
Finding the central relation. Kois Deprogrammer
Machine translation
Original article is written in RU language (link to read it) .
Finding the central ratio can sometimes seem like a difficult task, but with the right tools, such as the Kois deprogrammer, the process becomes clear and simple.
You will learn more about Kois' principles in the online course Kois' Principles: Digital Planning of Orthopedic and Orthodontic Treatment .
The centric relation (CR) can be defined as the physiological position of the head of the condylar process of the mandible in the glenoid fossa when the joint occupies its maximum superior posterior position.
Many studies regarding total oral work associated with increased occlusal height have shown that it is preferable to plan such cases in the CS position. Finding CS is well described in the literature, however, clinical success is often elusive.
However, anyone who has worked with patients knows that some of them find it extremely difficult to place their jaws in the CS.
The Kois deprogrammer is an effective device for registering a CA.
What is it?
The Koys deprogrammer is a removable plastic device that covers the hard palate and creates a single point of contact between the lower central incisors and the anterior bite platform.
How to make a Kois deprogrammer?
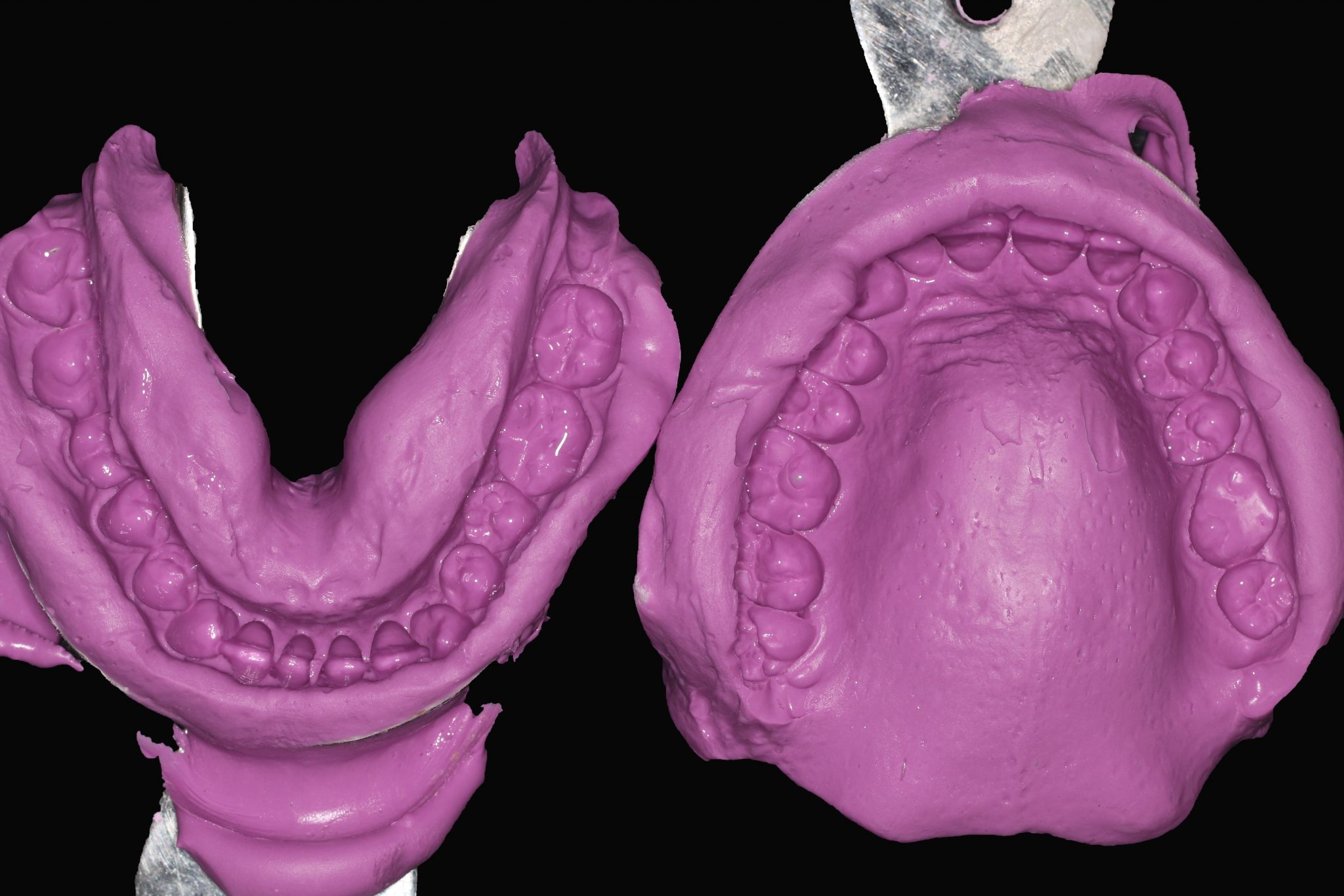
Figure 1: Alginate impressions of the maxilla and mandible should be obtained.

