
Rehabilitation of severe palatal erosion
Machine translation
Original article is written in RU language (link to read it) .
This article describes the clinical application of biomechanical and occlusal principles to achieve optimal clinical results in the restoration of eroded anterior teeth. The authors of this article deal with complex cases associated with deep bite combined with palatal erosion and tooth wear. This combines centric relation principles and Dahl approaches to create an anterior interocclusal space. It will reduce the need for invasive restoration of the palatal surface.
Learn more about this topic in the webinar: Tooth erosion as one of the factors in the development of pathological abrasion .
The combined use of composite restorations on the palatal surface and ceramic veneers on the labial surface helped optimize aesthetic and functional/biomechanical aspects. This ultra-conservative approach achieved the desired esthetic and biomechanical results by treating localized erosion and wear of the anterior teeth. Therefore, when treating eroded maxillary anterior teeth in deep bites, it is necessary to create adequate space by combining the principles of Dahl and centric relation before using composite materials and porcelain veneers.
Non-carious lesions have a polyetiological nature and are the result of various processes: oxidation (chemical dissolution), stress (abfraction), friction (abrasion of teeth with a toothbrush when brushing), etc. The clinician must take all these reasons into account to make the correct diagnosis and determine the necessary treatment plan.
Erosion is the progressive loss of hard dental tissues due to their dissolution by acids and mechanical action. More recently, the term erosion has been replaced by biocorrosion, which covers chemical, biochemical or electrochemical effects on the hard tissues of the tooth. This causes molecular changes that affect the composition and properties of tooth tissue.
In recent decades, adhesive technology has developed rapidly and, in addition to excellent aesthetics, can also be used to restore function, ensuring maximum preservation of the hard tissues of both anterior and posterior teeth. The adhesive technique has two main advantages:
- adhesive ceramic restorations do not require significant tooth grinding because the existing space created by missing tissue is used;
- The usual principles of "resistance and retention" can be omitted, and instead the bonds between the composite and the ceramic and the composite and the tooth are used.
Localized palatal erosion
The palatal surface of the anterior teeth presents a triple problem for clinicians when preparing this surface for further restoration:
- it provides limited stability and retention of materials due to their concave topography;
- internal stress tends to concentrate on the concave surface;
- limited space relative to the antagonists of the opposite dentition.
The authors offer two treatment options for anterior teeth with palatal erosion.
Recovery options
There are three recovery options to consider.
- Preparation for full crowning of the tooth: The task of tooth preparation and restoration becomes even more difficult in cases of deep bite and combined labial/palatal erosion, in which case clinicians tend to use traditional crown preparation. However, this approach has several disadvantages.
Firstly, such preparation involves grinding off a significant amount of intact tissue in already destroyed teeth; the basic substance of the tooth, necessary for sufficient resistance to stress, is lost. The teeth become short, thin and flat. The clinician may require more invasive procedures such as intraradicular pins, thereby compromising the viability of the pulp.
