
Features of the structure of toothless jaws
Machine translation
Original article is written in RU language (link to read it) .
As a result of the complete absence of teeth, the maxillofacial system undergoes significant functional changes, which trigger the processes of atrophy of the bones of the facial skull, as well as the soft tissues surrounding them.
Read more about the modern protocol for working with patients with complete edentia in the online course Removable dentures.
For patients with complete loss of teeth, the following anatomical and topographic changes are characteristic:
the edges of the eyelids droop
nasolabial folds are pronounced,
the tip of the nose is drooping,
the corners of the mouth are downturned,
the size of the lower third of the face becomes significantly smaller,
the facial expression becomes senile due to sagging muscles.
For the upper jaw, atrophy of the bone of the alveolar process on the vestibular surface is more typical, for the lower jaw - on the lingual surface; as a result of these pathological processes, senile progeny develops.
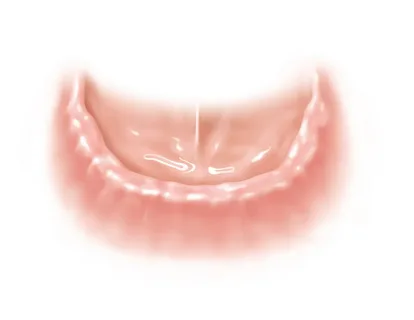
Rice. 1. Toothless lower jaw.
The absence of teeth in the oral cavity leads to damage to the masticatory muscles, and these can be both morphological and functional changes. The volume of muscle tissue decreases due to a decrease in chewing load, and partial atrophy occurs. Pathological processes also start in the temporomandibular joints: the articular fossae become flattened, the articular heads move upward and backward.
As the above pathological processes caused by missing teeth and atrophy progress, orthopedic treatment becomes more complicated, since landmarks that help the doctor determine the height of the lower third of the face and its shape are lost.
Toothless upper jaw. Structural features
When examining the upper jaw, it is important to first evaluate the severity of the frenulum of the upper lip, which is attached at different distances from the apex of the alveolar process and is a narrow and thin cord or fan-shaped formation. The width of the frenulum can reach 7 mm. In some clinical situations, in the area of the arch of the vestibule on the sides of the frenulum, depressions appear; their depth is small, but they are clearly expressed on the impression. It is important to grind off these protruding areas on the prosthesis; this is necessary to prevent injury to the mucous membrane in these areas.
In the lateral parts of the upper jaw there are buccal-alveolar folds. Their number and severity are determined by the severity of atrophic processes. The rational design of the plastic base of a removable denture is hampered by mucosal strands that appear as a result of injuries, operations, burns and other pathological mechanisms.
The pterygomaxillary folds are located behind the tubercle of the upper jaw; they straighten when the mouth is opened wide. All the described anatomical structures are capable of overturning removable dentures or being restrained by them; therefore, it is necessary to take into account these formations when taking impressions and creating the boundaries of removable dentures in the upper jaw.

Rice. 2. Complete denture for the upper jaw.
The bony base of the hard palate along the median suture ends with a protrusion, which in its shape is similar to a tongue. Line “A” represents the boundary of the soft and hard palate.
According to numerous clinical observations, the location of the “A” line is variable, as is its shape. Line “A” can shift up to 20 mm anteriorly, be placed along a conventional line connecting the bases of the tubercles of the upper jaws, or shift towards the soft palate up to 20 mm.
Line “A” is a guideline for planning the posterior edge of a removable denture: in case of complete loss of teeth, the posterior border of the denture overlaps line “A” by 1-2 mm. Blind holes are also used as a guide. The location of the posterior border of the prosthesis depends on one more parameter: the shape and angle of inclination of the soft palate relative to the pharynx.
There are the following types of soft palate shapes:
Steep, when the immobile mucosa turns into mobile mucosa abruptly, along the posterior edge of the hard palate. In this situation, it is almost impossible to lengthen the distal part of the prosthesis, and the palatal valve is represented by a narrow strip.
The gentle slope ensures the formation of the longest palatal valve.
The average slope of the clivus corresponds to the average size of the palatine valve.
In the anterior section of the alveolar process, along the median suture in the area of the central incisors, the incisive papilla is located. With this anatomical formation, transverse folds are also located in the anterior third of the hard palate. All these anatomical structures must be accurately depicted on the impression, otherwise they will be pinched when wearing the prosthesis, causing pain and discomfort in the patient.

