
Prevalence of Elongated Ossified Styloid Process and Eagle Syndrome in the Population Attending the Orthodontics Clinic of CEDHUM
Machine translation
Original article is written in ES language (link to read it) .
Summary
Introduction: The ossified styloid process, an anatomical structure measuring 20 to 25 mm, is considered elongated from 30 mm; a percentage of the population has a growth that affects surrounding structures and generates various symptoms. The objective of this study is to determine the prevalence of elongated ossified styloid process in the orthodontic population of the Center for Humanities (CEDHUM).
Materials and methods: Clinical records with panoramic radiographs from 2015 to June 2018 were reviewed, and the presence of elongated ossified styloid process was digitally observed. They were captured in the Kodak 8000C digital orthopantomograph program, calibrated in mm, measuring digitally from the base to the tip of the process bilaterally; the data were analyzed in Excel and Stata SE 14 statistical package.
Results: The prevalence of elongated ossified styloid process was 20.49% (95% CI 14.76-27.69), of which 95.24% (n = 40/42) was bilateral. When stratified by sex, 21.90% of women and 17.65% of men were diagnosed with elongated ossified styloid process, and no statistically significant differences were observed (p = 0.478).
Conclusions: The categorization as Eagle syndrome was 42.86%, and the average age was 20.47 years in women and 19.26 years in men. The location of the elongated ossified styloid process was bilateral in 95.24% (n = 40/42); when stratifying by sex, 21.90% corresponds to females and 17.65% to males. The prevalence of the elongated ossified styloid process was 20.49%, being more prevalent in the female gender than in the male, with no statistically significant differences observed.
Introduction
Eagle syndrome is a rarely identified entity clinically and radiographically, the first descriptions of this condition were by Marchetti in 1652; Luke in 1870; Weinlecheren in 1872; and was later described by Dr. Watt W. Eagle in 1937, who reported several cases of elongated styloid processes associated with vague pain symptoms in the head, neck, and orofacial regions, his work gave rise to the term "Eagle syndrome." It is a little-known entity, but it should be considered in the differential diagnosis of some cervical pain, in cases of glossopharyngeal neuralgia and temporomandibular dysfunction.
4% of the general population presents an elongation of the styloid process and only 0.16% presents symptoms. The physiological length of the styloid process is 20-30 mm and is classified as type I: physiological length, type II: elongated, type III: pseudoarthrosis, type IV: bony chain, and V: complete ossification.
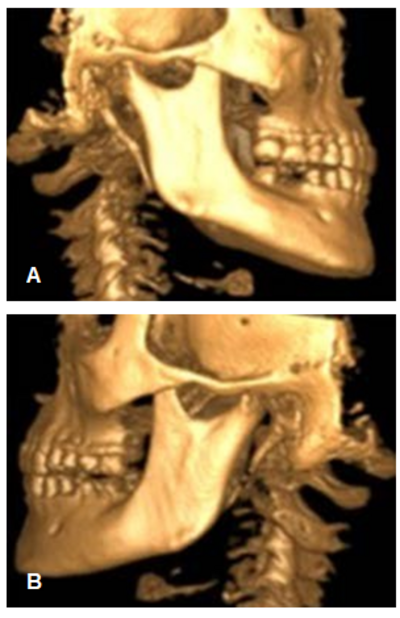
The majority of affected patients do not present symptoms, although the pressure exerted by this altered structure against neighboring structures can trigger a wide variety of symptoms (Figure 1).
Material and methods
Cross-sectional study conducted at the Clinic of the Center for Humanities (CEDHUM), located in the municipality of Jiutepec in the State of Morelos, Mexico, during the period from January 2015 to June 2018.
All subjects over 15 years old who attended orthodontic consultations during the study period and who signed the informed consent were included in the study. The only exclusion criterion considered was the lack of a complete clinical file.
For the diagnosis of elongated styloid process, a panoramic radiograph was taken of each patient. The measurement of the length of the styloid process was performed on those that were visually observed to be elongated and were captured in the Kodak 8000C digital orthopantomograph program. Prior to measurement, the reading of the panoramic radiograph measurement was individually calibrated by measuring the length of the clinical crown of an upper central incisor (11 or 21) to subsequently measure in the program from the base to the tip of the ossified styloid process (Figure 2). The values provided by the Kodak Dental Imaging Software 6.12.26.0, in mm, were transferred to the patients' database.
Based on the observations from the panoramic radiograph, the elongations were classified as bilateral (if they were present on both sides) and unilateral (if they were only on one side). On the other hand, patients who presented with an elongated ossified styloid process on their panoramic radiograph were questioned and clinically palpated to identify whether they exhibited any characteristic symptoms or were asymptomatic.
The general characteristics of the study population included age, sex, unilateral and bilateral elongated ossified styloid process, symptomatic or asymptomatic. The data were captured in an Excel® spreadsheet.