Secondly, this approach may lead to a higher likelihood of secondary caries due to the fact that the margins of the future restoration are located on dentin, which is exposed to enamel erosion.
Thirdly, this restoration method is potentially unsuccessful compared to veneers, since the crowns have a rigid metal frame lined with ceramics, which has a destructive effect under loads on an already weakened tooth. There is also a problem of gum inflammation due to injury from the edges of the crown.
Therefore, clinicians should minimize the use of approaches that involve more aggressive dissection and consider other treatment modalities.
- Orthodontic treatment: a conservative option that is close to ideal, but time constraints and economic difficulties can sometimes negatively affect the use of orthodontic appliances.
- Enameloplasty: with the consent of the patient, enameloplasty is performed on antagonists, but this can lead to hypersensitivity.
Occlusal principles
In an effort to develop a simple, conservative approach to the treatment of localized erosion and wear of anterior teeth, various authors have described two occlusal principles: the centric relation and the Dahl principle. The combined approach explains the third principle.
- Central relation: Lucia suggested using an acrylic device to record centric occlusion. The same method was subsequently refined to save the space needed to accommodate restorations. Cardoso et al. suggested using a modified anterior disconnector device to reposition the mandible in centric occlusion to first create some space, and then use this space for direct composite restorations. Due to the resiliency of composite materials and the ease of use even with limited thickness, direct composite restorations can be used as disconnectors, and for the same reasons they can be considered an ideal material for restoring palatal surfaces.
- Dahl's principle: Dahl proposed the use of the anterior occlusal plane in the treatment of localized wear of anterior teeth. With this approach, a cast metal apparatus is used over a period of 4-6 months to create space by separating the lateral teeth. This combined approach restores posterior occlusion while maintaining anterior space. Today, with the development of adhesive dentistry, direct composite restorations can be used as temporary restorations to achieve the same goals.
- Combined Clinical Approach: For severe generalized wear and erosion involving the anterior and posterior teeth, it may be reasonable to restore lost height by opening the bite by restoring the posterior teeth (i.e., complementary approach). Considering this and the multiple contacts in the central occlusion position, a space of several millimeters is provided to restore the lost shape without invasive interventions.
However, a major problem arises in cases of localized wear on the palatal surfaces of the upper anterior teeth, with little or no wear on the posterior teeth. The use of veneers on the palatal surface (modified Dahl principle) is a conservative option and is used in cases where this is possible. There are cases of successful treatment of such clinical cases using an adhesive technique along with a modified Dahl principle, allowing the remaining portion of the tooth to be preserved.
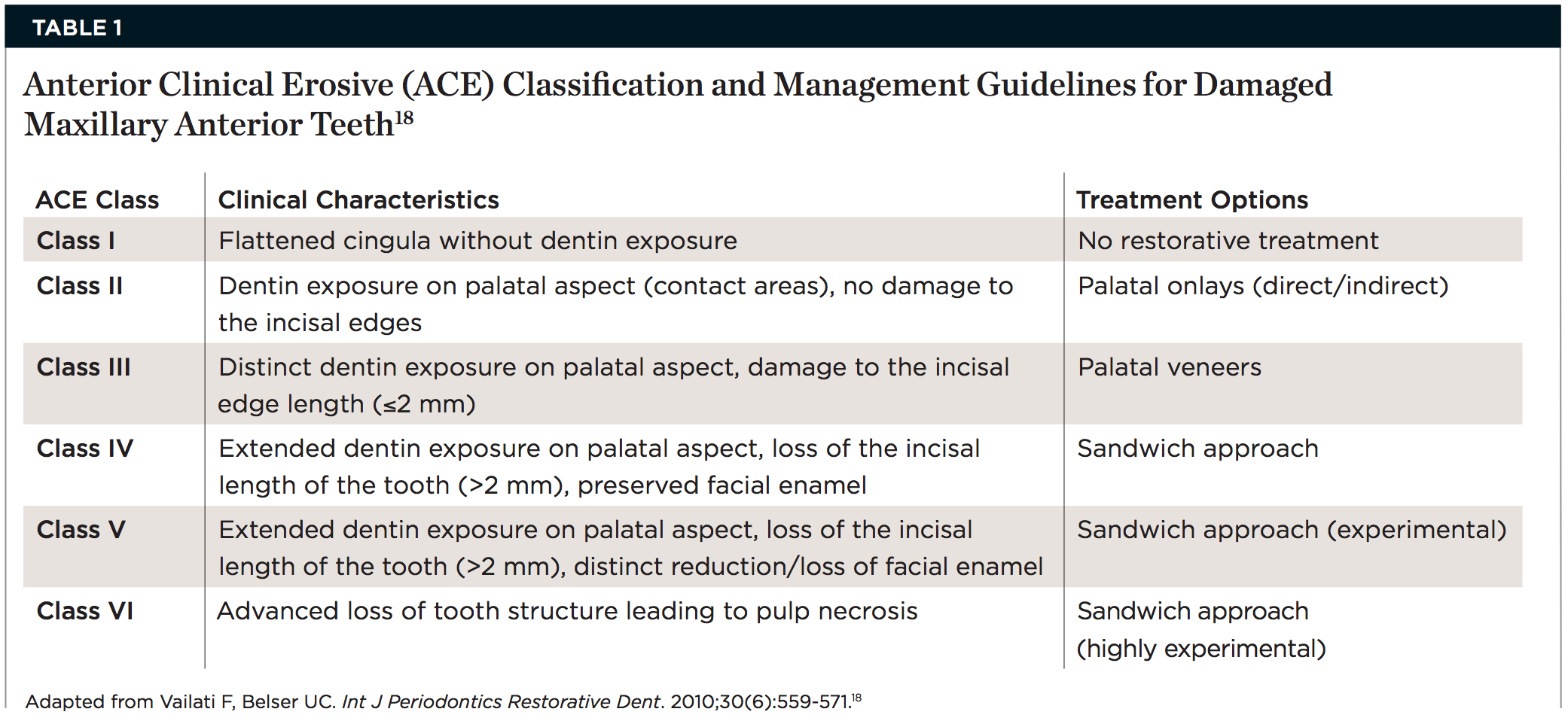
Table 1 presents the classification of damage to the anterior teeth in the upper jaw and their clinical manifestation. Below is a report on a holistic approach to restoring anterior teeth with palatal erosion.
Analysis of a clinical case and treatment sequence.
A 40-year-old patient complained of short teeth and asked for solutions to this problem. A clinical examination showed: the palatal surfaces of the anterior teeth in the upper jaw were destroyed, and the remaining parts of the tooth had a smooth and shiny surface. (Fig. 1 – Fig. 3).

