
Anatomical danger zone reconsidered: a micro-CT study on dentine thickness in mandibular molars
Abstract
Aim: To investigate the smallest dentine thickness in mesial canals of mandibular molars along the cervical and middle thirds of the root by means of a micro-computed tomographic (micro-CT) technology and digital image analysis.
Methodology: Fifty mesial roots of mandibular molars having two independent canals (mesiobuccal and mesiolingual), in the coronal and middle levels, were selected and scanned in a micro-CT device. After reconstruction procedures, approximately 468 slices per root covering the 7 mm below the furcation area of the mesial root were analysed to measure the smallest dentine thickness (danger zone [DZ]) in each slice from both distal and mesial regions of the mesial canals by an automatic segmentation process.
Results: The DZ values in the mesiobuccal canals varied from 0.67 to 1.93 mm, with an average of 1.13 ± 0.21 mm. For the mesiolingual canals, the DZ varied from 0.77 to 1.89 mm with an average of 1.10 ± 0.21 mm. There was no correspondence in the DZ between the mesiobuccal and mesiolingual canals at the same cross-sectional level in 71% of the specimens. Moreover, the smallest dentine thickness was towards the mesial region of the roots in 22% and 18% of the mesiolingual and mesiobuccal canals, respectively.
Conclusions: The smallest dentine thickness was on the mesial plane of the roots in about 40% of the canals. The vertical location of the DZ in relation to the furcation area was in the middle third of the root.
Introduction
Midroot perforations are normally caused by over-instrumentation on an already thin dentinal wall, which may seriously compromise the outcome of root canal treatment (Estrela et al. 2018). These perforations have been related historically to the distal area of mesial roots in mandibular molars, and thus, Abou-Rass et al. (1980) introduced the concept of the ‘danger zone’ (DZ) in the early 1980s. In fact, these authors formally reported what experienced clinicians already knew: often, mesial canals of mandibular molars do not assume a central position in the root with the distal area between the canal and root bifurcation being relatively thin, the so-called DZ, which is more vulnerable to strip perforations. On the other hand, the safety zone was described as the mesial area of the mesial root with a thicker dentine layer, which is often minimally instrumented by endodontic instruments. In short, Abou-Rass et al. (1980) pointed out the importance of this anatomical area during canal shaping and, since then, many studies have evaluated the safety of various preparation techniques in mesial canals of mandibular molars (Garcia Filho et al. 2003, Akhlaghi et al. 2010, Silva et al. 2017).
The anatomy of the DZ as well as the assessment of canal preparation techniques and instruments has been based on destructive and invasive approaches (i.e. sectioning methods) (Garcia Filho et al. 2003, Akhlaghi et al. 2010). This leads to serious experimental limitations as it allows the analysis of only a few slices per root.
In the early 2000s, the introduction of micro-computed tomographic (micro-CT) imaging opened new possibilities for endodontic research since this technology allows precise nondestructive longitudinal two-dimensional (2D) and three-dimensional (3D) assessments (Peters et al. 2001, 2003, De-Deus et al. 2015, 2016, Silva et al. 2017), because micro-CT is based on a powerful X-ray source, which allows visualization and measurement of the outer and inner structures of an opaque object without needing previous sample preparation or chemical fixation. For instance, micro-CT with mathematical modelling has provided information on the dentine thicknesses in 1-mm intervals (Harris et al. 2013). However, detailed morphological information about the DZ remains inconsistent, sparse and sometimes controversial, as the evaluation of just a few cross sections per sample is rather meaningless, especially when using micro- CT technology. Lee et al. (2015) appears to be the only micro-CT study that used high-resolution and smaller slice intervals (0.1 mm). Therefore, a comprehensive anatomical study of danger and safety zones in mesial roots of mandibular molars is timely and may help reduce either the risk of midroot perforations towards the furcation area or an unnecessary loss of sound dentine tissue, which appears to contribute to the long-term survival of teeth (Soares et al. 2008).
The current study has a descriptive nature and was designed to investigate the smallest dentine thickness in mesial canals of mandibular molars along the cervical and middle thirds of the root by means of micro-CT technology and digital image analysis.
