
Features of wound care and healing after complex removal
Machine translation
Original article is written in RU language (link to read it) .
Tooth extraction is the most common surgical procedure, which is most often performed not only among dentists, but also in medical practice in general. Surgical intervention, the purpose of which is to remove a decayed tooth, requires following the general principles that are mandatory when performing any other operation.
More detailed information on this topic in the webinar Protocols for tooth extraction in complex clinical cases .
Complex tooth extraction, also called open or surgical, involves additional surgical manipulation - cutting out and detachment of the mucoperiosteal flap, after which osteoectomy is often required, which is performed using a chisel and hammer or a drill.

Figure 1. Complex tooth extraction.
Indications for complex removal
Unsuccessful tooth extraction over a long period of time using the traditional closed method.
Semi-retention or tooth retention is most common among canines and wisdom teeth.
Significant curvature of the roots of the tooth being removed, if during the usual method of removal a root fracture occurred that cannot be removed.
Hypercementosis is most often found among patients with metabolic pathologies.
Teeth after impregnation treatment.
True exostoses.
Molars whose roots are located in the maxillary sinus.
Sequence of stages of complex removal
At the first stage, the dental surgeon performs local anesthesia.
Next, an incision is made in the area of the alveolar process of the mucosa and periosteum, followed by cutting out a mucoperiosteal flap. The design of the latter is determined by the topographic and anatomical characteristics of the operated area and localization.
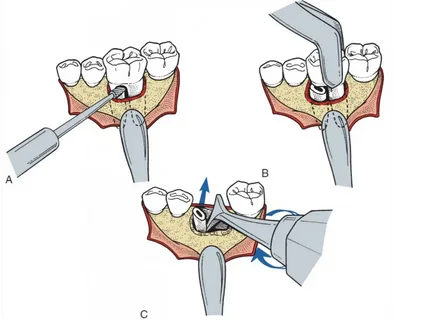
Figure 2. Schematic representation of the stages of a complex tooth extraction.
The following types of cuts are possible:
An arched flap, often referred to in the literature as a tongue-shaped flap, is most popular when it is necessary to remove roots or impacted teeth.
The trapezoidal flap is the most popular type and is used most often.
A rectangular flap from the necks of teeth is used in a situation where jaw atrophy is clinically determined and the alveolar process is shortened.
Triangular flap.
It is important to consider that the mucosal incision should be wider than the bone wound by a width equal to approximately the width of the crown of one tooth on both sides.
Subsequent stages of the operation
The mucoperiosteal flap is peeled off using a rasp.
Using a drill, trephination and subsequent osteoectomy of the outer cortical plate of the alveolar process of the jaw are performed.
The roots of the tooth are exposed and extracted using an elevator. To prevent breakage, the roots of multi-rooted teeth are recommended to be sawed with a drill and removed one at a time using an elevator.
After all the roots have been extracted, the sharp edges of the bone wound are smoothed with a surgical cutter.
If necessary, a revision of the wound is performed, granulations and bone fragments are removed.
Next, stitches are applied and the wound is sutured.
Wound care after complex removal
Inspection and antiseptic treatment of the wound is carried out the next day after surgery. Postoperative swelling of the surrounding tissues persists for three days. Painkillers and antibiotics are prescribed individually if indicated. Sutures are removed one week after surgery.
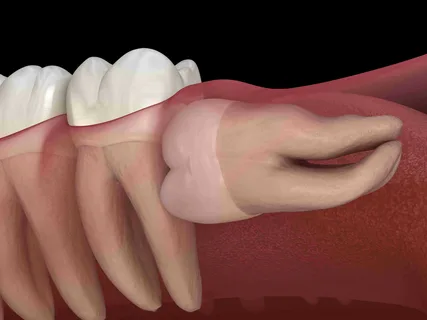
Figure 3. One of the indications for complex tooth extraction.
Wound healing after tooth extraction
In the absence of complications, the socket of the extracted tooth is filled with a blood clot. The presence of a blood clot represents the most optimal and natural healing option. Healing occurs by secondary intention.
Processes undergone by the socket of an extracted tooth
On days 3-4, under a microscope, the formation of granulation tissue is visible, which begins to gradually grow inside the blood clot.
