
Treatment of Pathological Tooth Wear
Machine translation
Original article is written in RU language (link to read it) .
Treatment of pathological tooth wear presents certain difficulties related to disturbances in various elements of the masticatory apparatus. Increased wear causes disturbances in the temporomandibular joint, bone tissue, and masticatory muscles. Such disorders further exacerbate the pathological process, complicating the identification of cause-and-effect relationships and the creation of effective prevention and treatment plans that can stop the increased wear.
Effective treatment methods for patients with pathological wear are presented in the online course Pathological Wear: Treatment.

Treatment of Generalized Pathological Wear
Preparatory stage of treatment for generalized pathological wear
During the preparatory stage of treatment for pathological wear, it is important to correctly determine the position of the lower jaw, eliminate its distal displacement, and restore the height of the lower third of the face. At this stage, radiological diagnostics of the position of the elements of the mandibular joint are necessary.
Restoration of the height of the lower facial section
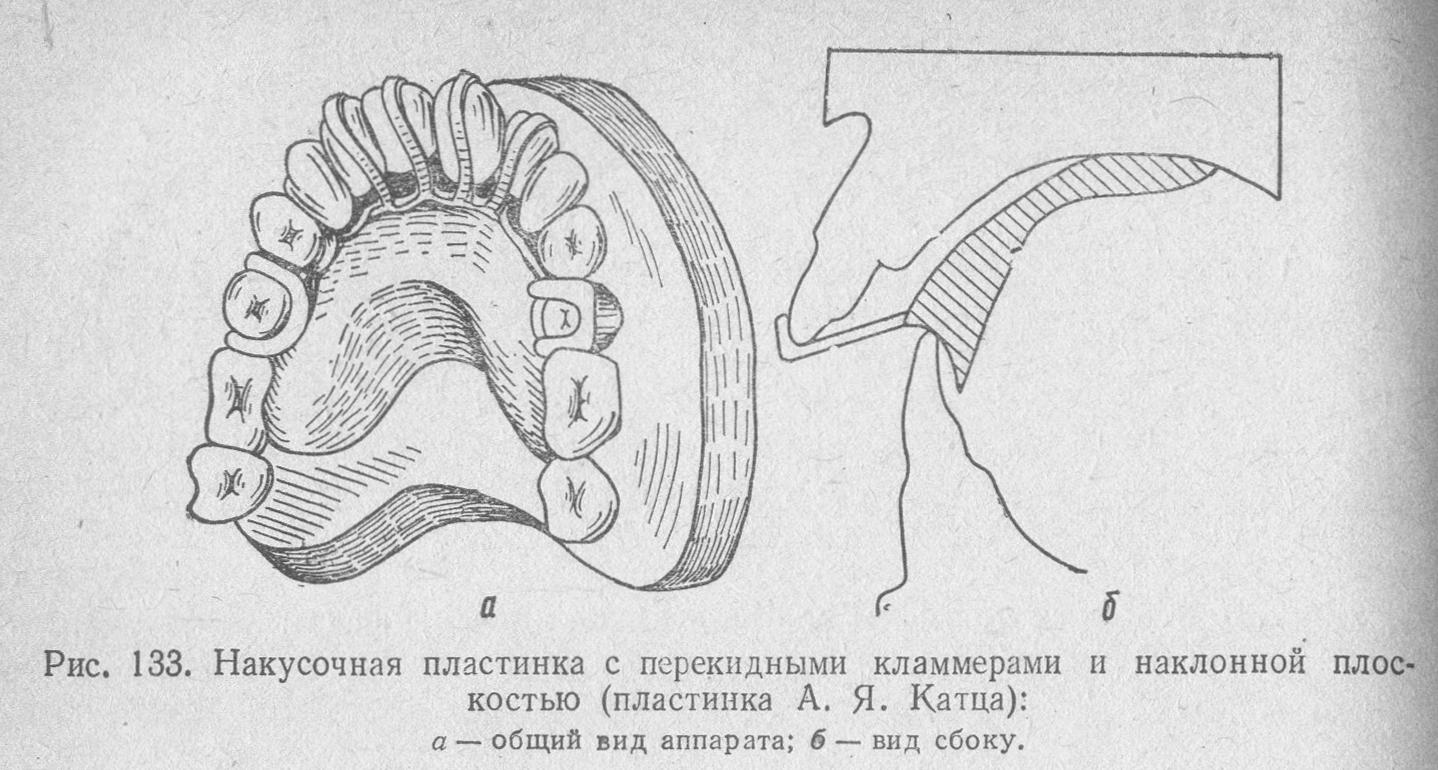
To restore the height of the lower facial section, dental caps and provisional removable and non-removable prostheses are used. The distal displacement of the lower jaw is conducted using caps with an inclined plane and plates with an inclined plane and a biting platform.
In the process of wear, there is a restructuring of bone tissue and hypertrophy of the alveolar ridge. The elimination of dental-alveolar elongation is carried out using orthodontic, surgical, appliance-based, and combined methods.
Increased wear often accompanies reactions from the pulp, dystrophic processes in it, including sclerosis and the deposition of calcificates. Therefore, in clinical situations, when there is significant loss of the hard tissues of the tooth crown and to prevent complications from the pulp, endodontic preparation of the teeth and restoration of the core part of the tooth with post constructions may be necessary.
Permanent prosthetics for pathological wear
For permanent prosthetics in cases of pathological wear, various types of crowns, inlays, and for defects in dental rows, bridge prostheses, implant constructions, clasp prostheses, and their combinations are used. When there are few supporting teeth, it is advisable to use removable prostheses with various types of locking attachments and telescopic fixation.
When restoring teeth with increased wear, it is effective to use metal inlays, however, in the aesthetically important area, it is advisable to use combined metal-plastic and metal-ceramic inlays, as well as all-ceramic inlays.
Similar to crowns on the chewing group of teeth, it is advisable to make them cast metal, whereas the use of stamped constructions is unacceptable, as they wear out quickly and become unusable. A compromise is the use of stamped crowns with cast metal protectors.
The most successful in terms of aesthetics and function are combined constructions with a cast metal frame and a coating of plastic or ceramics. However, if the patient has parafunctions, chipping of the coating can occur. In such cases, metal-plastic constructions are easier to restore.
In addition to orthopedic treatment, a medicinal method can also be used, aimed at eliminating hyperesthesia, and a therapeutic method that allows the restoration of lost hard tissues using composite materials. The method is quite effective, requires sufficient skills of a dental therapist, and competent motivation of the patient to achieve effective dynamic observation.

