
Condition of the oral cavity with partial loss of teeth
Machine translation
Original article is written in RU language (link to read it) .
Partial tooth loss is a pathological condition that occurs as a result of diseases such as periodontal disease and caries. In itself, partial secondary adentia is not a disease; it is a form of damage to the dental system.
Partial secondary adentia is a defect in the dentition that occurs due to loss of continuity of the dentition as a result of tooth loss.
Read more about the criteria for choosing a future design: removable or fixed prosthesis in the All-on-X online course: a complete guide for surgeons and orthopedists in one course .
Etiology
Reasons associated with the development of the dental system:
primary adentia, caused by the congenital absence of rudiments;
pathology of germ formation (retention).
Reasons associated with tooth loss in a developed dental system:
caries complications;
consequence of periodontal diseases;
surgical operations on the jaws caused by neoplasms, osteomyelitis;
traumatic damage to teeth and bone tissue of the jaws.

Figure 1. Partial secondary edentulism.
Classification
The most popular classification, capable of combining all the variety of dentition defects with partial loss of teeth, is the classification according to E. Kennedy, which was developed on the basis of anatomical and topographical features.
Class I is a bilateral absence of teeth in the end sections of the dentition;
Class II is the absence of teeth at the end of the dentition on one side;
Class III combines included defects, the absence of one or more chewing teeth;
Class IV is an included defect in the frontal part of the jaw.
If a patient has several defects in the dental arch, the condition is classified into a smaller class.

Figure 2. Partial removable laminar denture.
Useful for understanding the consequences of partial loss of teeth for the state of the entire dental system is the classification of K. Eichner (1962), which is based on the theory of the existence of protective zones in conditions of normal occlusion that ensure the maintenance of the height of the bite. There are four such zones. These zones are formed by premolars and molars.
Depending on the number of preserved protective zones, all dentition can be divided into three groups:
the first is the dentition, where there are antagonists in each of the four protective zones;
the second is the dental arch, where protective zones are partially absent;
the third is the dental arch, where there are no antagonists.
There are other classifications, each of which is designed to facilitate the study of the clinical picture of partial loss of teeth, simplify the filling out of documentation, and ensure communication between specialists.
However, drawing up a plan for future treatment is determined not only by the topography of the defect, but also by the condition of the crowns of the remaining teeth, the supporting apparatus of existing teeth, the type of bite of the patient, the characteristics of the edentulous area, and the age of the patient.
Clinic of the dental system against the background of partial loss of teeth
The clinical picture caused by partial loss of teeth is determined by the following factors:
time that has passed since the loss of teeth;
number of lost teeth;
topography of defects;
chewing load performed by the remaining teeth;
type of bite;
the condition of the remaining teeth and their periodontal tissues;
the age of the patient and the condition of his body.

Figure 3. Laboratory stage of production of SSPP.
Key symptoms of partial secondary adentia:
Violation of the integrity of the dentition.
Splitting of the dentition into separately working groups of teeth, the formation of three nodes: a functioning center; traumatic node; non-functioning atrophic area.
Excessive functional load on periodontal tissue of remaining teeth.
Deformation of the occlusal plane.
Pathology of chewing, aesthetic norms, speech, facial and masticatory muscles, condition of the temporomandibular joints.
Pathological transformations observed in the dentition are divided into the following conditions:
Compensated, characterized by a defect in the dentition, which does not affect the shape and structure of the latter, periodontal tissue.
Subcompensated - develops as a result of internal restructuring within the dentition: the teeth become inclined towards the area of the defect, trema are formed, antagonist teeth, not meeting the support opposite the defect, move vertically, a restructuring of the entire periodontium of the remaining teeth is observed.
A decompensated state is typical for situations when internal restructuring occurs against the background of inflammatory processes in periodontal tissues, destruction, accompanied by the formation of gingival pockets, and as the process progresses, bone pockets.

