
Pathology of Bone Tissue in the Clinical Practice of Dentists and Maxillofacial Surgeons
Machine translation
Original article is written in RU language (link to read it) .
The article presents the results of clinical observations of bone tissue pathology of the skull bones, which may be encountered in the practice of maxillofacial surgeons, dentists, and radiologists.
Introduction
The methodology for examining a patient in the clinic of dentistry and maxillofacial surgery (MFS) includes not only the collection of information regarding gender, age, complaints, and duration of the disease but also the assessment of the localization of the pathological process and the number of bones involved in the pathological process. In addition to a wide range of radiological studies, additional methods such as cone-beam computed tomography (CBCT), multi-slice computed tomography (MSCT), and/or magnetic resonance imaging (MRI) are used. If necessary, radionuclide technologies are employed, represented by positron emission computed tomography (PET-CT), single-photon emission computed tomography (SPECT-CT), and bone scintigraphy. Failure to adhere to the algorithm and thoroughness of the examination in some cases may lead to irreversible consequences.
Radiographic semiotics of bone and joint diseases includes changes in the position, shape, and size of bones, their contours and structure, as well as destructive and osteosclerotic processes.
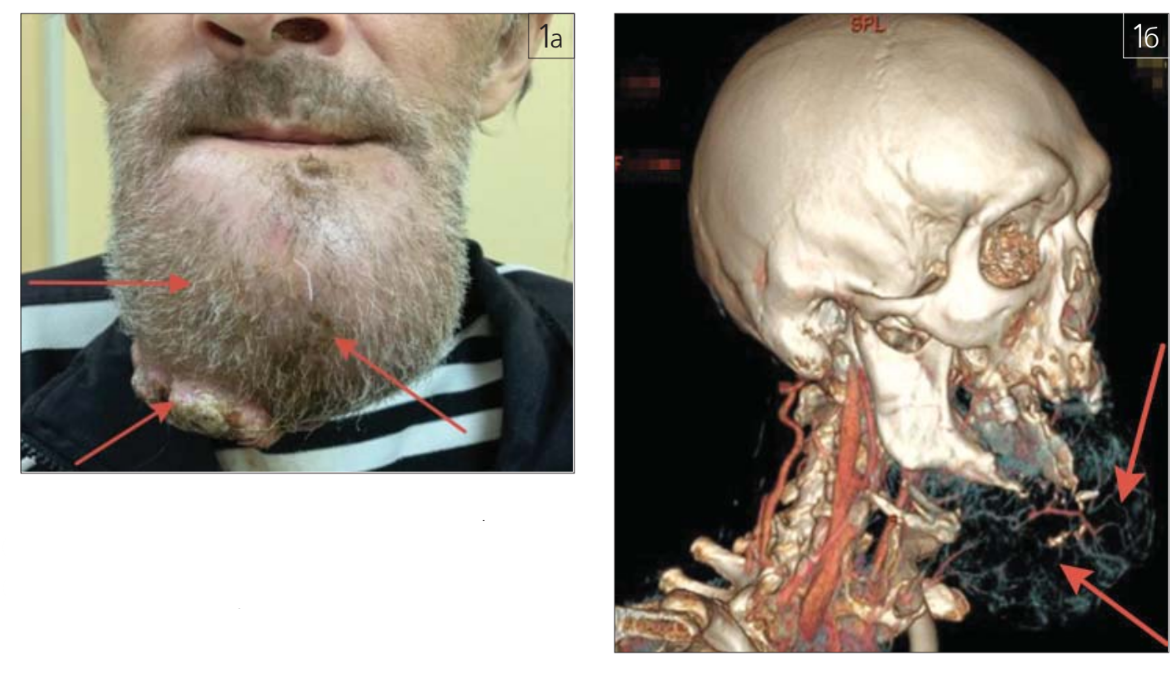
Changes in the shape and size of bones may be characterized by volume disturbances (hyperostosis, "bulging", atrophy), pathological tissue growth (Fig. 1 a-g), curvature, elongation or shortening of bones, and changes in the articulating surfaces in the joint.