Materials and methods
Sample selection and imaging
The present ex vivo study was approved by the Ethical Research Committee of Fluminense Federal University. Initially, one hundred moderately curved mesial roots (10–20°) of first and second mandibular molars, selected according to Schneider’s method (Schneider 1971), with 10 ± 1 mm in length, were imaged with a micro-CT scanner (SkyScan 1173; Bruker microCT, Kontich, Belgium) at 14.25 lm (pixel size), 70 kV, 114 mA, 180° rotation around the vertical axis, rotation step of 0.7°, camera exposure time of 250 milliseconds and frame average of 4, using a 1-mm-thick aluminium filter. The images were reconstructed (NRecon v. 1.7.1.6; Bruker microCT) with similar parameters for beam hardening (35–45%), ring artefact correction (3–5) and contrast limits (0–0.05). Then, fifty mesial roots with two independent canals (mesiobuccal and mesiolingual), at the coronal and middle levels, were selected. None of the specimens had a root filling, root caries, cracks, fractures, and internal or external resorption.
Image analysis
The volume of interest was selected extending from the furcation level to 3 mm from the anatomical apex of the mesial roots, corresponding to approximately 468 slices per root, for a total of 23400 slices. An image analysis routine was developed to measure the minimal dentine thickness from both distal and mesial aspects of the mesial canals of mandibular molars by using a previously validated BoneJ plug-in (Doube et al. 2010) implemented into the Fiji/ImageJ software (Fiji v.1.51n; Madison, WI, USA). First, a 3D median filter was applied to the stacks in order to reduce overall noise (Neves et al. 2015) and the dentine was binarized using a minimum threshold algorithm. Then, the BoneJ plug-in was used to identify the position and measure the smallest dentine thickness in each slice for both mesial canals.
Three-dimensional mapping of the dentine thickness was created and saved for structure thickness in CTAn v.1.15 software (Bruker microCT), and loaded into CTVox v.3.3 software (Bruker microCT) to generate colour-coded 3D models of the mesial roots of mandibular molars.
Results
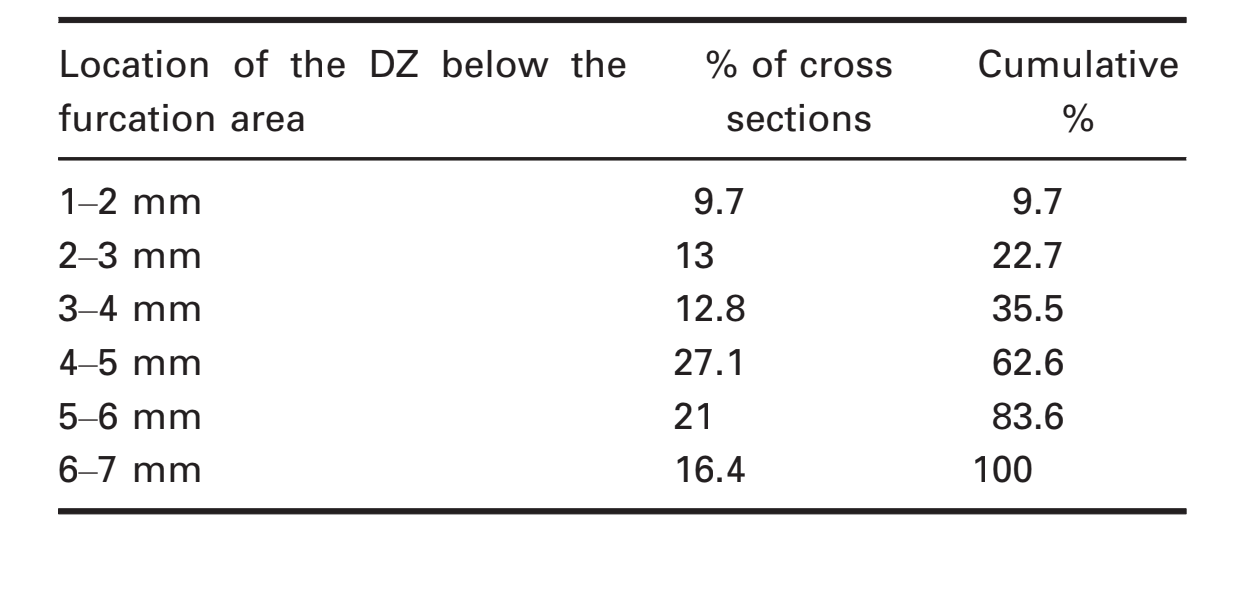
Table 1 presents descriptive data for all specimens regarding the smallest dentine thickness (DZ) and its location relative to the furcation area. Table 2 shows the location of the DZ for all specimens according to the distance from the furcation area distributed in 1-mm intervals.