Figure 4. Clinical picture with partial loss of teeth.
Sub- and decompensated states are formed in conditions of reactive failure of the body; under the influence of chewing load, the dentoalveolar system begins to collapse, and a pathological condition occurs, accompanied by internal restructuring.
Laboratory studies have proven that the pathology of calcium metabolism due to tooth loss is generalized, there is no direct dependence on the number and topography of jaw defects, this condition is a harbinger of radiological and clinical disorders, and worsens as resorptive processes progress.
The ongoing bone restructuring resembles the phenomenon of osteoporosis (atrophy, which is characterized by the replacement of destroyed connective fibrous tissue).
Resorption of the alveolar process is an irreversible chronic process, constantly progressing, which aggravates the general condition.
The type of bone structure determines the rate of resorption. Based on X-ray data, the following types of bone tissue can be distinguished by structure:
dense, has a fine-mesh structure, dense cortical plate, thick trabeculae; such tissue is difficult to atrophy;
spongy, has a large-cell structure, poorly defined cortical plate;
without a cortical layer, has thin bone beams, needle-like trabeculae along the periphery of the alveolar process; such tissue easily and rapidly atrophies.
The intensity of the resorption process is most pronounced during the first six months after tooth loss; its expression within the alveolar ridge does not depend on time and is not limited to any volume.
Condition of the mucous membrane of the prosthetic bed
Assessment of the mucous membrane in the area of the edentulous alveolar process includes determining the following indicators:
thickness,
pain sensitivity,
degree of compliance.
These data are important when determining the boundaries of the prosthetic bed.
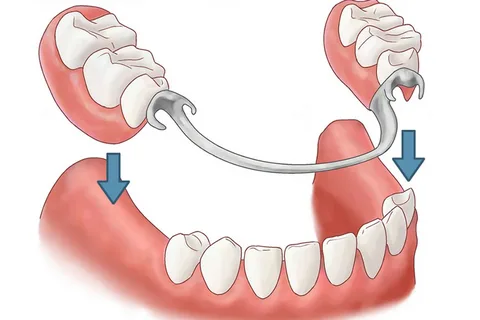
Figure 5. Prosthetics for partially edentulous patients.
Compliance classification:
small – up to 0.4 mm;
average – 0.4-0.9;
large – more than 0.9 mm.
Zones of the hard palate according to the degree of compliance:
The median fibrous zone corresponds to the sagittal suture; it is devoid of a submucosal layer, for this reason the degree of its compliance is minimal.
The peripheral fibrous zone corresponds to the alveolar process and has a submucosal layer of insignificant thickness.
The area of the transverse palatal folds is characterized by medium compliance.
The posterior third of the hard palate is lined with mucosa, which has a thick submucosal layer equipped with adipose tissue and mucous glands; the degree of compliance here is maximum.
The degree of compliance is directly proportional to the area of the vascular fields, their density increases as they approach line A. The ability of the vessels to quickly empty due to anastomoses with the nasal cavity, maxillary sinus, deep sections of bone tissue and again fill with blood creates conditions for reducing tissue volume.
This is where the concept of buffer zones comes from - these are areas of the mucous membrane of the hard palate where there are large vascular fields, which are characterized by spring or shock-absorbing qualities.
The condition of the mucous membrane in the area of the prosthetic bed must be taken into account in the process of planning an orthopedic design, since the base of the prosthesis must be placed on tissues characterized by the same level of compliance when pressure is applied to them. It is also important to consider that muscle activity and occlusal forces on the working side increase, and neuromuscular control increases. This is due to the proprioceptive characteristics of the periodontal ligament of the remaining teeth.
When diagnosing the disease and drawing up a treatment plan, it is necessary to take into account the following periodontal indicators of the remaining teeth:
volume of bone tissue;
presence of mobility;
presence and depth of pockets;
volume of attached gum;
the presence of inflammatory processes in surrounding tissues.
The prognosis of treatment for partial edentia is determined by the periodontal condition of the remaining teeth.
About the benefits of removable prosthetics at the webinar Introduction to removable prosthetics .