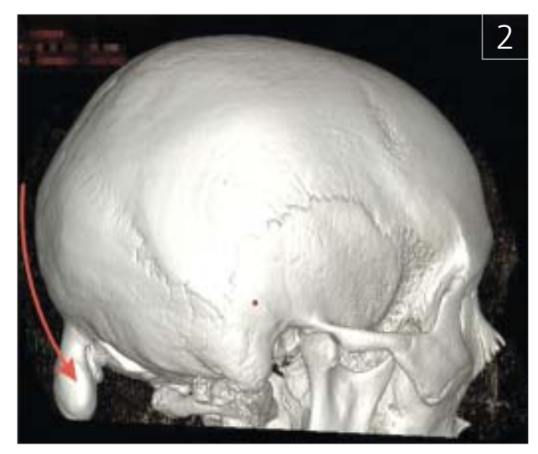
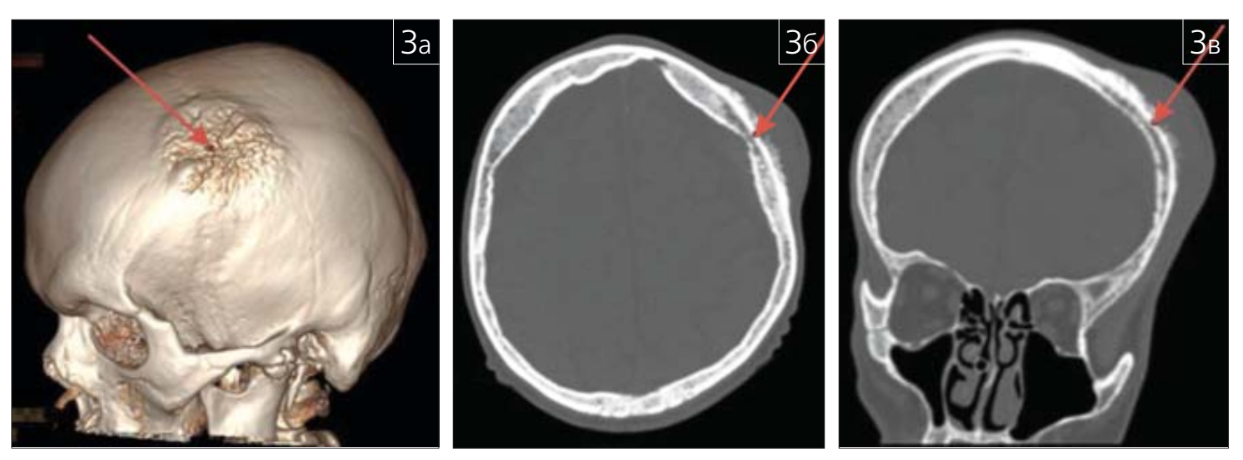
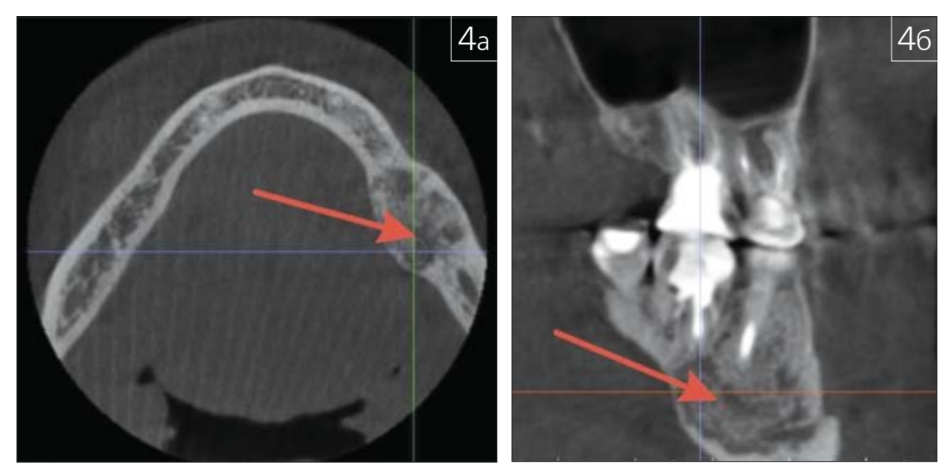
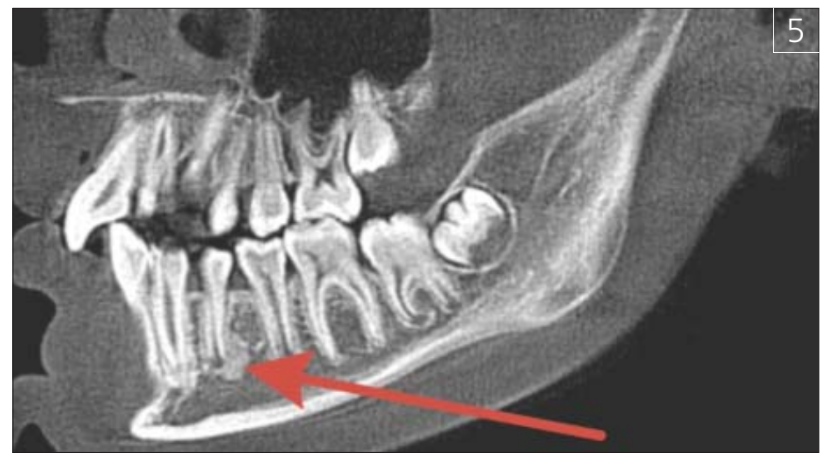
A pathological neoplasm may be a symptom of a primary or secondary bone tissue tumor (fig. 2; 3 a-b), fibrous dysplasia (fig. 4 a-b; 5), which may be hereditary, and the main