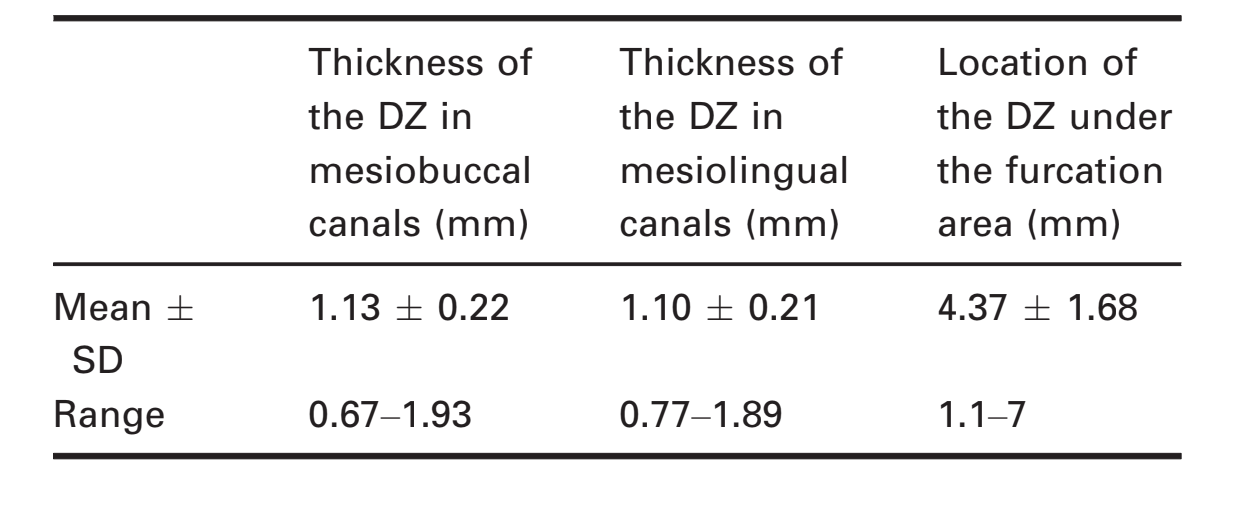
The DZ values in the mesiobuccal canals varied from 0.67 to 1.93 mm, with an average of 1.13 ± 0.21 mm. For the mesiolingual canals, the DZ varied from 0.77 to 1.89 mm, with an average of 1.10 ± 0.21 mm. There was no correspondence in the DZ between the mesiobuccal and mesiolingual canals at the same cross-sectional level in 71% of the specimens. Moreover, the DZ was towards the mesial region of the roots in 22% and 18% of the mesiolingual and mesiobuccal canals, respectively (Figs 1 and 2).
