
Medication-related osteonecrosis of the maxilla, surgical treatment (clinical case)
Machine translation
Original article is written in RU language (link to read it) .
Disruption of the bone remodeling process under the influence of various factors, including local and systemic ones, including medications (anti-resorptive and anti-angiogenic), can lead to the development of osteonecrosis of the jaw bones. A clinical case of osteonecrosis of the maxilla associated with the use of bisphosphonates and its surgical treatment in an 81-year-old patient with complaints of pain in the left maxilla and a sharp ichorous smell from the mouth is described, who was hospitalized 6 months after the extraction of teeth 24, 25 due to complicated caries. Upon examination, a site of exposed bone tissue was observed in the area of the alveolar process of the left maxilla. Surgical intervention was performed, including sectoral resection while preserving continuity within healthy tissues, filling the bone tissue defect with a platelet-rich blood clot and compact osteotomy of healthy bone around the defect's periphery. Timely diagnosis of osteonecrosis of the jaw bones is crucial for improving treatment effectiveness. When diagnosing, it is important to consider that patients undergoing invasive dental procedures and receiving bisphosphonate therapy for osteoporosis are at risk for bisphosphonate-related osteonecrosis of the jaw. The proposed method of surgical treatment for MRONJ contributes to improved blood supply and provides effective separation of the bone cavity from the oral cavity in the area of the defect.
Relevance of the Problem
In recent decades, osteonecrosis of the jaw related to medication use, particularly bisphosphonates, has been widely discussed. Accumulating at the site of active bone formation, bisphosphonates disrupt the remodeling cycle, reducing the survival and function of osteoclasts. Triggers for the development of medication-related osteonecrosis of the jaw include invasive dental procedures, periodontal diseases, and trauma from dental prosthetics. Recent studies reveal the role of osteomalacia and low vitamin D levels as risk factors in the occurrence of MRONJ.
According to the American Society for Bone and Mineral Research, medication-related osteonecrosis of the jaw associated with bisphosphonate therapy is defined as the presence of exposed bone in the oral cavity that persists for 8 weeks in a patient who is currently receiving or has received bisphosphonates, with no history of radiation therapy to the jaw or face. The diagnostic criteria were updated in 2014 by the American Association of Oral and Maxillofacial Surgeons and are based on clinical features, radiological imaging in the presence of a pharmacological history or ongoing use of anti-resorptive agents, particularly bisphosphonates (BPs) or anti-angiogenic agents such as monoclonal antibodies targeting vascular endothelial growth factor (VEGF) receptors. A special committee of the American Association of Oral and Maxillofacial Surgeons (AAOMS) proposed to change the nomenclature from bisphosphonate-related osteonecrosis of the jaw (BRONJ) to medication-related osteonecrosis of the jaw (MRONJ) due to the increase in cases of osteonecrosis associated with other anti-resorptive and anti-angiogenic treatment methods. However, the nomenclature regarding this pathology has been and remains a subject of discussion.
Thus, according to the latest data, MRONJ is a severe and multifactorial clinical disease. Its development requires a combination of several accompanying factors. The main risk factors, in addition to osteomalacia, the use of anti-resorptive agents, and immunosuppression, include the concomitant use of such medications as steroids. Dental interventions, infections of the oral cavity and gums, and vitamin D deficiency exacerbate the course of the pathological process.
The aim of the study: to improve the effectiveness of the treatment of drug-induced osteonecrosis of the jaws.
Materials and Methods of the Study
The results of treatment were evaluated dynamically (upon admission, before surgery, after surgery, during stabilization, before discharge) based on clinical and laboratory data using the Apache II scale, adapted for maxillofacial surgery. The obtained data were compared with the patients' self-assessment of the internal clinical picture of the disease at the same stages of treatment. For this purpose, we developed special questionnaires that included the severity of anxiety (2-4 points) in the patient's self-assessment of the internal picture of the disease: pain in the area of the lesion; swelling of the gums in the area of the lesion; swelling, cheek infiltrate; limitation of mouth opening; bad breath; discharge of pus and bleeding in the mouth; tongue injury from friction with exposed bone; discharge of pus and bleeding from external fistulous tracts; increased pain when opening the mouth; general weakness. The patient had to indicate how much each of the listed manifestations of the disease bothered him. The level of anxiety (1-4 points) was also taken into account. The total score for each clinical case was determined as follows: Ex — total self-assessment of the disease picture by the patient at the stages of treatment [before and one month after surgery (in percentage)]; E1 - number of points before treatment; E2 — number of points after treatment; Ex%=100 - (E2x100:E1).