radiological criterion for assessment is the preservation of the closure plate, indicating the benign nature of the pathological process.
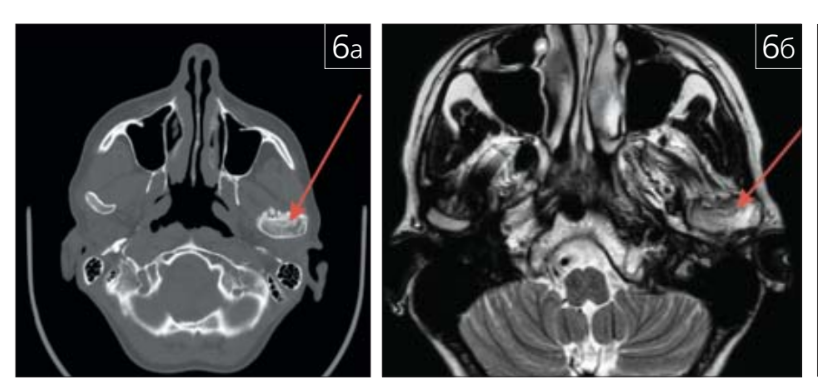
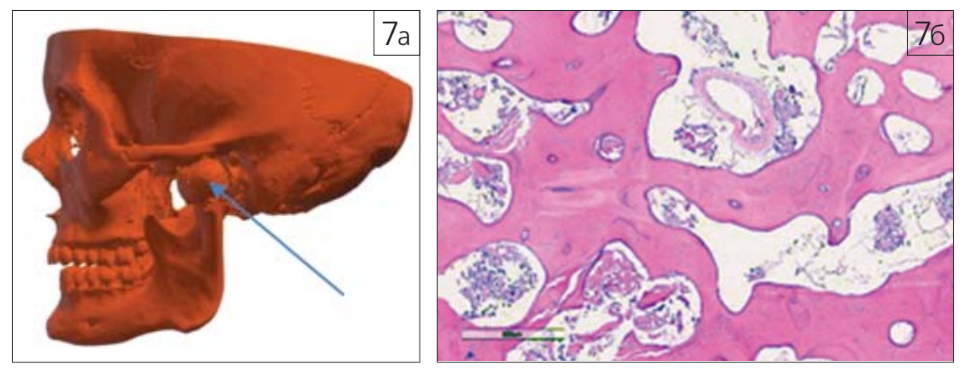
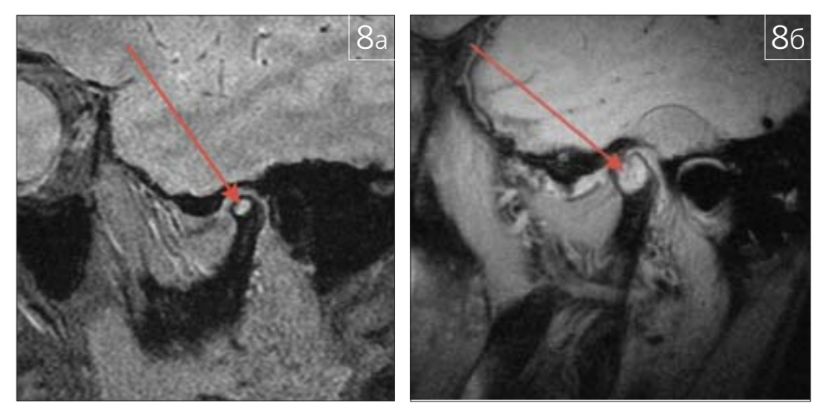
Using radiological diagnostic methods, pathological changes in the articulating