
Identification and Characterization of a Previously Undiscovered Anatomical Structure in Maxillary Second Molars: The Palato-Mesiobuccal Canal
Abstract
Introduction This report aims to communicate the discovery of a novel anatomy in a three-rooted maxillary second molar, named as palato-mesiobuccal canal. Further details about endodontic treatment in different clinical cases are accessible for you to learn in our course "Endodontics 3.0".
Methods The tooth selected for this report was found incidentally as a result of a study on extracted maxillary molars that was being conducted for an unrelated purpose and involved hundreds of teeth. This three-rooted maxillary second molar was scanned using a micro-CT device set at a pixel size of 13.68 μm. The images were reconstructed with previously tested parameters resulting in the acquisition of 1655 axial cross-sections. Three-dimensional models of the internal and external anatomies were generated in STL format and were texturized to simulate the pulp tissue. The inner structure of the tooth was analyzed through the axial cross sections and the 3D volume was qualitatively evaluated.
Results The analysis of the 3D models revealed that the maxillary second molar under examination has 3 independent roots and 4 root canals. Each root contains 3 canals (mesiobuccal, distobuccal and palatal), while the fourth canal follows a unique path, originating in the coronal third of the palatal canal and proceeding in a buccal direction ultimately exiting through an independent foramen at the apex of the mesiobuccal root, near the mesiobuccal canal.
Conclusions This brief communication reports the discovery of a novel anatomy in a three-rooted maxillary second molar, named as palato-mesiobuccal canal, and provides important insights into the complexity of the root canal system in this group of teeth.
Introduction
The development of teeth is determined during the embryonic development by the interaction between the surface epithelium (ectoderm) and the mesenchyme derived from the neural crest(1). As odontogenesis initiates, the ectoderm-derived dental lamina folds inward to create the dental papilla, the source of the dental pulp. As the tooth continues to develop, the dental pulp and odontoblasts differentiate, producing dentin that forms the walls of the root canal space which, eventually, serves as a pathway for the nerves, blood vessels, and other tissues playing a critical role in maintaining the overall health and function of the tooth(2). Due to the intricate and unpredictable nature of root canal morphology, which is shaped by various factors such as genetics, tooth position, and environmental conditions, Guido Fischer(3) coined the term root canal system (RCS). Since then, extensive research has been conducted on the internal anatomy of teeth, leading to significant advancements in clinical practice and dental education. The insights gained from these studies have had a remarkable impact on both areas(4).
In maxillary second molars, the RCS typically consists of three or four canals. The fourth canal is often found in the mesiobuccal root and is commonly referred to as MB2. The internal morphology of this group of teeth has been studied by a considerable range of methods. In recent years, however, technological advancements in three-dimensional computed tomographic imaging have led to the development of more precise methods for evaluating tooth anatomy, such as micro-CT technology. Despite the advancements in technology that have provided a clearer understanding of tooth anatomy, no new configuration of the RCS has been reported in the literature since the classic publications from the early half of the 20th century(3,5-11).
Therefore, the aim of this brief report is to announce the discovery of a novel anatomy in a three-rooted maxillary second molar, named as palato-mesiobuccal canal.
Materials and methods
The tooth selected for this report was found incidentally as a result of a study on 300 extracted maxillary second molars that was being conducted for an unrelated purpose. This three-rooted maxillary second molar was scanned using a micro-CT device (SkyScan 1172; Bruker-microCT, Kontich, Belgium). The scan parameters were set at 100 kV, 100 μA, a pixel size of 13.68 μm, 360º rotation with 0.3º steps, and an aluminum-copper alloy filter. The images were reconstructed using NRecon v.1.7.4.6 software (Bruker-microCT) with a 50% beam hardening correction, ring artifact correction of 7, and smoothing of 5. This resulted in the acquisition of 1655 axial cross-sections. Three-dimensional models of the internal and external anatomies were generated in STL format using CTAn v. 1.20.8.0 (Bruker-microCT) and were texturized to simulate the pulp tissue using Blender v.3.3.1 software (Blender Foundation; Amsterdam, Netherlands). The inner structure of the tooth was analyzed through the axial cross sections using DataViewer v. 1.5.6.2 (Bruker-microCT), and the 3D volume was qualitatively evaluated with CTVol v.2.3.2.0 (Bruker-microCT) and CTVox v.3.3.1 (Bruker-microCT).
