
Manifestations of dermatoses on the oral mucosa
Machine translation
Original article is written in RU language (link to read it) .
There is a wide variety of diseases accompanied by skin pathology, but only some of them have typical symptoms on the oral mucosa. This article is devoted to just such diseases - dermatoses, as well as their manifestations in the oral cavity.
More information on various diseases of the oral mucosa and periodontal diseases in our section Training in Periodontology .
Pemphigus
Pemphigus is a collection of bullous dermatoses, the pathogenesis of which is based on the appearance of autoantibodies directed against stratified squamous epithelium of various localizations (skin and mucous membranes of internal organs).

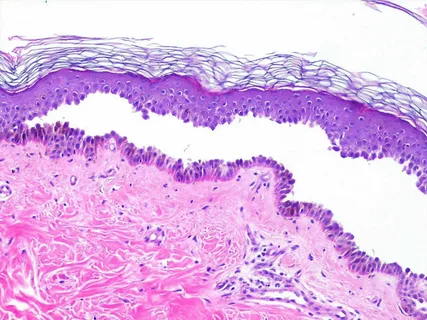
Rice. 1. Erosion on the dorsal surface of the tongue.
Etiology
- Genetic predisposition.
- Insolation.
- Taking medications that contain thiol groups.
- Infectious agents.
- Abuse of certain foods.
- Stress.
- Often the cause cannot be determined.
Pemphigus vulgaris
This disease is characterized by blisters of varying sizes with a relaxed, thinned covering, filled with serous exudate, appearing on intact skin or mucous membranes.
Clinic
- Hypersalivation, bad breath.
- The first blisters are observed on the oral mucosa, on the lips, and within a year the disease spreads to the entire skin.
- The tires quickly burst open, leaving behind painful erosions that do not heal for a long time.
- The blisters on the skin become crusty.
- Erosion has a shiny surface and tends to increase along the periphery.
- Nikolsky's symptom is positive - the epidermis exfoliates under the influence of mechanical stress in the affected area and in distant areas.
Seborrheic pemphigus
Clinic
- It begins with damage to seborrheic areas of the skin (back, chest, face, scalp).
- The first elements of the lesion are clearly defined erythematous lesions covered with yellow or brown-brown crusts.
- The blisters are small and quickly turn into crusts, which, when torn off, leave moist erosions.
- Nikolsky's symptom is positive only in the affected area.
Rice. 2. Formation of a bladder in pemphigus.
Pemphigus foliaceus
Clinic
- Erythematous-squamous rash.
- The blisters have a thin wall, reappear in the same place, when opened, they leave pink-red erosions, and then lamellar crusts.
- Damage to mucous membranes is not typical.
- Typically rapid spread with the development of exfoliative erythroderma.
- Nikolsky's symptom is positive in the affected area and beyond in the healthy area.
Pemphigus vegetans
- Typical localization of blisters is around the mouth, nose, and genitals.
- At the bottom of the erosions, soft, foul-smelling vegetations grow, which are covered with a serous or purulent coating.
- Nikolsky's sign is positive in the affected area.
Pemphigus herpetiformis
- It is a rare bullous dermatosis, clinically resembling Dühring's dermatitis herpetiformis.
- The lesion element is plaques, and papules and vesicles are identified along their periphery.
- Patients report severe itching of the skin.
- In case of progression, the clinical picture resembles pemphigus vulgaris or pemphigus foliaceus.
Paraneoplastic pemphigus
- Often a complication of chemotherapy.
- Often combined with neoplasia, sarcoma, carcinoma.
- The clinical picture is similar to that of pemphigus vulgaris.
Drug-induced pemphigus
- Clinical manifestations are similar to those of pemphigus vulgaris, foliaceus or seborrheic pemphigus.
- Occurs as a result of taking certain drugs: D-penicillamine, pyritol, captopril, β-lactam antibiotics.
- The pathogenesis is based not on autoimmune reactions, but on biochemical reactions.
- After discontinuation of the drugs, complete recovery occurs.
IgA-dependent pemphigus
Refers to intraepidermal bullous dermatoses, accompanied by vesiculopustular lesions, acantholysis, neutrophil infiltration, and the presence of IgA autoantibodies against stratified squamous epithelium.
- Pustules form on intact or moderately hyperemic mucosa.
- The pustules merge to form ring-shaped lesions with crusts in the center.
- Patients report severe itching.
- The course is benign.
Bullous pemphigoid
Refers to skin lesions, characterized by the formation of subepidermal blisters in response to the production of autoantibodies to hemidesmosomes.
Risk factors
- taking certain medications: penicillins, cephalosporins, nifedipine, aspirin, furosemide, influenza vaccine,
- viral infections,
- long-term exposure to physical agents: radiation therapy, UV irradiation, electrical or thermal burns.
Clinical picture
- The general condition does not suffer.
- Bubbles up to 10 mm in diameter appear on the hyperemic epidermis, have the shape of spheres, the cover is smooth, filled with serous secretion, sometimes mixed with blood.
- Erosion at the site of opened blisters heals quickly.
- The contents of the blisters dry out, leaving behind crusts, which, when peeled off, leave behind pale spots.
- On the epidermis, the lesions practically do not cause pain, unlike skin rashes.
- The disease is characterized by a long-term course with periods of remission.
Dermatitis herpetiformis
A skin lesion of inflammatory origin caused by gluten enteropathy; it is characterized by polymorphic rashes that cause significant discomfort to the patient and a chronic course with frequent relapses.
The pathogenesis is based on the sedimentation of immune complexes in the papillae of the dermis, activation of the chemotaxis process of neutrophils, the latter triggering the proteolytic destruction of the basement membrane. The result of the pathological process is subepidermal blisters.
In addition to the skin, the oral mucosa is affected; the typical localization of the affected elements is the cheeks and palate.
Clinic
- Vesiculobullous rashes are characteristic, characterized by a dense covering and the formation of erosions after opening.
- Erosion on the skin epithelializes, leaving behind weakly pigmented spots and, in rare cases, scars.
- The bubble size does not exceed 5 mm.
- Bubbles on the mucous membrane are surrounded by slight hyperemia, and slight swelling is detected.
- Acantholysis is not common.
- Nikolsky's symptom is negative.
- There is practically no pain syndrome.
- Epithelization of erosions on the mucous membrane occurs within a few weeks, and they heal without leaving marks.
Systemic lupus erythematosus
A skin lesion belonging to the group of collagenoses, rashes are detected both on the skin and on the mucous membranes.
Clinic
- Whitish or bluish-red plaques with a clear outline, the center of which sinks, erosion can form in it.
- Patients experience pain when eating.
- Typical “lupus” spots are foci of hyperkeratosis, bordered by a rim of hyperemia, noted on the mucous membrane of the cheeks in the distal sections along the line of closure of the teeth.
- Keratotic growths are not removed by scraping.
- All forms are characterized by atrophy.
- During the period of remission, cicatricial atrophy and scar cords remain at the site of the lesion.