surfaces of the temporomandibular joint (TMJ) can be identified. Examples of bone tissue pathology of the TMJ are shown in Fig. 6 a, b; 7 a, b; 8 a, b.
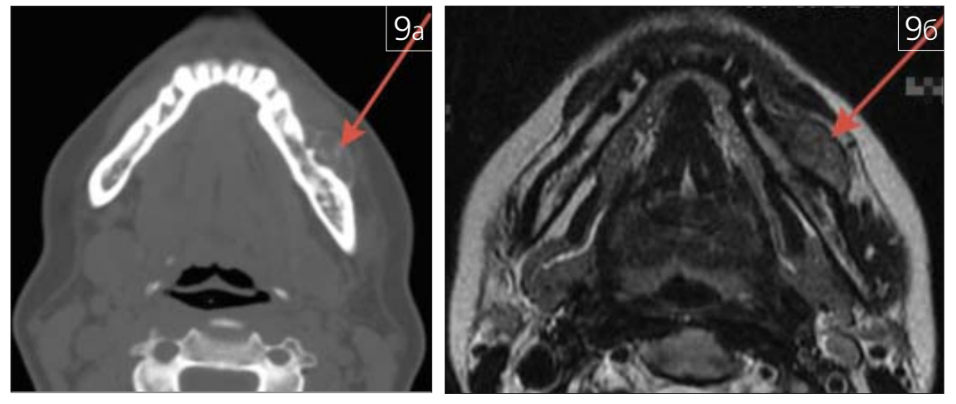
Bone tissue pathology can be characterized not only by changes in its structure but also by changes in the adjacent soft tissues (Fig. 9 a-c).