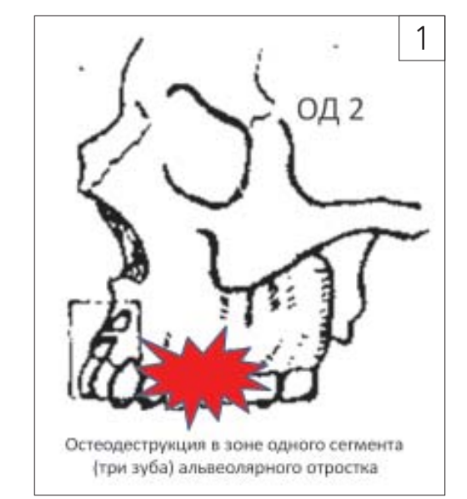
We have developed a classification of the prevalence of pathological osteodestructive processes in the upper and lower jaws, stages of drug-induced osteonecrosis, and the interdependence of surgical treatment methods. The variant of osteodestruction of one of the segments of the alveolar process of the upper jaw OD 2 is depicted in the diagram (Fig. 1). The method of surgical treatment is presented in the clinical observation outlined below.
Clinical case. Patient E., 81 years old, was hospitalized in the Center for Maxillofacial and Plastic Surgery with complaints of pain in the upper jaw on the right side and a sharp ichorous smell from the mouth. From the history, it is known that the patient underwent bisphosphonate therapy (oral form “Bonviva” 150 mg once a month for 3 years) for osteoporosis. Six months ago, the patient had teeth 24 and 25 removed in the clinic due to complicated caries. Upon examination, an area of exposed bone tissue measuring 1.5×2.0 cm, gray in color, under a fibrinous membrane is identified in the area of the alveolar process of the upper jaw on the left. The surrounding gingival mucosa is hyperemic, swollen, and sharply painful upon palpation.

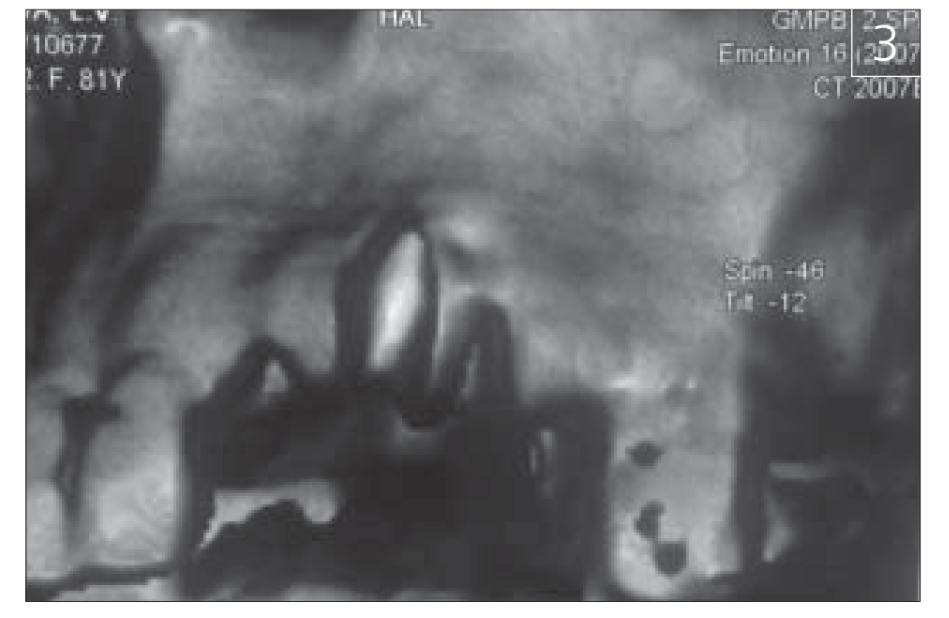
According to the 3D CT: in the projection of the extracted teeth 24, 25, a focus of bone tissue destruction is identified without clear boundaries, localized in the area of the alveolar process on the left (Fig. 3). No distinct disruption of the integrity of the bone floor of the maxillary sinus was identified. No shadows in the sinus were present (Fig. 3).
