
Dystrophic Calcification of Parotid Salivary Glands in Sjögren's Disease
Machine translation
Original article is written in RU language (link to read it) .
The article discusses a rare clinical case of differential diagnosis between calcinosis and sialolithiasis, which developed against the background of autoimmune pathology. The diagnosis of these pathologies poses difficulties for practicing physicians, and the treatment methods have fundamental differences. In this regard, the description of the present case is relevant and important. An algorithm for the application of basic and additional research methods to confirm the diagnosis is presented.
Calcinosis is a pathological condition characterized by the deposition of calcium salts in soft tissues or organs. Several types of calcinosis are distinguished based on the mechanism of its formation: metastatic, metabolic, and dystrophic. Additionally, calcification can be either local or systemic, which makes the differential diagnosis of this pathology challenging for practicing physicians.
The main erroneous diagnosis among maxillofacial surgeons is sialolithiasis. The development of sialolithiasis is indeed one of the most common pathologies of the salivary glands. The incidence is estimated to be between 1 in 10,000 to 1 in 30,000 people. Approximately 85% of salivary stones form in the submandibular gland, while 15% occur in the parotid gland. However, the formation of calcifications is possible in vascular developmental anomalies (phleboliths), malignant tumors, lymph nodes, scar tissues, and tonsils. Most often, patients may complain of swelling or enlargement in the parotid-masticatory, submandibular, and buccal areas, but a "chance finding" may also occur during radiological examination. Dystrophic calcification is associated with the formation of calcifications only locally, and the main causes can be chronic inflammatory processes or traumatic factors.
The purpose of the study is to determine the algorithm for the differential diagnosis of patients with sialolithiasis and calcinosis.
Clinical case
Patient P., 34 years old, presented to the oncology department No. 8 (maxillofacial surgery) of the St. Petersburg State Medical University named after acad. I.P. Pavlov with complaints of periodic swelling of the preauricular areas on both sides.
According to the patient, for 8 months she had noticed swelling of the preauricular areas on the right and left. There were three episodes of "swelling" in the specified areas. She independently conducted conservative therapy in the form of taking non-steroidal anti-inflammatory drugs and applying cold compresses. Due to the increasing frequency of symptoms, she sought outpatient dental assistance. Diagnostic measures were carried out to exclude viral sialadenitis, as well as a consultation with an otorhinolaryngologist. Upon performing multi-slice computed tomography of the head and neck without contrast agent, multiple hyperdense, well-defined foci measuring 1-3 mm were found in the parotid salivary glands on both sides (Fig. 1). Based on the obtained data, the patient was referred for a consultation with a maxillofacial surgeon with a preliminary diagnosis of sialolithiasis. During the history taking, she noted a gradual onset of dry mouth and moderate swelling of the upper eyelids.

Medical history: non-smoker. No somatic pathology detected. No pathological changes in the chest organs were found during fluorographic examination.
The patient consented to the diagnostic procedures, processing, storage, and publication of the obtained data in an anonymized format.
During the examination, moderate enlargement of the parotid salivary glands was visualized on both sides. The skin was of normal color, without pathological rashes. Mouth opening and swallowing were free and painless. Regional lymph nodes were not palpated. Both parotid glands were of a firm-elastic consistency, movable, and painless on palpation; a small amount of clear saliva was released during massage. The mucous membrane of the mouth was pink, without pathological rashes, smooth, and matte.
After collecting the history and conducting the main examinations, a decision was made to carry out additional diagnostic procedures.
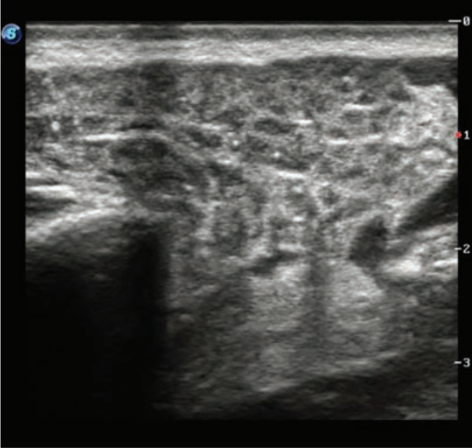
Ultrasound examination revealed diffuse changes in the structure of the parotid salivary glands on both sides, decreased echogenicity, and increased size. The presence of multiple calcifications in the structure of the glands on both sides was noted (Fig. 2).