Rice. 3. Complete removable dentures.
The torus, or palatine ridge, is the median suture of the hard palate, which is formed during the fusion of the palatine processes of the upper jaws and the horizontal plates of the palatine bones. It has a length equal to the length of the entire hard palate. The palatal ridge is lined with a thin, immobile mucous membrane; the more pronounced this anatomical structure is in the patient, the more unfavorable it is for creating a removable denture. Its height can reach 2 cm, it occurs in 20-60% of the population.
Classification according to the type of torus localization
central - located in the middle of the sky;
posterior - in the posterior third of the palate;
total, occupies almost the entire hard palate.
In the process of modeling the base of a removable denture, if there is a pronounced torus, the dental technician isolates it by placing a lead plate on the model. As a result, a chamber is formed on the plastic prosthesis in the area of the palatal ridge, and the pressure on the mucous membrane and underlying tissues is distributed evenly.
There is also another technique when one to three layers of plaster are glued to the torus in the oral cavity before taking an impression; the thickness of the insulating layer depends on the level of pliability of the mucosa.
Toothless lower jaw. Structural features
Any orthopedist and dental technician knows that on the edentulous lower jaw the border of the removable denture is significantly smaller compared to the upper jaw, which is due to adjacent organs that create obstacles to the application and fixation of the prosthesis, the location of frenulums, cords and other anatomical formations here.
Below we will consider special anatomical areas and spaces that, if possible, are used to increase the area of the prosthetic bed in the lower jaw.

Rice. 4. Complete removable denture for the lower jaw.
The buccal region is an area limited behind by the mucous tubercle of the lower jaw, in front by the buccal cord, below by the vault of the vestibule, and on the sides by the cheeks and alveolar processes. Due to bone tissue atrophy, as well as pathological changes that occur in the surrounding soft tissues, a space of individual size and shape is formed - a buccal pocket or buccal shelf. It is necessary to expand the base of the prosthesis as much as possible in this area in order to obtain a closing valve.
The retromolar region is often used to extend the border of the prosthetic bed in the mandible. Here, the postmolar tubercle is of interest for research - a dense, inflexible or soft and elastic formation, which in any case must be covered with a prosthesis.
The retroalveolar region is limited by the anterior palatal arch, floor of the mouth and root of the tongue. The “wing” of the prosthesis can be placed in this area. To check the possibility of using the retroalveolar region in a particular patient, the following test is used: the index finger is placed in this area and the patient is asked to touch the opposite cheek with his tongue. If the finger does not move, the border of the prosthesis can be placed at the distal border of this area. If the finger is pushed out with the tongue, the “wing” modeling is canceled: the prosthesis will tip over when chewing and speaking.
Quite often, in patients on the lower jaw, one can find peculiar bone protrusions, which are called exostoses. These bone formations can be observed both from the side of the tongue, in this case the exostosis is located closer to the premolars, and from the vestibule of the oral cavity, here they are located closer to the canines and lateral incisors. On the lower jaw, exostoses can be observed - bony protrusions, which on the tongue side are more often found in the area of premolars, and on the vestibular side - in the area of \u200b\u200bthe canines and lateral incisors.
Exostoses do not allow the prosthesis to take a stable position on the prosthetic bed, cause balancing, and as a result the patient receives mechanical trauma to the mucous membrane. To avoid this kind of complications, dental technicians perform isolation of exostoses, this is done using special soft pads. The edges of the prosthesis must overlap these bone formations, otherwise the functional suction will be impaired.

Rice. 5. Ready-made removable dentures.
On the eve of prosthetics, it is important for the doctor to evaluate the anatomical and physiological features of the tongue. The tongue has a significant impact on the fixation of the prosthesis on the lower jaw. The loss of teeth forces the patient to grind food with the tongue, as a result of which the tone increases and the size of the muscles increases. Therefore, the tongue can push out the prosthesis, the stability of the latter will be poor until the tongue adapts to the new position.
Up-to-date information on removable prosthetics in our course Removable dentures for dentists and technicians.