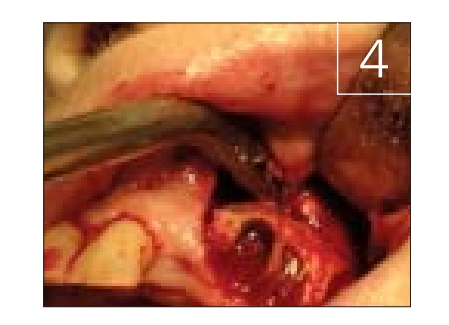
Operation: under combined anesthesia, an incision was made in the mucosa of the alveolar process on the left, with the excision and detachment of a trapezoidal mucoperiosteal flap from the vestibular side to visualize the area of exposed bone tissue, in the projection of the sockets of teeth 24, 25. The zone of destruction in the area of the alveolar process of the upper jaw on the left was skeletonized (Fig. 4).
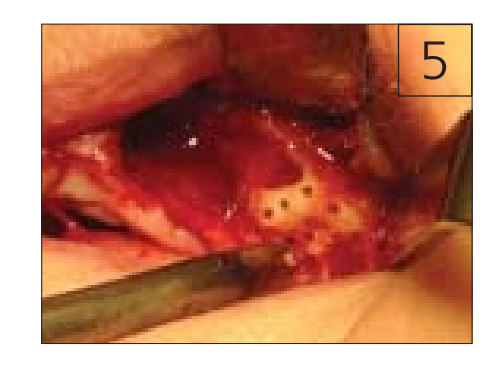
A BLOCK resection was performed within healthy tissues in the area of the alveolar process of the upper jaw on the left, measuring 1.5×1.5, down to visibly healthy bleeding bone. Hemostasis was achieved. After the BLOCK resection, a bone cavity with smooth walls is observed, and good blood supply is visually noted. There is focal resorption of the floor of the maxillary sinus without signs of perforation and communication of the wound with the maxillary sinus. The bone cavity is filled with a platelet-rich blood clot, and a compactostectomy was performed around the periphery of the bone cavity (Fig. 5).
The mucosal-periosteal flap is mobilized by incising the periosteum and creating additional incisions, which allows for the wound to be closed completely, preventing its communication with the oral cavity (Fig. 6), sutures are applied (vicryl).

In the postoperative period, the patient received comprehensive therapy aimed at improving microcirculation and antibacterial treatment (pentoxifylline, amoxiclav, vitamin E). Healing of the surgical wound by primary tension.
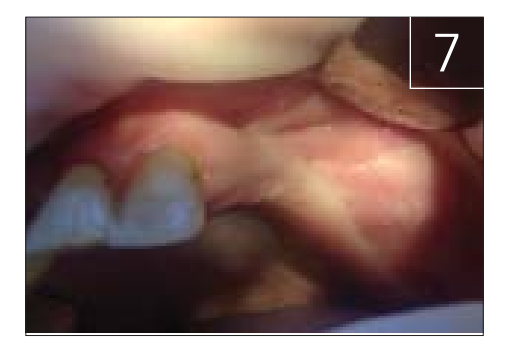
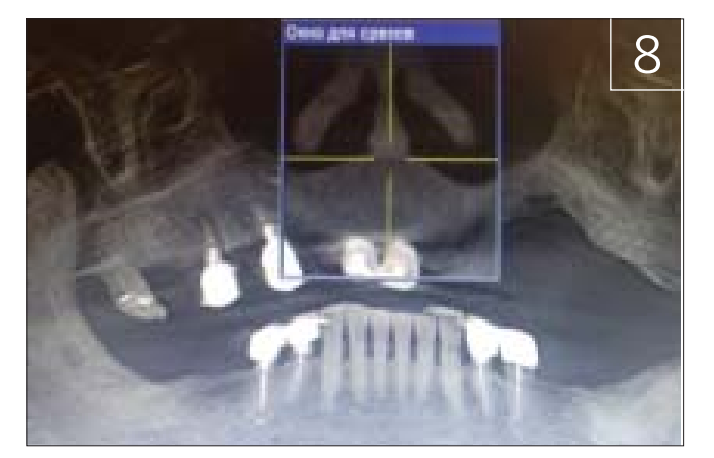
At the follow-up examination after 2 years — epithelialization and partial restoration of bone tissue in the area of the destruction focus (Fig. 7, 8).