The following types of granulations are distinguished:
fine-grained;
medium-grained, represent the most optimal variety;
coarse-grained, occur if there are inflammatory phenomena in the healing zone.
By the end of the second week, the socket is covered with epithelium, and over the next three months, young bone beams are formed, which on an x-ray have the appearance of young bone tissue.
Within six months, the entire hole is filled with bone tissue, the full maturation of which will occur only after a year.
Along with the process of filling the socket with bone tissue, resorption of damaged sections of the walls of the socket, separately lying bone fragments, and the edges of the alveoli is observed. As a result of all the above processes, restructuring occurs in this area of bone tissue.
As the alveolus is filled with bone tissue, its edges become lower, and the alveolar process in this area becomes thinner. Its height is reduced by a third. The wound heals by primary intention or secondary if no stitches are applied.
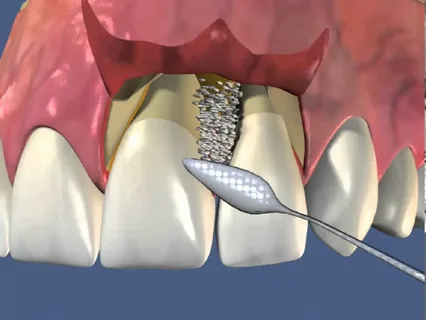
Figure 4. Trapezoid flap.
The following stages are distinguished in the healing process of the hole:
The first stage, the duration of which can be from six to fourteen days, when the contents of the hole have not yet been completely covered by the epithelium. The period is characterized by the simultaneous occurrence of several processes at once: resorption, resorption, regeneration. The blood clot dissolves, fragments of bone tissue that accidentally fell into the socket, and damaged areas of the socket itself are destroyed. Granulation tissue is intensively formed. Healing proceeds according to the type of secondary healing.
The second stage occurs from the second to the sixth week, characterized by intense regeneration processes, and the formation of osteoid tissue begins.
At the third stage, processes of restructuring of the formed bone tissue occur, which gradually acquires a structure identical to the bone tissue of neighboring holes.
Six weeks later, at the site of the socket of the extracted tooth, a formation is detected that is sufficiently stable to be subjected to mechanical influence (prosthetics), however, the mechanisms of bone tissue restructuring continue, so subsequent changes are possible.
Features of wound healing against the background of infection
Any infectious process, either one that occurred before the tooth extraction operation (with periostitis) or one that was added from the outside, has an adverse effect on the healing processes. This can cause a prolongation of the healing period and the addition of unwanted complications.

Figure 5. Size of the mucoperiosteal flap for complex tooth extraction.
At later stages, there is no significant difference between the healing of an infected wound and natural, uncomplicated healing. If a wound becomes infected, the rate of its healing slows down significantly; this is characterized by late formation of granulations, slow growth of the gingival epithelial cover, and delayed formation of osteoid tissue.
If there are no complications, healing of the hole occurs painlessly.
If there was a complex traumatic removal, it causes the following complications:
slowing down the healing process,
attachment of a painful component,
larger area of bone resorption,
alveolitis,
alveolar osteomyelitis due to the absence of a healthy formed blood clot.
Features of removal against the background of concomitant pathology
When performing any surgical procedure, including tooth extraction, it is necessary to pay special attention to patients with a history of concomitant pathology. It can be:
heart disease,
circulatory system,
endocrine system,
liver,
allergic reactions,
mental illness.
If, during the collection of anamnesis, a concomitant disease was identified in the patient, then before performing surgery it is necessary to consult with specialists.
If tooth extraction causes aggravation of somatic pathology or, conversely, a systemic disease causes complications of the operation, then the patient needs appropriate therapy. For such patients, tooth extraction is carried out as planned, against the background of preliminary medicinal preparation. In such situations, the psychological attitude and support of the patient have a great influence, which can often prevent many complications associated with systemic diseases.
If necessary, the patient may be recommended to take sedatives on the eve of surgery. During the operation, it is important to maintain constant contact with the patient, clarify his well-being, try to calm him down, and distract him from negative thoughts.
Even more relevant information at the webinar Using PRF for complex tooth extractions .