Fig.1

Fig.2

Fig.3
In the centric occlusion position, there is no additional space between the teeth because the lower anterior teeth are in close contact with the upper teeth, which complicates the clinical situation. In most cases, according to traditional treatment protocols, such teeth are restored with crowns.
The difference between MIP and CR was identified using the Lucia fixture, which controlled the mandible in centric occlusion (Fig. 4). The maxillary model was mounted on a semi-adjustable articulator with a facebow and the mandibular model was mounted in centric relation. The articulator showed that when the condylar processes were in a position of central occlusion, there were no multiple contacts. By opening the central anchor on the articulator and allowing the teeth to return to their normal position, the authors found that there was insufficient space available to restore the anatomy of the palatal surfaces. Therefore, the decision was made to maintain the articular rests in centric relation in the articulator, which would create some space in the anterior region for restoration of the palatal surfaces.
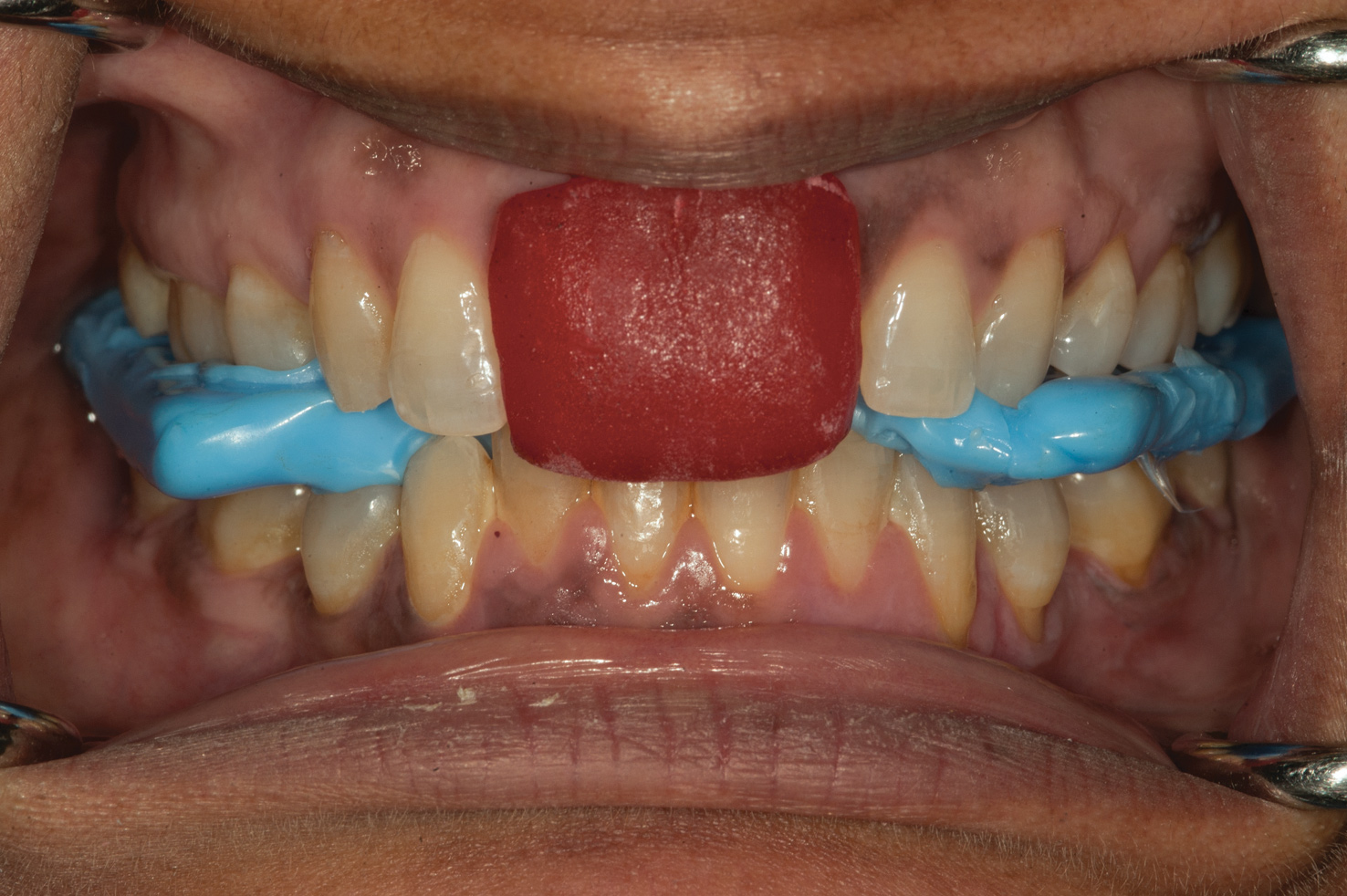
Fig.4
This space, obtained by correctly recording the centric occlusion, was used to prepare wax reproductions of future restorations (Fig. 5).
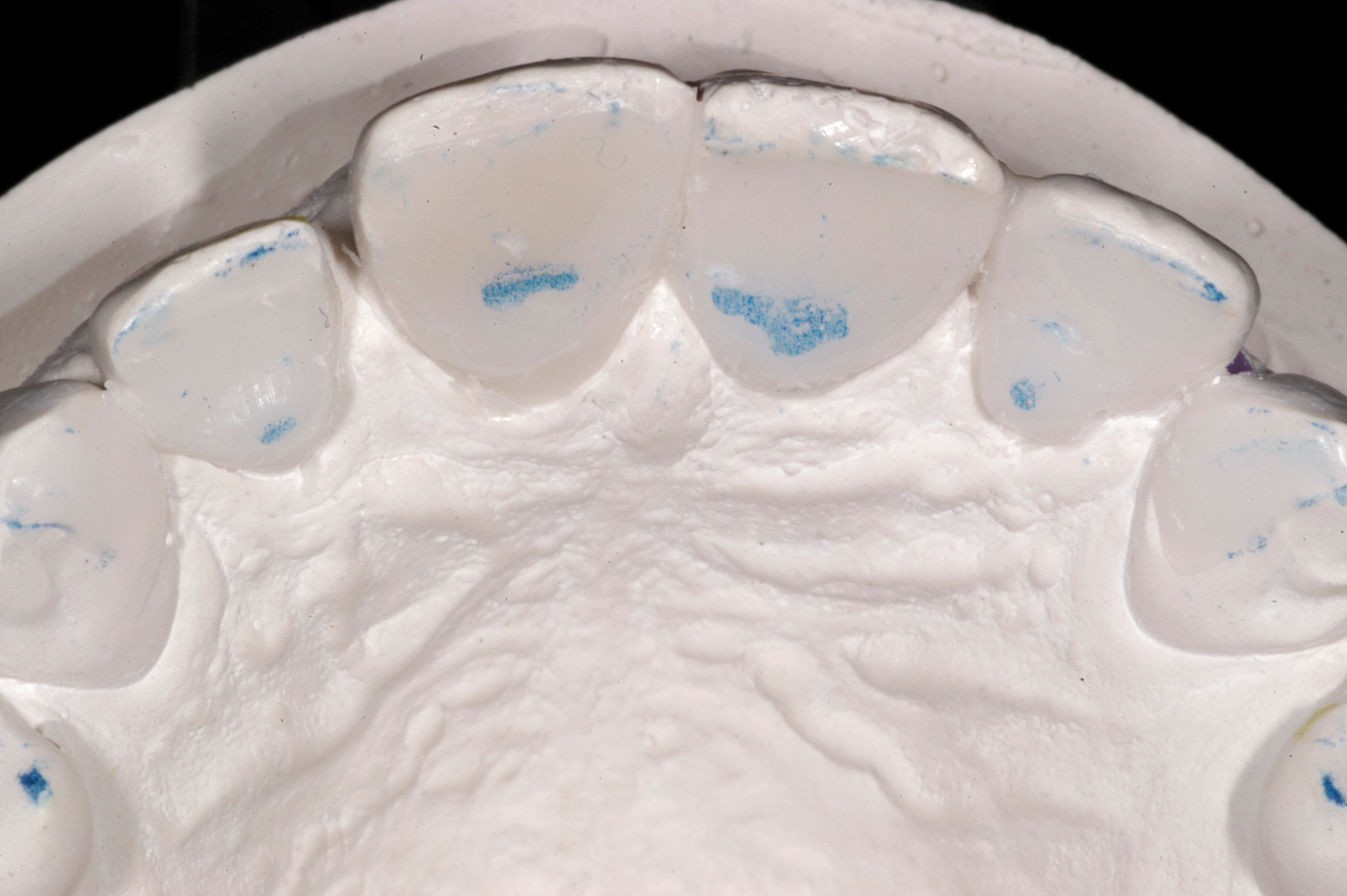
Fig.5
This opened the rear contacts by 1mm. This new maxillary-mandibular relationship was created intraorally and stabilized by restoring the palatal surfaces with composite veneers (Figure 6 and Figure 7).