Study Results and Discussion
Patients who have been taking bisphosphonates for a long time represent a risk group for MRONJ, especially if they undergo invasive dental treatment. In our case, the patient had been using the tablet form of the drug "Bonviva" (active ingredient - ibandronic acid) for five years to treat osteoporosis. MRONJ was triggered by the extraction of teeth 24 and 25 due to complicated caries.
Surgical treatment was performed using the method we developed for the surgical treatment of MRONJ, which includes: incision of the mucosa of the alveolar ridge in the area of the defect, resection of the alveolar ridge within healthy tissues, and the formation of a trapezoidal mucoperiosteal flap in the area of the defect to close the wound. The resection of the alveolar ridge was performed as a single bone block within one segment while maintaining the continuity of the jawbone structure. The bone cavity was filled with a platelet-rich autologous blood clot, and a compactostectomy was performed around the periphery of the bone cavity. To completely separate the bone cavity from the oral cavity, the periosteum at the base of the formed flap was incised, and two incisions were made in the shape of a hook to increase its length and allow free movement into the surgical field, and the defect was closed.
When performing resection with a single bone block within one segment while maintaining the continuity of the jawbone structure, the risks of damaging blood vessels and nerves are minimized due to their good visualization during resection. Resection with a single bone block allows for the creation of a bone bed that retains a platelet-rich autologous blood clot, which is fixed by a connective tissue framework formed during the movement of the mucoperiosteal flap, contributing to reliable and complete separation of the bone defect from the oral cavity. Filling the bone cavity with a platelet-rich blood clot promotes the acceleration of reparative processes in the area of the bone tissue defect, while the effectiveness of treatment is enhanced due to the formed bone bed with smooth edges and minimal damage to blood vessels and nerves.
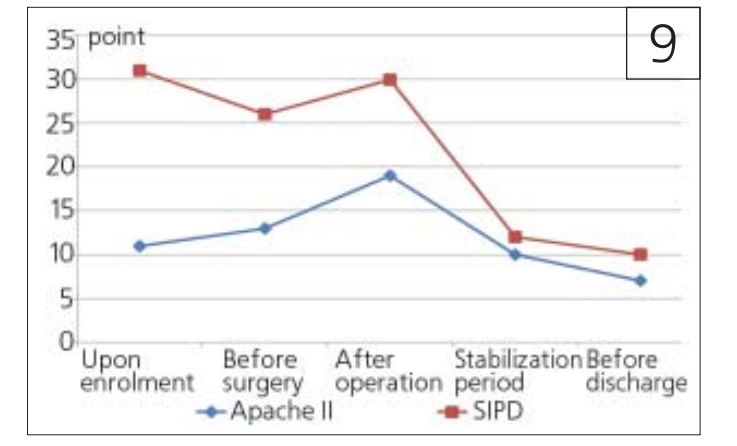
The comparison of clinical-laboratory data according to the Apache II scale with the patient's self-assessment of the internal clinical picture of the disease (SVKZ) revealed a unidirectional trend towards improvement (Fig. 9). In percentage terms, the improvement in condition one month after the operation is 79.2%.
Conclusions
Before starting bisphosphonate treatment, the patient must undergo complete oral sanitation to further exclude invasive dental procedures.
Timely diagnosis of osteonecrosis of the jaw bones is crucial for improving treatment effectiveness. When making a diagnosis, it is important to consider that patients who have undergone invasive dental procedures and are receiving bisphosphonate therapy for osteoporosis are at risk for bisphosphonate-related osteonecrosis of the jaw.
Performing a one-block resection within a single segment while maintaining the continuity of the jawbone structure, filling the bone tissue defect with a platelet-rich blood clot, compact osteotomy of healthy bone within the surgical wound, and closing the defect area with a mucoperiosteal flap along the transitional fold allows for good results by improving blood supply to the affected area.