Laboratory examination revealed increased levels of rheumatoid factor and antinuclear factor 1:5120 (nuclear granular type of fluorescence). Hypercalcemia was not detected. In the biopsy of the minor salivary glands, focal lymphocytic infiltration of the follicular type was observed. Based on the obtained data, the patient was recommended to consult a rheumatologist for further examination and diagnosis. After that, the diagnosis of Sjögren's disease was confirmed.
Results and Discussion
Sjögren's syndrome is an autoimmune systemic connective tissue disorder characterized by the involvement of exocrine glands. The mechanism of development of this disease is the destruction of the epithelium of the salivary glands due to abnormal reactions of B- and T-cells. Dystrophic calcification is the most common variant of calcinosis, which is associated with a large number of diseases, including some autoimmune pathologies such as scleroderma, dermatomyositis, and lupus erythematosus. Cases of calcification in Sjögren's syndrome are quite rare, most often describing the formation of calcifications in soft tissues, the brain, and the kidneys.
The formation of concretions is also a debatable issue. However, the treatment of this condition boils down to their removal or complete extirpation of the salivary gland. In the case of calcinosis, the strategy is aimed at treating the underlying disease and is conservative in nature. Therefore, differential diagnosis is of great importance for choosing the correct strategy for further treatment.
Currently, the patient is under dynamic observation by a maxillofacial surgeon and is also receiving treatment for the underlying disease from a rheumatologist. There has been no pain syndrome or swelling of the parotid salivary glands since the treatment began.
Conclusion
The presented clinical case demonstrates the importance of correlating the radiological picture and clinical symptoms in the patient, the necessity of an interdisciplinary approach to the treatment of salivary gland diseases, as well as raising awareness among doctors about the diagnostic search algorithm for such patients.
A.Ya. Razumova, A.I. Yaremenko, S.I. Kutukova, N.L. Petrov
References
Kumar GA, Deora SS. Dystrophic Calcification in the Oral Cavity Resulting in Mechanical Dysphagia: A Case Report and Review of Calcification in the Head and Neck Region. Cureus. 2020;12(3):7469. https://doi.org/10.7759/cureus.7469
Junior VM, Netto R, Janini ME, Azevedo AB, de Andrade VM. Dystrophic calcification vs sialolithiasis in a pediatric parotid gland: A case report. J Clin Exper Dentistry. 2019;11(5):496-499.https://doi.org/10.4317/jced.55621
Huoh KC, Eisele DW. Etiologic factors in sialolithiasis. Otolaryngology — Head Neck Surg. 2014;145(6):935-939.https://doi.org/10.1177/0194599811415489
Thimsen V, Fauck V, Wiesmüller M, Agaimy A, Schapher M. Calcification in Salivary Gland Cancer Mimicking Sialolithiasis-A Diagnostic Pitfall on Imaging: Report of Two Cases and Brief Review of the Literature. J Clin Med. 2022;11(12):3329.https://doi.org/10.3390/jcm11123329
Groppo ER, Glastonbury CM, Orloff LA, Kraus PE et al Vascular malformation masquerading as sialolithiasis and parotid obstruction: a case report and review of the literature. Laryngoscope. 2010;120 (l4):130. https://doi.org/10.1002/lary.21594
Annapoorani AS, Thambi JR, Christy W. A retrospective diagnostic study of prevalence of orofacial calcifications using panoramic radiograph: To insinuate the unseen. J Clin Exper Dentistry. 2023;15(4):289-297. https://doi.org/10.4317/jced.60224
Yalcin ED, Ararat E. Prevalence of soft tissue calcifications in the head and neck region: A conebeam computed tomography study. Nigerian J Clin Pract. 2020;23(6):759-763. https://doi.org/10.4103/njcp.njcp_269_19
Chander S, Gordon P. Soft tissue and subcutaneous calcification in connective tissue diseases. Curr Opin Rheumatol. 2012; 24(2):158-164. https://doi.org/10.1097/BOR.0b013e32834ff5cd.
Brito-Zeron P, Baldini C, Bootsma H, Bowman SJ et al. Sjögren syndrome. Nature Rev Dis Primers. 2016;2:16047. https://doi.org/10.1038/nrdp.2016.47
Llamas-Velasco M, Eguren C, Santiago D, Garcia-Garcia C et al. Calcinosis cutis and Sjögren’s syndrome. Lupus. 2010;19(6):762-764. https://doi.org/10.1177/0961203309355298
Gonzalez-Ramos K, Ramsubeik K, Kaeley G. Case of calcinosis cutis associated with Sjogren’s syndrome. Clin Case Reports. 2023;11(6):7628. https://doi.org/10.1002/ccr3.7628.e