Fig.6

Fig.7
The principles used here demonstrate the Dahl technique, which has been modified from its original version to suit the aesthetic needs of the patient when using an adhesive technique. The open contacts and interocclusal space created between the posterior teeth (Fig. 8) resulted in displacement after approximately 4 months. Once the movement was complete, occlusal equilibration was performed and bilateral multiple contacts were achieved between all posterior teeth. Then, using the matrix in a direct manner, wax reproductions of future veneers were made on the vestibular surface (Fig. 9). After the patient approved the proposed changes to the shape of the front tooth, minimal preparation was carried out to install veneers. (Fig. 10).

Fig.8

Fig.9

Fig.10
Monolithic lithium disilicate pressed veneers were then fabricated for the six maxillary anterior teeth. Staining was carried out to achieve polychromy and the required transparency. While layering the incisal edges will provide a superior esthetic result, it would require the incisal edges to be reduced to make room for the porcelain. To prevent tissue loss in a patient with minimal aesthetic needs, the authors chose an acceptable option for an already stained veneer that would provide a good aesthetic result. A few weeks later the veneers were installed. The final result photograph (Figure 11) demonstrated the patient's restored smile harmony and multiple occlusal contacts (Figure 12). The palatal surfaces were restored using a nanocomposite, which restored the chewing cycle (Fig. 13 and Fig. 14).

Fig.11

Fig.12

Fig.13

Fig.14
Step-by-step protocol for total rehabilitation for erosion and abrasion in the online course Total adhesive restorations - direct and indirect techniques .
https://cced.cdeworld.com/