
How to upgrade from suction deglutition to swallowing deglutition trough cortical or subcortical networks
The deformities that orthodontists have to cure are mostly caused by a lack of balance between the opposing forces produced by the cheek muscles and the forces generated by the tongue.
Whether orthopedic treatment in the deciduous dentition, orthodontic treatment in the mixed or permanent dentition, it is necessary to reach at the end of any treatment a functional balance that will ensure the stability of the results.
The transition from sucking deglutition to the physiological deglutition takes place spontaneously for 60% of the children between the age of three and a half and four by a subcortical activation of the a pre-existing neurological wiring which have just matured.
Suction deglutition was a physiological function during the first years. It has a paleocortical origin, and the facial nerve controls it. But it becomes archaic when the full set of teeth is in place, and when the mastication appears.
- If suction-swallowing habit continues, the forces exerted by the labio-jugal muscles will disturb the physiological growth and will lead to various skeletal disorders in the three dimensions of space.
If it does not happen by itself, then, like in a computer, a new program will have to be downloaded, controlled by the trigeminal nerve
It is what the practitioner or the speech therapist is going to do through a series of exercises to code a new praxis. But even with an accurate cooperation of the child, it is a long and complicated process because it need a participation of the cortical brain.
According to Eric Kandel, Nobel Price of Medicine in 2000, when this action comes from the cortical area we have a stimulation of neurotransmitters in our synapses, but when it comes from the subcortical area we have a creation of new synapses.
The swallowing rehabilitation must not be based on the control of voluntary movements but on the stimulation of automatic movements:
- Froggymouth is a new appliance which helps young children at the age of 3-4 years to use the best swallowing method for a toothed patient through the subcortical way and not anymore the suction deglutition method.
- This Appliance is based on the idea of deconnection between the upper lip and the lower one.
Froggymouth is not placed inside the mouth but beetwen the lips (fig.1).
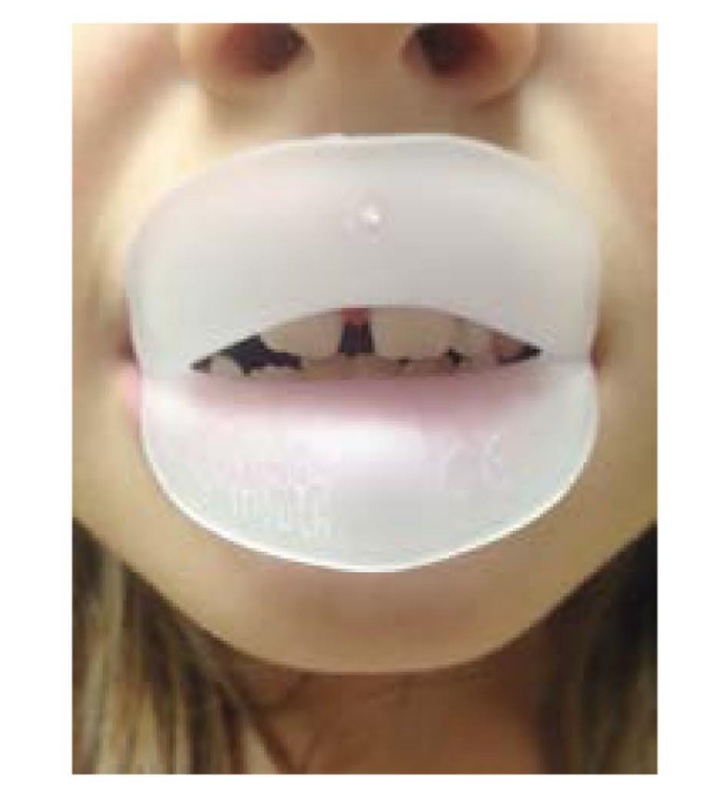
It will prevent the upper one from touching the lower one. So, it is impossible to create the negative pressure which is necessary during suction deglutition thanks to a water-tight joint around the lips. Indeed, it will force the child to find by himself a new way for the deglutition, in the lower part of his brain, by raising the upper back part of the tongue to the palatal bone when the teeth are in occlusion.
The activity of the seventeen muscles of the tongue against the internal side of the teeth allows an optimal stimulation of the transversal and antero-posterior growth of the dental arch.
This appliance has to be worn 15 minutes per day and should not be worn during the night like a trainer as the quality of the sleep is so important for young children. Froggymouth must be worn in front of a TV screen to have a good orientation of the head and to catch the attention of the patient. It will stimulate his neuron circuits, which are related to the subconscious functions. At rest the lips are not in contact, the teeth are in occlusion and the trigeminal nerve control this program.
At the opposite, when the lips are closed, the teeth will not be in contact, and the facial nerve will be the leader, the child will use the old swallowing pattern.
This Appliance is only an auxiliary that you will be able to use during your treatments for a few weeks whatever the techniques you apply (functional or mechanical).
It is obvious that results will be achieved much faster if the muscles and the appliance are both working in the same direction rather than if they are fighting against each other.
Froggy mouth is perfectly adapted to young children and it can even be used alone if the deformity is slight:
- The simple fact to rebalance the functions will allow a spontaneous correction of slight deformity when the child still has deciduous teeth.
Conclusion
Froggymouth will not only reduce the length of your treatments but much more important; it will ensure its durability when the treatment will be over and then reduce the risk of relapse.