Figure 2. Making a plaster model.

Figure 3. The model is carefully trimmed.
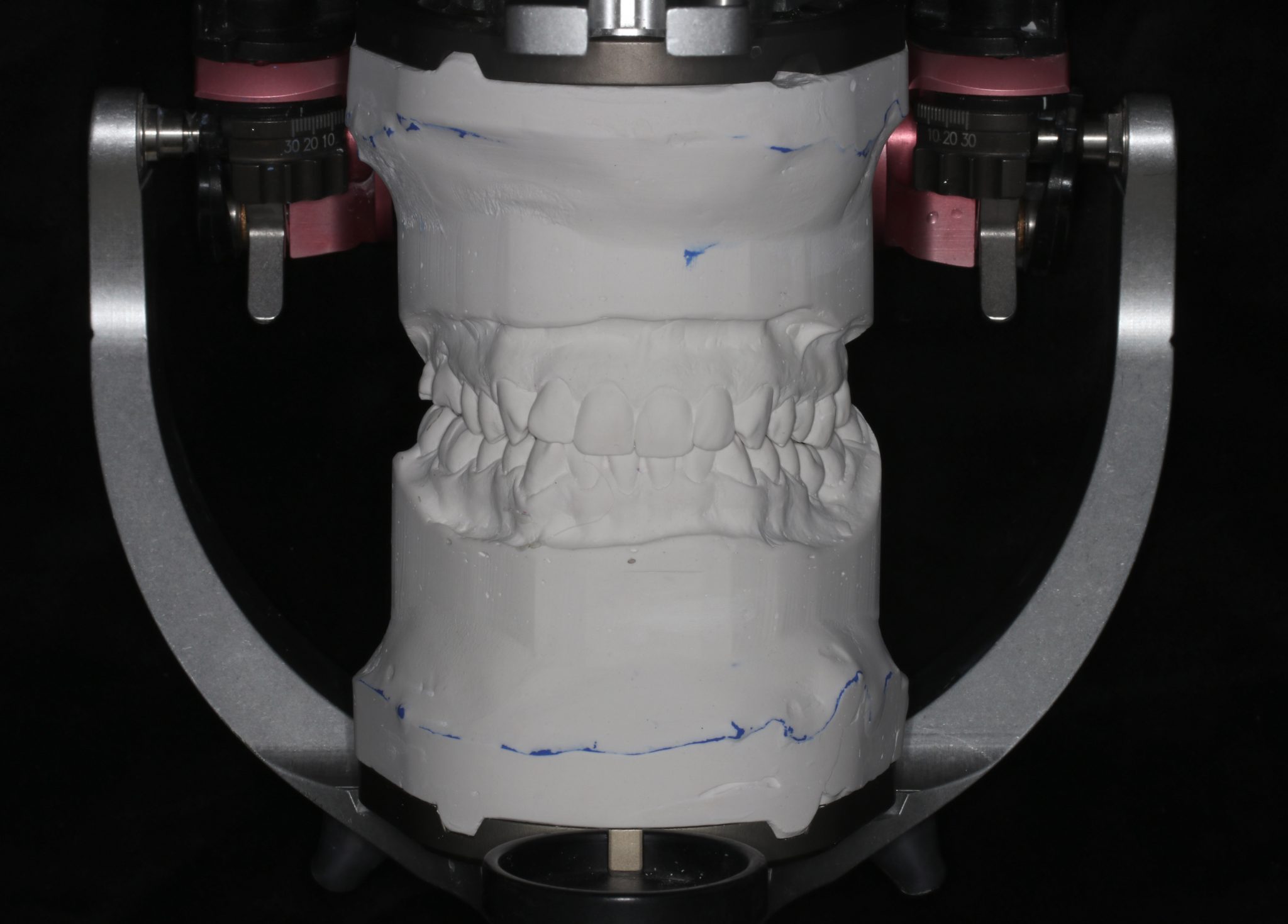
Figure 4. The impressions are then placed in the articulator at maximum fissure-tubercle contact. A facebow and occlusion recorders are not needed.