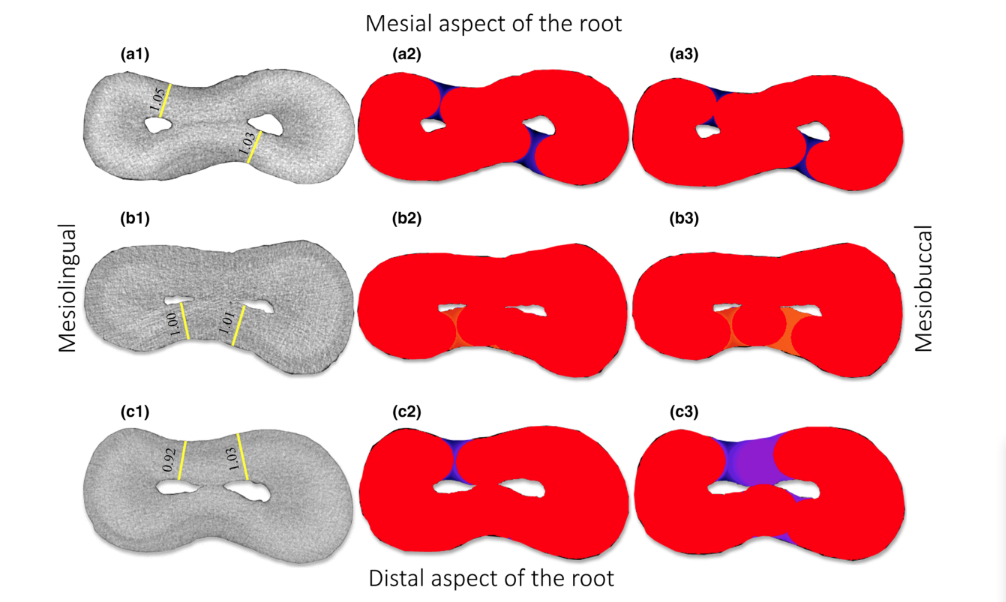
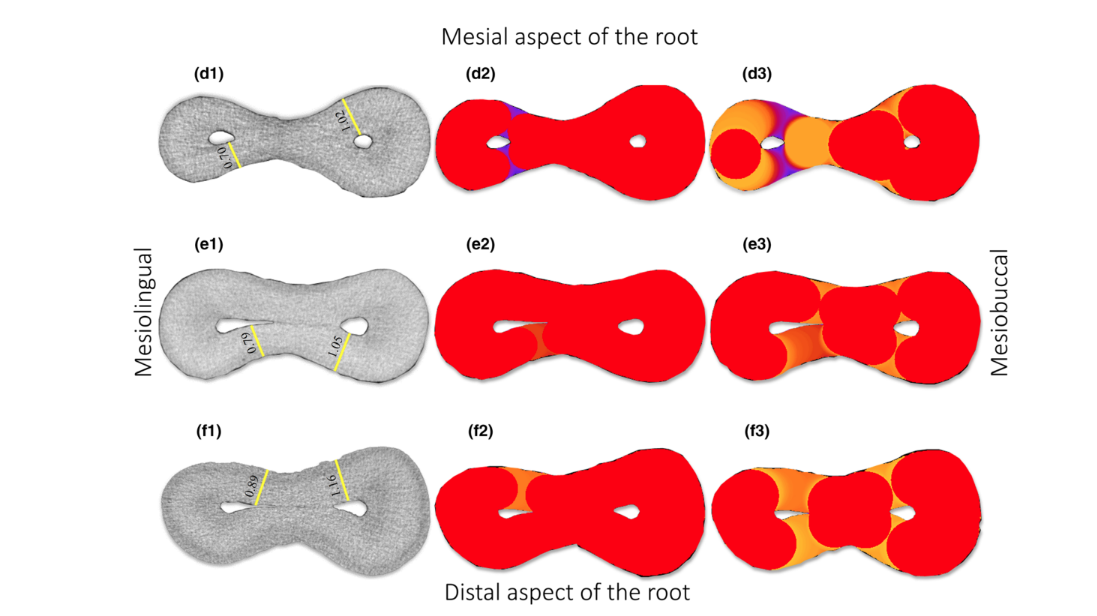
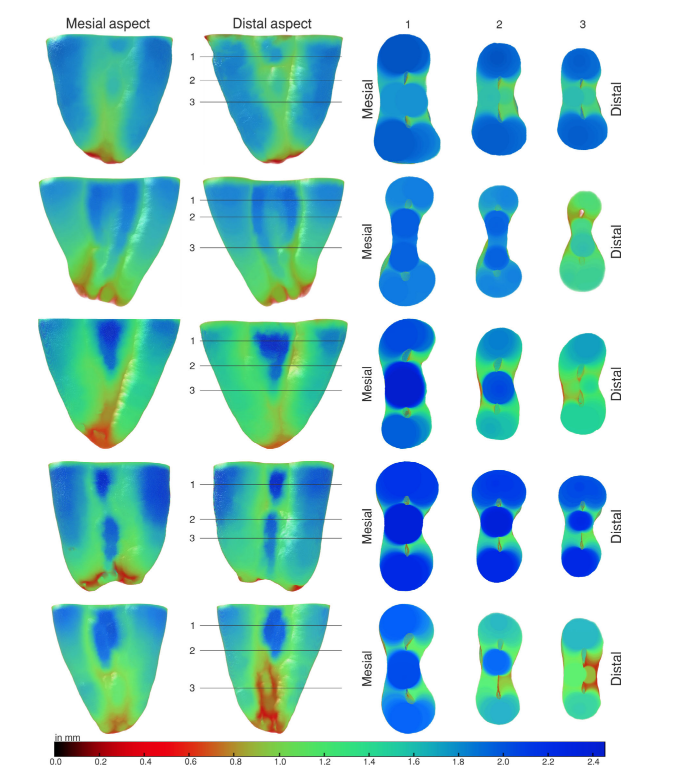
Figure 3 shows colour-coded representations of the dentine thickness throughout mesial roots of five representative mandibular molars. Qualitative analysis demonstrated that the noncentred position of the mesial canals and the asymmetric shape of the root resulted in variable thickness of the dentine at different levels and directions, including areas towards the mesial aspect of the root in some cases.