Rice. 3. Systemic lupus erythematosus.
Psoriasis
Papulosquamous skin disease.
Clinic
- Monomorphic rashes, represented by flat papules, the latter can merge into a single plaque.
- Typical localization is the mucous membrane of the tongue.
- The plaque on top is covered with loose scales.
- The pustular form is characterized by the appearance of small painful pustules against the background of local hyperemia; the surrounding mucosa is intact and is not involved in the pathological process.
- Nonspecific manifestations in the mouth: folded tongue, “geographical” tongue, erythema migrans.

Rice. 4. Manifestation of psoriasis on the hands.
Lichen planus
The main risk factor is trauma to the mucous membrane from fillings, dentures, sharp edges of teeth, and galvanosis.
Typical clinic shape
- The course is asymptomatic, rarely discomfort from spicy foods.
- Gray-white polygonal knots are combined into a single pattern, forming lace or a network.
- The surrounding mucosa is not involved in the process.
- Typical localization: cheeks, back of the tongue, line of closure of teeth, rarely – palate.
Clinic of hyperkeratotic form
Foci of keratinization unite into clear stripes, causing dryness of the mucous membrane, patients complain of roughness, and a burning sensation in the oral cavity may occur.
Clinic of exudative-hyperemic form
- Patients complain of discomfort when eating, redness and burning in the mouth.
- Papules characteristic of lichen planus are located on edematous and moderately hyperemic mucosa.
- Often pathological changes are localized in the area of contact of the mucous membrane with the prosthesis material, on the lips and cheeks.
Clinic of erosive-ulcerative form
- All patients complain of pain.
- Against the background of a typical picture, erosions of irregular polygonal shape appear, with granulations covered with fibrinous plaque. If injury occurs to the elements of the lesion, bleeding may develop.
Clinic of bullous form
- Doesn't happen often.
- Patients report discomfort.
- Along with typical rashes, blisters are detected, the size of which can reach 1 cm and persist for no longer than a day.
- Erosion formed after the opening of the blisters quickly epithelializes.

Rice. 5. Examination of the oral mucosa.
Atypical clinic
- Patients complain of pain.
- Atypical location: upper lip and gums.
- The lesion in the center of the lip, above the surrounding mucosa, is covered with a whitish coating, and congestive hyperemia is noted at the base.
- The gingival papilla between the central incisors is hypertrophied and covered with a pale whitish mesh.
If you are interested in this article and want to receive more useful information on various areas of dentistry, look for training that is interesting to you on our website .