Figure 5. The vestibular arch of the device is made of wire; it should not touch the occlusal surface of the teeth.
The vestibular arch controls retention and stabilization of the appliance within the patient's mouth.

Figure 6. A horseshoe-shaped base with a platform for the central lower incisors is made from acrylic plastic.

Figure 7. The width of the platform is 3 mm, the platform should be parallel to the vestibular arch. Its purpose is to separate the bite by 1.0-1.5 mm.

Figure 8. Polishing.

Figure 9. How to use the Kois deprogrammer?
After receiving the device from the laboratory.
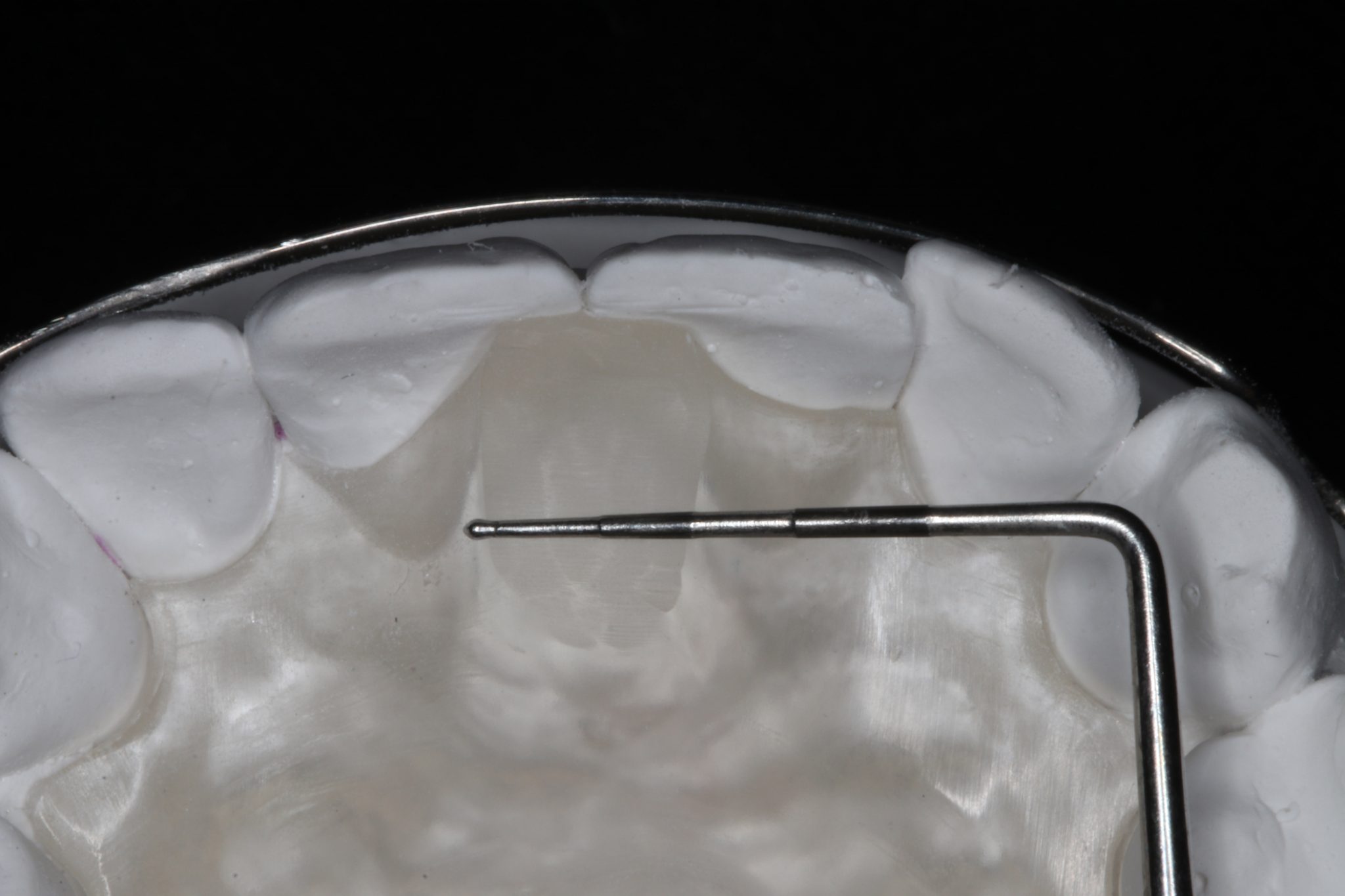
Figure 10. Checking the platform width (no more than 3 mm).
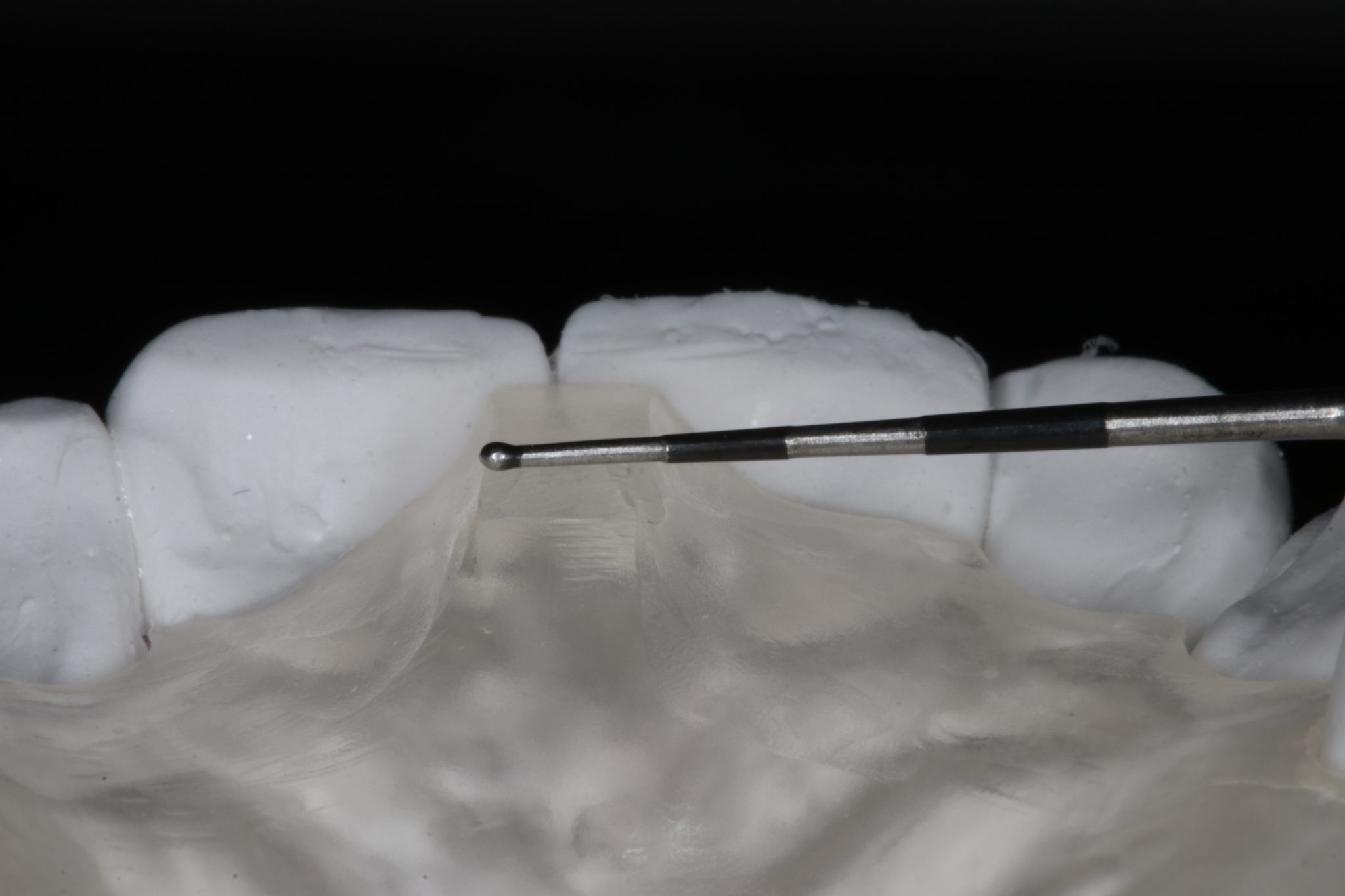
Figure 11. If it is wider than 3 mm, it should be narrowed.