Bridge Prostheses
For the treatment of increased wear compounded by defects in dental rows, bridge prostheses are used. The principles of prosthetics with bridge prostheses are the same as with inlays and crowns, involving the effective use of cast metal structures with ceramic or plastic veneers to restore aesthetics.
Clasp dentures with occlusal pads are also effective, which do not require the preparation of the supporting teeth. Sometimes, teeth correction is necessary, which involves grinding down sharp edges to prevent them from chipping under the pressure of the clasp denture.
Surgical Treatment
If necessary to correct deformations of the dental arches, surgical treatment may be used (correction of alveolar ridges, removal of protruding teeth), shortening of teeth, and appliance-based methods.
Therapeutic Occlusal Plates
To eliminate dental alveolar elongation, therapeutic occlusal plates are used, allowing the bite to be disconnected by up to 2 mm at a time. After 1-2 months, adaptation to the new bite height occurs, and the process is repeated until the desired result is achieved.
Tooth Caps
For addressing pathological wear of the II and III degrees, tooth caps are used. Tooth caps allow for a one-time disclusion of the bite up to 4 mm in height. Initially, the cap is used as a removable prosthesis until the patient fully adapts to it. Afterwards, the cap is fixed and the patient is monitored for a month, after which, if necessary, the height of the bite is increased, keeping in mind that the rest height should be 2 mm greater than the new occlusal height.
After restoring the height of the bite, prosthetics are carried out. If there are defects in the dental arches, the cap is shortened in the area of the defect, and the discluded bite in this area allows for prosthetics. If there are no defects in the dental arches, the cap is shortened in the area of the molar group of teeth and their prosthetics are carried out, maintaining the new height on the front teeth.
Elimination of dysfunctions in the temporomandibular joint often begins with restoring the height of the bite to the physiological norm, after which the dysfunctions of the muscles and joints are restored in most patients. If there is a distal displacement of the lower jaw, caps are used that are made to position the lower jaw in the necessary relation to the upper. For large distal displacements (more than 4 mm), caps with an inclined plane are used, allowing for the gradual elimination of the lower jaw displacement.

Treatment of Localized Pathological Wear
Localized pathological wear is most often compensated by local hypertrophy of the alveolar ridge and dental-alveolar elongation, so the first stage of treatment for localized pathological wear is aimed at eliminating the deformation of the dental row. The elimination of dental-alveolar elongation is carried out using a cap or a bite plate on a group of protruding teeth. If it is not possible to use a hardware method, a surgical method may be used to lengthen the crown part of the tooth and resect part of the alveolar ridge.
In cases of severe tooth wear, depulpation and restoration of the core part with pin constructions are performed. Depulpation also helps eliminate hyperesthesia when medication treatment proves ineffective.
After eliminating tooth protrusion, they proceed to prosthetics. For prosthetics, metallic, metal-plastic, and metal-ceramic inlays and crowns are used, as well as covering the occlusal and palatal surfaces of teeth with cast metal overlays to eliminate further wear. In the area of the frontal group of teeth, restoration with composite restorations is also used.

All updated and new restorative and functional treatment protocols for pathological tooth wear are collected in one course Pathological Wear 2.0: Updated and New Treatment Protocols.