Discussion
The current study provided two innovative results regarding the anatomical DZ. First, the smallest dentine thickness was towards the mesial plane of the roots in around 40% of the canals (22% and 18% of the mesiolingual and mesiobuccal canals, respectively). Secondly, the vertical location of the DZ in relation to the furcation area was towards the middle third of the root.
Relevant original data revealed by the present study were about the position of the DZ in the cross-sectional plane of the root. Traditionally, the understanding from the classic concept of the DZ refers to the distal area between the main canal space and the root bifurcation, which has the thinnest dentine and is more prone to the development of strip perforations. However, the current results revealed that the DZ was displaced towards the furcation area in only 60% of the evaluated cross sections. In the other 40% of the slices, the thinnest dentine was located on the mesial region of the roots, which contrasts with the generally held view (Abou-Rass et al. 1980). Also using a micro-CT imaging analysis, Lee et al. (2015) found the thinnest root canal wall on the mesial portion of the root in between 15% and 33% of the specimens, which is consistent with the present results.
The DZ evaluated in the present study was located up to 4 mm under the furcation area in only 35% of the specimens, whilst the majority of the samples revealed that the DZ was between 4 and 7 mm below the furcation area. In other words, DZs prone to either strip perforation or unnecessary loss of dentine are more towards the middle third of the root (4.37 ± 1.68 mm under the furcation area) than previously reported (Table 1). This finding is innovative inasmuch as previous information described the anatomical position of the DZ is concentrated up to 4 mm below the furcation level (Kessler et al. 1983, Berutti & Fedon 1992, Garcia Filho et al. 2003, Sauáia et al. 2010, Tabrizizadeh et al. 2010, Akhlaghi et al. 2015).
It is worth mentioning that the mean smallest dentine thickness along the distal surfaces in mesial roots of mandibular molars found in this study was 0.67 mm, which is smaller than usually reported in the literature: Lim & Stock (1987) = 0.94 mm, Garcia Filho et al. (2003) = 0.79 mm, Kessler et al. (1983) = 1.08 mm, Akhlaghi et al. (2015) = 1.05 mm, Berutti & Fedon (1992) = 1.2 mm and Tabrizizadeh et al. (2010) = 1.3 mm. The information on the smallest dentine thickness values was mainly created from investigations based on destructive sectioning methods and direct optical microscopy observation of a few slices of the mesial roots. One exception is a cone beam computed tomography study with low spatial resolution (Akhlaghi et al. 2015). The other exception is a micro-CT study which revealed values of 0.81 mm, but the measurements were taken only 1.5 mm below the furcation area (Harris et al. 2013). The original findings presented in this study are probably a consequence of the methodological advancement achieved with the interplay between the micro-CT imaging technology and an automatic computational routine for digital image analysis and processing. In fact, the accumulated body of evidence on the DZ was created essentially based on destructive methods and direct microscopy observation of a few root sections per tooth (Kessler et al. 1983, Berutti & Fedon 1992, Garcia Filho et al. 2003, Sauáia et al. 2010, Tabrizizadeh et al. 2010). Moreover, even studies that used micro-CT imaging technology only performed the evaluation of a few cross-sectional images (Harris et al. 2013, Ordinola-Zapata et al. 2019). In this study, a full 3D mapping of dentine thickness along the entire cervical and middle thirds was performed rendering data from hundreds of cross sections per root. Furthermore, measurements performed by an automatic computational routine are more robust and reliable. Markedly, the automated analysis allowed the rapid measurement of thousands of slices rendering the experiment less time-consuming and labour-intensive. Moreover, the age of teeth is an uncontrolled variable that may have influenced the present results at least to some degree. Stored teeth were used with unknown information about age; as long as age affects the overall canal size, it is likely to affect the overall dentinal thickness.
Conclusions
The smallest dentine thickness in extracted mandibular first and second molars was towards the mesial plane of the roots in approximately 40% of the canals, whilst the overall vertical location of the DZ was towards the middle third of the root.
Authors: G. De-Deus, E. A. Rodrigues, F. G. Belladonna, M. Simões-Carvalho, D. M. Cavalcante, D. S. Oliveira, E. M. Souza, K. A. Giorgi, M. A. Versiani, R. T. Lopes, E. J. N. L. Silva, S. Paciornik
References:
- Abou-Rass M, Frank AL, Glick DH (1980) The anticurvature filing method to prepare the curved root canal. Journal of the American Dental Association 101, 792–4.