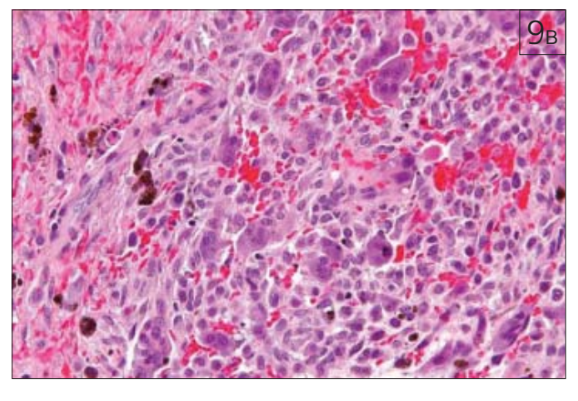
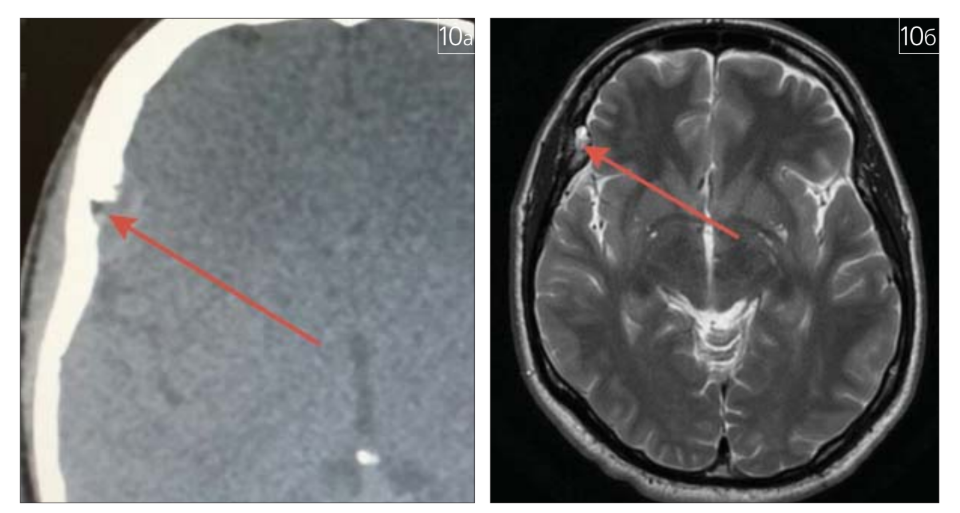
In the practice of a radiologist, a condition such as eosinophilic granuloma (Taratynov's disease) is regularly encountered. Its radiological signs include areas of bone tissue rarefaction with indistinct "fringed" contours without a sclerotic rim, possible destruction of the outer and inner cortical plates of bone tissue, and invasion into soft tissues, with the formation of sequestra (the "button" sign on the X-ray, Fig. 10). It is worth noting that these changes can be detected on X-ray images used for cephalometric analysis in the practice of an orthodontist and maxillofacial surgeon. This refers to lateral and frontal cephalometric radiographs (CR) of the skull and 3D cephalometry. Myeloma (multiple myeloma, generalized plasmacytoma, Rustitsky-Kalera disease) is a malignant tumor of plasma cells (differentiated B-lymphocytes that produce antibodies). This blood system disease, classified as paraproteinemic leukemias, is radiologically characterized by well-defined "stamped" foci of destruction of varying sizes in the bones of the skull vault, clavicles, ribs, and pelvic bones (Fig. 11).
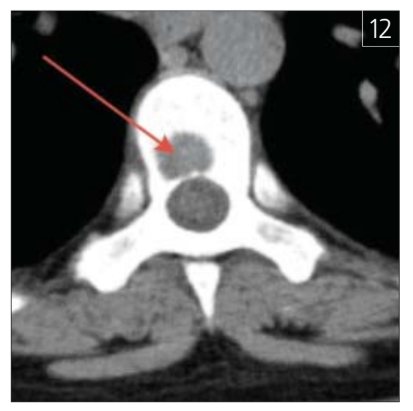
A sad finding in the practice of a dentist and maxillofacial surgeon can be osteolytic metastases in the skeleton's bones, including the vertebrae (Fig. 12).