Figure 12. Checking the device in the oral cavity.

Figure 13. Stabilization of the apparatus in the oral cavity is achieved through a plastic base on the palate and vestibular arch.

Figure 14. Bite separation by 1.0-1.5 mm.

Figure 15

Figure 16. The patient should then sit back in the chair; he should be asked to bite down on the articulation paper and move his jaw back and forth.

Figure 17. Removing excess material from the palatal surface.

Figure 18: The contact on the platform should be tapered so that it touches the midline of one of the lower incisors.

Figure 19. When the patient closes his mouth and the same initial contact is confirmed, the patient is “deprogrammed.”
Repeatability is a key criterion for determining when a patient is deprogrammed.
conclusions
How long should I wear the deprogrammer?
It is worn until the necessary muscle deprogramming is completed (days or weeks, usually 2-4 weeks are needed). Some patients may need to wear the device up to 24 hours a day (removed for meals) so that old muscle memory is erased and replaced with new muscle memory.
Deprogramming Confirmation
The initial point of contact should be marked as the patient closes the mouth using articulation paper.
When the patient closes his mouth and the same initial contact is confirmed, the patient is deprogrammed (Fig. 19). Repeatability is the key criterion.
The Kois deprogrammer has several uses:
- It can be used as a diagnostic tool to determine whether the mandible should move forward or backward to achieve centric relation at maximum fissure-tubercle contact.
- This is an invaluable tool for diagnosing the most common types of pathological wear: occlusal dysfunction, parafunction (bruxism).
- Bite registration using the Kois Deprogrammer allows you to control your bite height.
- The device facilitates the search for premature contacts - that is, any contact encountered during the closure of the lower jaw in the correct position of the joint in the glenoid fossa.
Are there any contraindications for the Kois deprogrammer?
- In case of TMJ problems, the patient needs a posterior support and a Michigan splint
- Damage to periodontal tissue in the area of the lower incisors. In this case, splinting of the teeth of the lower jaw or Michigan splint is used.
- The patient has a gag reflex. Try reducing the size of the acrylic base to avoid extensive contact with the soft palate.
More relevant information on this topic at the webinar : Ideal bite height and centric relation in the treatment of pathological abrasion in the concept of D. Koys .
http://www.styleitaliano.org/