- Akhlaghi NM, Kahali R, Abtahi A, Tabatabaee S, Mehrvarzfar P, Parirokh M (2010) Comparison of dentine removal using V-taper and K-Flexofile instruments. International Endodontic Journal 43, 1029–36.
- Akhlaghi NM, Bajgiran LM, Naghdi A, Behrooz E, Khalilak Z (2015) The minimum residual root thickness after using ProTaper, RaCe and Gates-Glidden drills: a cone beam computerized tomography study. European Journal of Dentistry 9, 228–33.
- Berutti E, Fedon G (1992) Thickness of cementum/dentin in mesial roots of mandibular first molars. Journal of Endodontics 18, 545–8.
- De-Deus G, Belladonna FG, Silva EJ et al. (2015) Micro-CT evaluation of non-instrumented canal areas with different enlargements performed by NiTi systems. Brazilian Dental Journal 26, 624–9.
- De-Deus G, Belladonna FG, Marins JR et al. (2016) On the causality between dentinal defects and root canal preparation: a micro-CT assessment. Brazilian Dental Journal 27, 664–9.
- Doube M, Kłosowski MM, Arganda-Carreras I et al. (2010) BoneJ: free and extensible bone image analysis in ImageJ. Bone 47, 1076–9.
- Estrela C, Decurcio DA, Rossi-Fedele G, Silva JA, Guedes OA, Borges AH (2018) Root perforations: a review of diagnosis, prognosis and materials. Brazilian Oral Research 32, e73.
- Garcia Filho PF, Letra A, Menezes R, Carmo AM (2003) Danger zone in mandibular molars before instrumentation: an in vitro study. Journal of Applied Oral Sciences 11, 324–6.
- Harris SP, Bowles WR, Fok A, McClanahan SB (2013) An anatomic investigation of the mandibular first molar using micro-computed tomography. Journal of Endodontics 39, 1374–8.
- Kessler JR, Peters DD, Lorton L (1983) Comparison of the relative risk of molar root perforations using various endodontic instrumentation techniques. Journal of Endodontics 9, 439–47.
- Lee JK, Yoo YJ, Perinpanayagam H et al. (2015) Three-dimensional modelling and concurrent measurements of root anatomy in mandibular first molar mesial roots using micro-computed tomography. International Endodontic Journal 48, 380–9.
- Lim SS, Stock CJ (1987) The risk of perforation in the curved canal: anticurvature filing compared with the stepback technique. International Endodontic Journal 20, 33–9.
- Neves AA, Silva EJ, Roter JM et al. (2015) Exploiting the potential of free software to evaluate root canal biomechanical preparation outcomes through micro-CT images. International Endodontic Journal 48, 1033–42.
- Peters OA, Schönenberger K, Laib A (2001) Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. International Endodontic Journal 34, 221–30.
- Ordinola-Zapata R, Martins JNR, Versiani MA, Bramante CM (2019) Micro-CT analysis of danger zone thickness in the mesiobuccal roots of maxillary first molars. International Endodontic Journal 52, 524–9.
- Peters OA, Peters CI, Scho€nenberger K, Barbakow F (2003) ProTaper rotary root canal preparation: effects of canal anatomy on final shape analysed by micro CT. International Endodontic Journal 36, 86–92.
- Sauáia TS, Gomes BP, Pinheiro ET et al. (2010) Thickness of dentine in mesial roots of mandibular molars with different lengths. International Endodontic Journal 43, 555–9.
- Schneider SW (1971) A comparison of canal preparations in straight and curved root canals. Oral Surgery Oral Medicine Oral Pathology 32, 271–5.
- Silva EJNL, Pacheco PT, Pires F, Belladonna FG, De-Deus G (2017) Microcomputed tomographic evaluation of canal transportation and centring ability of ProTaper Next and Twisted File Adaptive systems. International Endodontic Journal 50, 694–9.
- Soares PV, Santos-Filho PC, Queiroz EC et al. (2008) Fracture resistance and stress distribution in endodontically treated maxillary premolars restored with composite resin. Journal of Prosthodontics 17, 114–9.
- Tabrizizadeh M, Reuben J, Khalesi M, Mousavinasab M, Ezabadi MG (2010) Evaluation of radicular dentin thickness of danger zone in mandibular first molars. Journal of Dentistry (Tehran) 7, 196–9.