanent maxillary central incisors (Fig. 4).

Fig.4
The described clinical signs were observed in the patient in the position of central occlusion. Dynamic analysis demonstrated differences in mandibular position during centric relation and centric occlusion, which is an important factor in determining functional occlusion. The diagnosis was made: posterior functional crossbite with a favorable prognosis.
Crossbite treatment
The crossbite was treated using a modified Hyrax expansion screw. The device was created using a 9 mm expansion screw held on the primary molars and canines using rigid wires (the ring was cemented on the second primary molars using glass ionomer cement) (Fig. 5).

Fig.5
Sequence of treatment
Sequence of treatment:
- introduction of the Hyrax device;
- occlusal radiography before expansion (Fig. 6);
- 2 activation turns at 1/4 per day, one in the morning and one in the evening;
- grinding of temporary canines to remove blockage of expansion;
- achieving transverse hypercorrection (Fig. 7);
- occlusal radiography after final expansion (Fig. 8);
- retention period for 150 days using the device itself;
- removal of the device and periodic monitoring every 6 months.
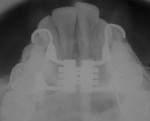
Fig.6

Fig.7

Fig.9
results
Regarding intraoral results, the anterior view showed marked improvement in vertical overlap and restoration of transverse dimension. The vestibular inclination of the teeth was restored, taking into account the morphogenetic development of the upper jaw (Fig. 9). It is noteworthy that the middle line was also centered after correction.

Fig.9
In the occlusal plane, in the initial phase of treatment, a lack of space for the permanent maxillary lateral incisor was evident and crowding of the central incisors was present (Fig. 10). However, then there was a noticeable improvement in the contour of the upper jaw and the axial inclination of the posterior teeth, and an increase in the intercanine and intermolar distances.

Fig.10
The results obtained showed satisfactory stability during the 1-year post-retention period (Fig. 11).

Fig.11
Monitoring performed over the next 5 years revealed that the patient had a normal occlusion (Fig. 12 and Fig. 13) and illustrated the importance of treating this malocclusion at the appropriate time.

Fig.12

Fig.13
Discussion
The treatment protocol described in this article included the use of a fixed device known as a modified Hyrax expander, daily double activations of 1/4 turn until maximum correction was achieved, and retention for 150 days and follow-up every 6 months. This protocol is widely used in this clinical setting and has a high guarantee of success.
The apparatus used was developed on the basis of the Biederman apparatus. It has a simplified form with hooks on the canines and distal leads to the palatal surface of the first permanent chewing teeth. This device has a rigid structure, is easily adapted and fixed to the supporting teeth, is easy to clean and allows precise control of the process, which could otherwise result in over-correction. Various types of appliances, such as an acrylic plate with an expansion screw and a twisted helix, can be used to correct a functional posterior crossbite. The description given in this protocol does not indicate the superiority of one device over another, but offers clinical evidence of a simple and effective treatment method.
A previous study recommended activation of half a rotation per day and used an apparatus with an expander that simulated rapid maxillary extension. In the present treatment protocol, the essence was to use the same number of activations, adjusted for the patient's lack of pain or discomfort. The retention period of 150 days is consistent with the literature, in which the authors conducted a clinical study in children under the same clinical conditions as in this case.
In 2013, Lippold et al. conducted a randomized clinical trial to evaluate the effects of orthodontic treatment in children with primary or mixed dentition with a functional posterior crossover and concluded that the appliances used to correct this problem are effective and improve occlusal relationships and craniofacial growth. The authors emphasized the importance of early orthodontic treatment.
If the patient still has a posterior crossbite at the end of puberty, it will not allow the maxilla to develop normally in the transverse plane. Therefore, a problem of dentoalveolar origin can become a problem for the entire skeleton, which may subsequently require surgical intervention for correction.
According to Pinto et al., 2001, during the period of craniofacial growth, untreated functional posterior crossbite will not result in growth of the unaffected side of the maxilla, while the affected side will show limited growth. Some studies have shown that this growth will cause facial asymmetry.
Children with primary or mixed dentition do not necessarily show signs of craniomandibular dysfunction with this malocclusion pathology; they can develop in a later period of growth. Therefore, early diagnosis and correction of this malocclusion in patients who are in the stage of growth and development of the dentition is vitally important, because the main goal of treatment is the normal development of the craniomandibular skeleton.
Modified Hyrax device
This treatment protocol found the modified Hyrax appliance to be easy to use and effective in correcting functional posterior crossbite in short periods of time. It does not require strict cooperation with the patient.
If you are interested in this topic and want to get acquainted with other treatment protocols, including crossbite, go to the online lesson Crossbite and deep bite: treatment protocols .
http://www.aegisdentalnetwork.com/