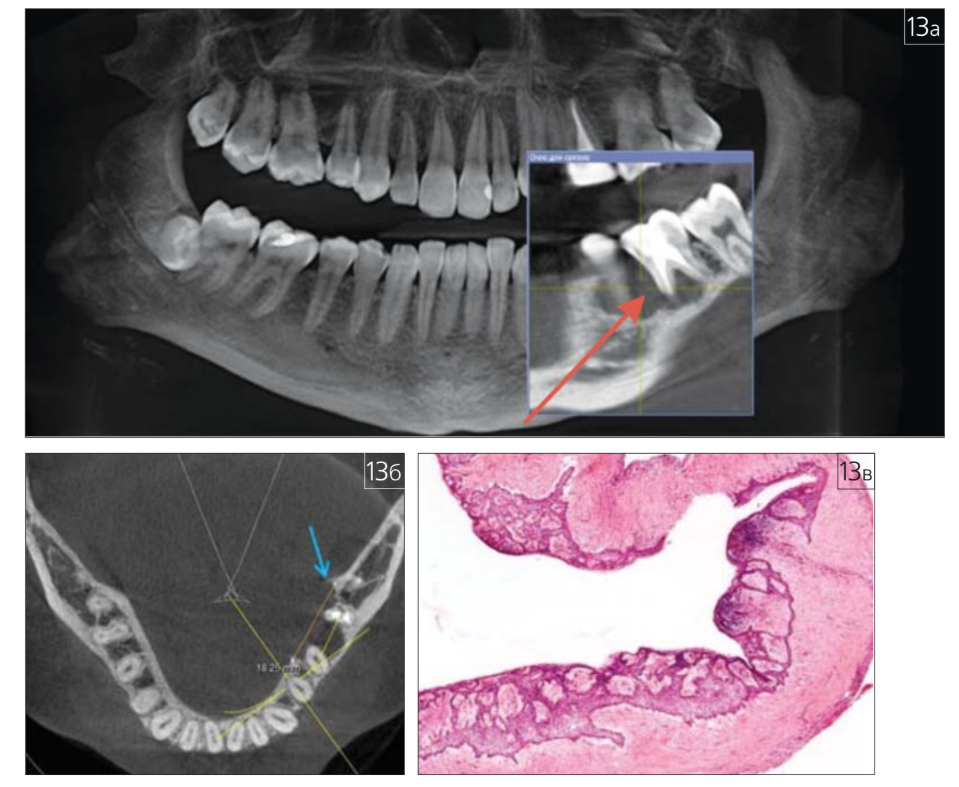
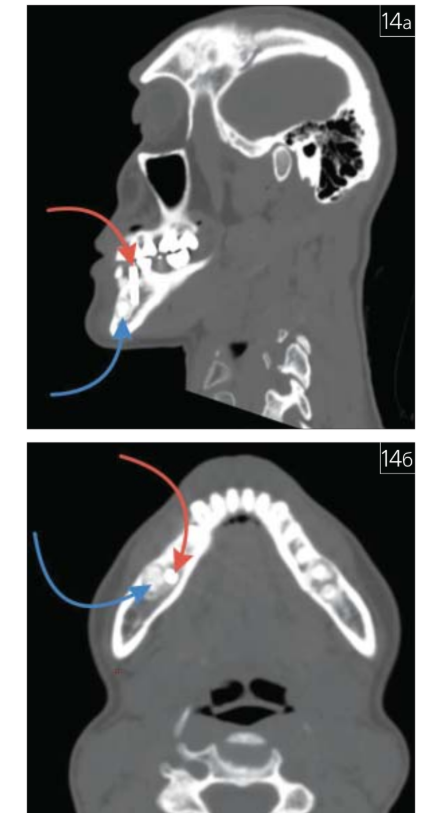
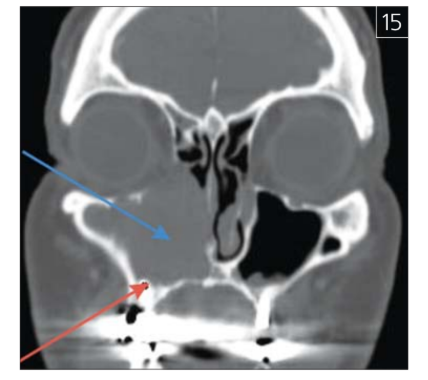
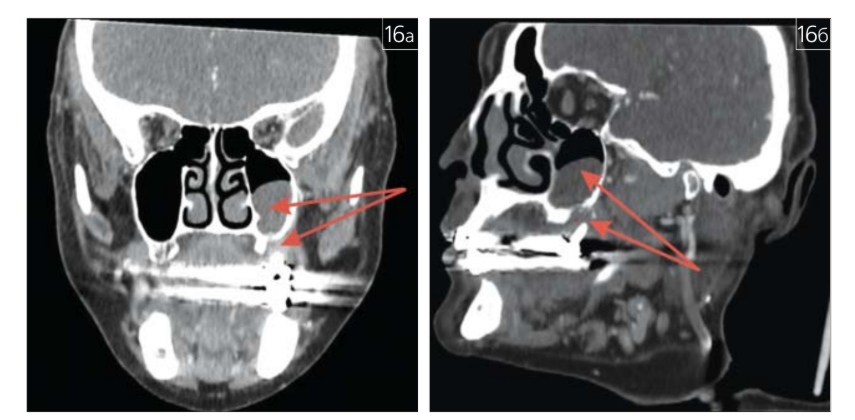
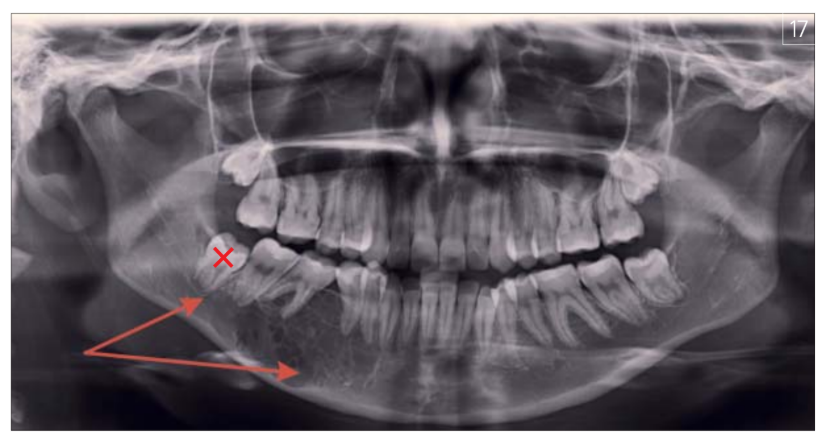
Iatrogenesis occupies a special place in the practice of a dentist, maxillofacial surgeon, and radiologist (Fig. 13 a-c; 14 a, b; 15 a-c; 16; 17).
Thus, based on a number of clinical examples provided by us, the diversity of pathological changes in the bone tissue of the jaws and other bones of the skull encountered in the routine practice of a dentist and maxillofacial surgeon is clearly illustrated. The interaction of the clinician with the radiologist and pathologist plays a crucial role in the timely detection and correct interpretation of these changes.
In order to prevent iatrogenesis, the authors' collective considers it possible to propose the following practical recommendations:
Compliance with the Order of the Ministry of Health of the Russian Federation dated 09.06.2020 No. 560n regarding the description of the X-ray image of the jaws (skull bones) by the radiologist.
Radiological control at all stages of dental treatment.
Use of additional examination methods (MSCT and MRI, PET-CT, SPECT-CT, osteoscintigraphy, densitometry, laboratory re-examination, etc.).
Performing tissue biopsy (if indicated).
Exclusion of teeth located near the pathological area from the action zone of orthodontic appliances.
Control of the presence in the outpatient card (medical history) of informed voluntary consent for examination and treatment.
Assessment of the psycho-sensory and anatomical-functional disadaptation of the patient at the stages of treatment and involving (if necessary) a clinical psychologist in the work.