A description by sex of the characteristics of the population was performed using the Mann-Whitney test for continuous variables and the χ2 test for categorical variables. Additionally, to determine the risk factors associated with the elongation of the styloid process, a logistic regression analysis was conducted considering variables such as age and sex. Furthermore, another logistic regression analysis was conducted to evaluate the risk factors associated with the presence of symptoms, considering the length of the styloid process, age, and sex.
The statistical analysis was performed using the Stata SE 14 statistical package.

Results
During the study period from January 2015 to June 2018, 205 clinical records of patients who visited the CEDHUM clinic in Jiutepec, Morelos, Mexico were reviewed.
The average age of the evaluated population was 20.01 years (SD 6.17 years), of which 66.83% (n = 137/205) were women with an average age of 20.47 years (SD 6.56 years), while the average age of men was 19.26 years (SD 5.25 years).
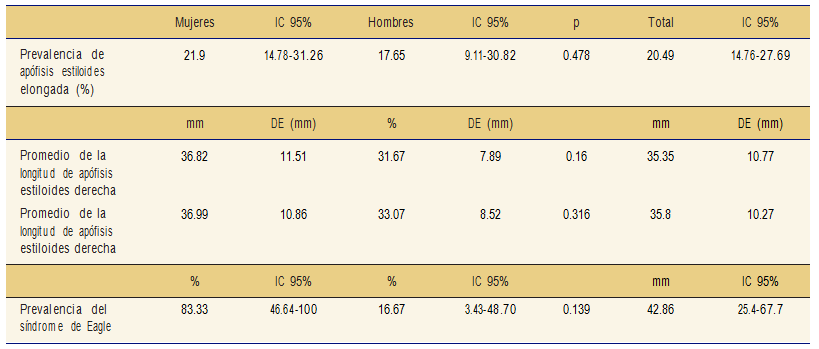
The prevalence of elongated ossified styloid process was 20.49% (CI 95% 14.76-27.69), of which 95.24% (n = 40/42) was bilateral. When stratifying by sex, 21.90% (CI 95% 14.78-31.25) of women and 17.65% (CI 95% 9.11-30.82) of men were diagnosed with elongated ossified styloid process; however, no statistically significant differences were observed (p = 0.478).
The average length of the right elongated styloid process was 35.35 mm (SD 10.77 mm) and 35.8 mm (SD 1.027 mm) on the left side (Table 1).
Of the subjects with elongated ossified styloid process, 42.86 mm (CI 95% 25.4-67.7) were diagnosed with Eagle syndrome due to presenting symptoms characteristic of it. When evaluating the syndrome concerning sex, it was observed to be more frequent in women; no statistically significant differences were found (p = 0.139) (Table 1).
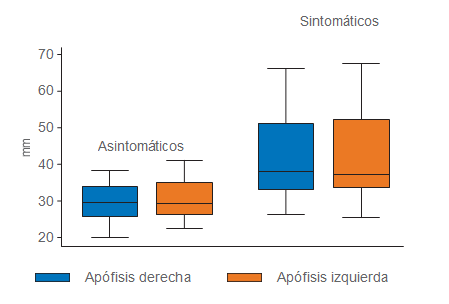
Additionally, the relationship between the length of the styloid process and the symptoms corresponding to Eagle's syndrome was evaluated (Figure 3).
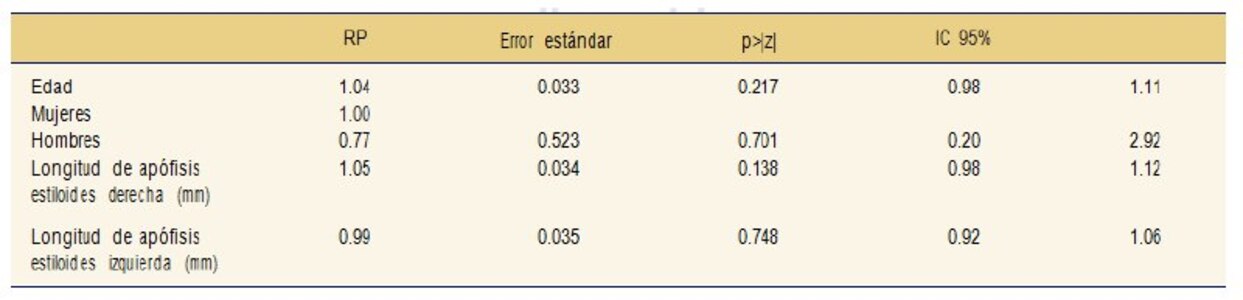
Furthermore, in the multivariate analysis adjusted for sex, it was estimated that the risk of presenting elongation of the styloid process increases on average by 11% for each one-year increase in age, and that association was statistically significant (Table 2). In contrast, when evaluating the association between symptoms and the length of the styloid process while adjusting for age and sex, no statistically significant differences were observed (Table 3).

Discussion
In the present study, the elongated ossified styloid process was confirmed and quantified through panoramic radiographs, and the Eagle syndrome was categorized in the study population.