A.I.Yaremenko, G.A.Khatkevich, T.L.Onokhova, I.G.Trofimov, E.V.Tumanov
List of References
Kharitonov Yu.M., Kikov R.N. Evaluation of homeostasis in patients with progressive facial and neck phlegmons in adverse disease course // Applied information aspects of medicine. - 2020. - No. 23 (4). - Pp. 40-50. [Харитонов Ю.М., Киков Р.Н. Оценка состояния гомеостаза у пациентов с прогрессирующими флегмонами лица и шеи при неблагоприятном течении заболевания. Прикладные информационные аспекты медицины. 2020; 23(4): 40-50. (На русском).] Link is active on19.10.2021. https://www.elibrary.ru/download/elibrary_45332931_67341439.pdf
Dalle Carbonare L., Mottes M., Valenti M.T. Medication-Related Osteonecrosis of the Jaw (MRONJ): Are Antiresorptive Drugs the Main Culprits or Only Accomplices? The Triggering Role of Vitamin D Deficiency. Nutrients. 2021;13(2):561. https://doi.org/10.3390/nu13020561
Demircan S., Isler S. Changes in serological bone turnover markers in bisphosphonate induced osteonecrosis of the jaws: A case control study. Niger. J. Clin. Pract. 2020;23(2):154-158. https://doi.org/10.4103/njcp.njcp_374_19
Heim N., Warwas F.B., Wilms C.T., Reich R.H., Martini M. Vitamin D (25-OHD) deficiency may increase the prevalence of medication-related osteonecrosis of the jaw. J. Cranio-Maxillofac. Surg. 2017;45(12):2068-2074. https://doi.org/10.1016/j.jcms.2017.09.015
Kizub D.A., Miao J., Schubert M.M., Paterson A.H.G., Clemons M., Dees E.C., Ingle J.N., Falkson C.I., Barlow W.E., Hortobagyi G.N., et al. Risk factors for bisphosphonate-associated osteonecrosis of the jaw in the prospective randomized trial of adjuvant bisphosphonates for early-stage breast cancer (SWOG 0307) Support Care Cancer. 2021;29(5):2509-2517. https://doi.org/10.1007/s00520-020-05748-8
Khosla S., Burr D., Cauley J., Dempster D.W., Ebeling P.R., Felsenberg D., Gagel R.F., Gilsanz V., Guise T., Koka S., McCauley L.K., McGowan J., McKee M.D., Mohla S., Pendrys D.G., Raisz L.G., Ruggiero S.L., Shafer D.M.,
Shum L., Silverman S.L., Van Poznak C.H., Watts N., Woo S.B., Shane E. American Society for Bone and Mineral Research. Bisphosphonate-associated osteonecrosis of the jaw: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2007;22(10):1479-91. https://doi.org/10.1359/jbmr.0707onj
Kim J., Lee D.-H., Dziak R., Ciancio S. Bisphosphonate-related osteonecrosis of the jaw: Current clinical significance and treatment strategy review. Am. J. Dent. 2020;33:115-128.
Kuroshima S., Sasaki M., Sawase T. Medication-related osteonecrosis of the jaw: A literature review. J Oral Biosci. 2019;61(2):99-104. https://doi.org/10.1016/j.job.2019.03.005
Mücke T., Krestan C.R., Mitchell D.A., Kirschke J.S., Wutzl A. Bisphosphonate and Medication-Related Osteonecrosis of the Jaw: A Review. Semin Musculoskelet Radiol. 2016;20(3):305-314. https://doi. org/10.1055/s-0036-1592367
Otto S., Marx R.E., Tröltzsch M., Ristow O., Ziebart T., Al-Nawas B., Groetz K.A., Ehrenfeld M., Mercadante V., Porter S., Bedogni A., Campisi G., Fusco V., Dayisoylu E., Fliefel R., Herlofson B.B., Pautke C., Kwon T-G., Fedele S. Comments on “diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus” J. Bone Miner. Res. 2015;30(6):1113-1115. https://doi.org/10.1002/jbmr.2525
Ruggiero S.L., Dodson T.B., Fantasia J., Goodday R., Aghaloo T., Mehrotra B., O’Ryan F. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw-2014 update. J. Oral Maxillofac. Surg. 2014;72(10):1938-1956. https://doi.org/10.1016/j.joms.2014.04.031
Schiodt M., Otto S., Fedele S., Bedogni A., Nicolatou-Galitis O., Guggenberger R., Herlofson B.B., Ristow O., Kofod T. Workshop of European task force on medication-related osteonecrosis of the jaw-Current challenges. Oral Dis. 2019;25(7)10:1815-1821. https://doi.org/10.1111/odi.13160
Yarom N., Peterson D.E., Bohlke K., Saunders D.P. Reply to Fusco et al. Comment on Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline Summary. January 24, 2020. JCO Oncol. Pract. 2020;16(3):145-146. https://doi.org/10.1200/JOP.19.00716