N.V. Vishneva, A.N. Lanina, O.V. Lukina, E.V. Bubnova, A.G. Tyurin, R.A. Fadeev, A.I. Yaremenko
References
Kitaev, V.M. Radiological Diagnosis of Bone Tissue Pathology / V.M. Kitaev, S.V. Kitaev, O.Yu. Bronov. - Moscow: MEDpress-inform, 2022. - 184 p. : ill.
Psycho-sensory-anatomical-functional disadaptation syndrome (PSAF disadaptation syndrome) in dentistry and related disciplines / M.M. Soloviev, A.I. Yaremenko, A.M. Solovieva et al. // Collection of abstracts “Fundamental and Applied Problems of Dentistry” (Saint Petersburg, December 11-13, 2014). - Saint Petersburg, 2014. - P. 143-144.
Brody A., Zalatnai A., K. Csomo, Belik A., Dobo-Nagy C. Difficulties in the diagnosis of periapical translucencies and in the classification of cemento-osseous dysplasia // BMC Oral Health. - 2019. - 19:139 p. 1-8. DOI 10.1186/s12903-019-0843-0.
Daviet-Noual V., Ejeil A.-L., Gossiome C., Moreau N., Salmo B. Differentiating early stage florid osseous dysplasia from periapical endodontic lesions: a radiological-based diagnostic algorithm // BMC Oral Health. - 2017. - 17:161, p 1-8. DOI 10.1186/s12903-017-0455-5.
Esfahanizadeh N., Yousefi H. Successful Implant Placement in a Case of Florid Cemento-Osseous Dysplasia: A Case Report and Literature Review // J Oral Implantol. - 2018. - Aug;44(4):275-279. DOI 10.1563/aaid-joi-D-17-00140.
Grün P., Schneider B., Bandura P., Pfaffeneder-Mantai F., Bytyqi D., Turhani D. Bone remodelling after minimally invasive surgical management of a recurrent florid cemento-osseous dysplasia in a Caucasian woman - 18 years follow-up of a unique case - a case report // International Journal of Surgery Case Reports. - 2023. - 108074. - p. 1-8.
Haefliger S., Baumhoer D. The new WHO classification of jaw tumors, The Pathology. - 2023. - 4. - 44. - p. 240-249. DOI 10.1007/s00292-023-01195-4.
Hameed M., Horvai A.E., Jordan R.C.K. Soft Tissue Special Issue: Gnathic Fibro Osseous Lesions and Osteosarcoma // Head and Neck Pathology. - 2020. - 14: p. 70-82. DOI 10.1007/s12105-019-01094-2.
Nelson B.L., Phillips B.J. Benign Fibro-Osseous Lesions of the Head and Neck // Head and Neck Pathology. - 2019. - 13. - p. 466-475. DOI 10.1007/s12105-018-0992-5.
Nilius M., Nilius M.H., Müller C., Lauer G., Berit K., Marcus K. Multifocal periapical cemental dysplasia in periodontal Ehlers-Danlos syndrome combined with leukoencephalopathy in the mutation of c.890G >a, G297D [pEDS] // Clin Case Rep. - 2022. - 10:e06490. - p. 1-6. DOI 10.1002/ccr3.6490.
Soluk-Tekkesin M., Wright J.M. The World Health Organization Classification of Odontogenic Lesions: A Summary of the Changes of the 2022 (5th) Edition // Turk Patoloji Derg. - 2022.-Vol. 38. - p. 168-184. DOI: 10.5146/tjpath.2022.01573.
Shadid R., Kujan O. Success of dental implant osseointegration in a florid cemento-osseous dysplasia: A case report with 8-year follow-up // Clin Pract. - 2020. - 4;10(3):1281. DOI 10.4081/cp.2020.1281.
Vered M., Wright J.M. Update from the 5th Edition of the World Health Organization Classification of Head and Neck Tumors: Odontogenic and Maxillofacial Bone Tumours // Head and Neck Pathology. - 2022. - 16:63-75. DOI 10.1007/s12105-021-01404-7.