The prevalence of the elongated ossified styloid process was 20.49%, similar to what was reported by Balcázar and Ramírez, which is 4-28%.
The normal length of the styloid process varies considerably among most individuals, reported to be between 20 to 30 mm, generally considered elongated when it measures more than 25 mm, while other authors mention that it is considered elongated starting from 30 mm. The average found on the right side was 35.35 mm and 35.8 mm on the left side, which coincides with what was reported by Nazar and colleagues.
Other authors such as Sanchez and his team, and D’Addino and colleagues, report that Eagle syndrome occurs between the third and fourth decades of life, and between the ages of 30 and 50 years, respectively. This does not align with the average of the evaluated population in our study, which was 20.01 years, with an average age of 20.47 years for women and 19.26 years for men.
Of the subjects with elongated ossified styloid process diagnosed with Eagle syndrome, it was 42.86%, and when evaluating by sex, it was observed to be more frequent in women, without finding statistically significant differences. This coincides with what was reported by Balcázar and Ramírez.
According to the location of the elongated ossified styloid process, the presence was bilateral in 95.24% (n = 40/42), these results do not agree with those found by Fuentes and his group, who observed more unilateral elongations than bilateral.
Conclusions
According to the limitations of the study, the following can be concluded:
- The prevalence of elongated ossified styloid process was 20.49% (95% CI 14.76-27.69), being more prevalent in the female gender than in the male; however, no statistically significant differences were observed (p = 0.478), which confirms the working hypothesis.
- The categorization as Eagle syndrome was 42.86% (95% CI 25.4-67.7).
- The location of the elongated ossified styloid process was bilateral in 95.24% (n = 40/42), when stratified by sex, 21.90% corresponds to females and 17.65% to males. Of the total elongated ossified styloid processes with symptoms, the average age was 20.47 years in women and 19.26 years in men.
- In the multivariate analysis adjusted for sex, it was estimated that the risk of presenting elongation of the styloid process increases on average by 11% for each unit increase in years of age, and this association was statistically significant.
Authors: Franco Fonseca Balcázar, Julia Salinas Basauri, Irma Yvonne Amaya Larios, Antonio Martínez Ronquillo, Miguel Ángel Reyes
References:
- Raffo LM. Eagle syndrome: case report. Odontoestomatología. 2012; 14 (20): 26-31.
- González JM et al. Eagle syndrome. Importance for the dentist. Literature review. Acta Odontológica Venezolana. 2011; 49 (2).
- Espinoza ML, Ruiz MM. Clinical characteristics of Eagle syndrome. Rev Esp Med Quir. 2013; 18 (3): 264-270.
- Garcia LA et al. Eagle styloid syndrome, clinical case. Acta Méd Grupo Ángeles. 2016; 14 (4): 244-247.
- Tisner NJV et al. Calcification of the styloid ligament: Aubin's stylalgia and Eagle syndrome. Contribution of 5 clinical cases. Research and applied clinical work. Rehabilitation Service of the Miguel Servet University Hospital of Zaragoza. Orl Aragon. 2003; 6 (2): 5-12.
- Ortega AV et al. Review of the elongation of the styloid process. Possible genetic etiology. Regarding three clinical cases. Rev Cien Dent. 2015; 12 (1): 45-50.
- Sanchez LE, Repetto LJL, Gallego GR. Odynophagia and cervicobrachialgia in Eagle syndrome. Description of a case. ORL Journal. 2017; 8 (1): 65-68.
- Hassan MK et al. Fractured styloid process masquerading as neck pain: Cone-beam computed tomography investigation and review of the literature. Imaging Sci Dest. 2018; 48: 67-72.
- Gino ML. Eagle syndrome. Literature review. Rev Otorrinolaringol Cir Cabeza y Cuello. 2016; 76: 121-126.
- Mareque BJ et al. Intraoral approach in Eagle syndrome. Presentation of a clinical case. Rev Esp Cirug Oral y Maxilofac. 2011; 33 (4): 157-161.
- Balcázar RLE, Ramírez AYL. Eagle syndrome. Gac Med Me. 2013; 149: 552-554.
- Villalba LMA, Miranda VE. Eagle syndrome; case report. Mexican Association of Oral and Maxillofacial Surgery. 2009; 5 (1): 26-31.
- Thoenissen P et al. Eagle’s syndrome – A non-perceived differential diagnosis of temporomandibular disorder. Int J Surg Case Rep. 2015; 15: 123-126.
- Smerilli A, Flores JM. Eagle syndrome. Clinical case. Rev Fac Odontología. 2014; 29 (67): 35-37.
- Nazar SR et al. Eagle syndrome in otorhinolaryngology. Clinical Hospital University of Chile Journal. 2008; 19: 156-161.
- D’Addino JL et al. Eagle syndrome, styloid process extending to the hyoid. Archives of Medicine. 2017; 17 (2): 434-436.
- Fuentes FR et al. Styloid process in a sample of panoramic radiographs from the city of Temuco-Chile. Int J Morphol. 2007; 25 (4): 729-733.