Results
The analysis of the 3D models revealed that the maxillary second molar under examination has 3 independent roots and 4 root canals. Each root contains 3 canals (mesiobuccal, distobuccal and palatal), while the fourth canal follows a unique path, originating in the coronal third of the palatal canal and proceeding in a buccal direction ultimately exiting through an independent foramen at the apex of the mesiobuccal root, near the mesiobuccal canal (Figures 1 and 2).
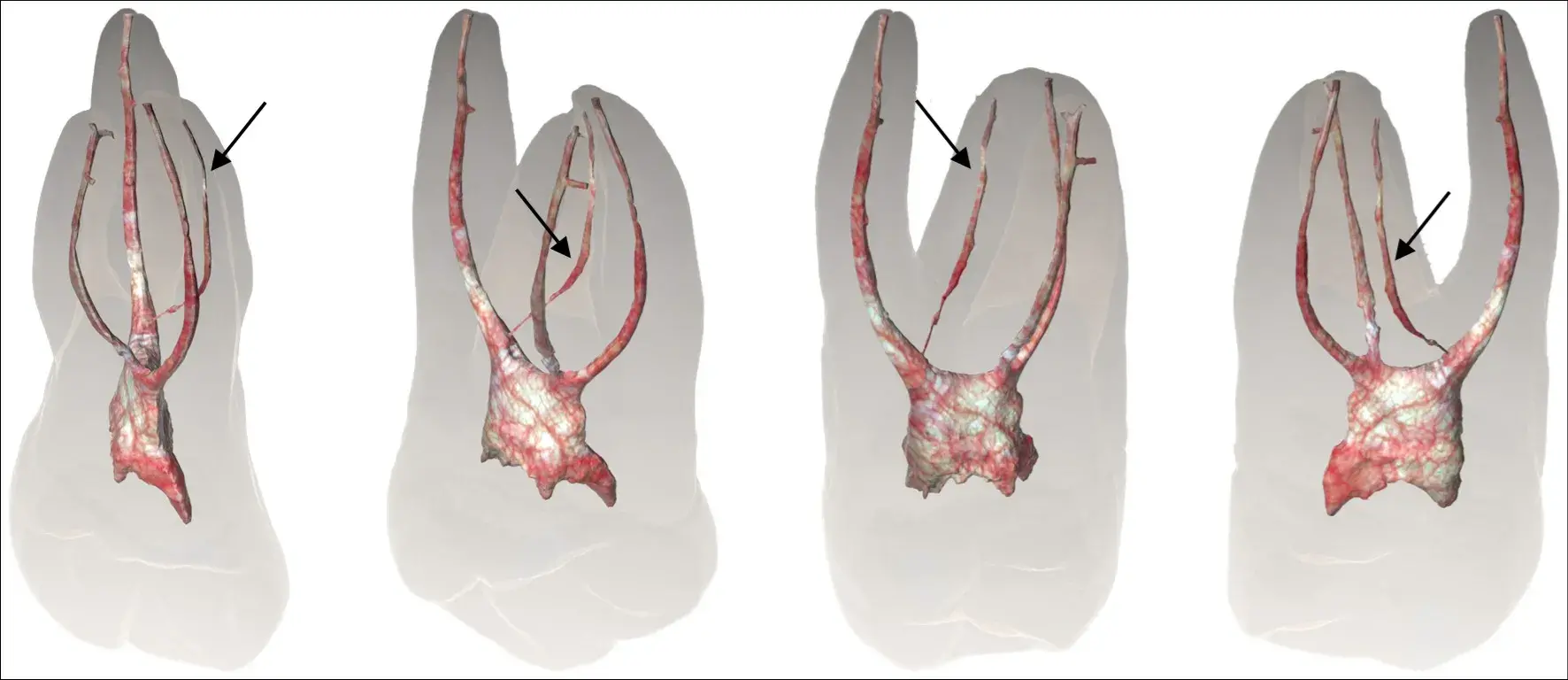 Figure 1 Frontal and lateral views of 3D models of root and root canals of a maxillary second molar depicting the existence of the palato-mesiobuccal canal (arrows).
Figure 1 Frontal and lateral views of 3D models of root and root canals of a maxillary second molar depicting the existence of the palato-mesiobuccal canal (arrows).
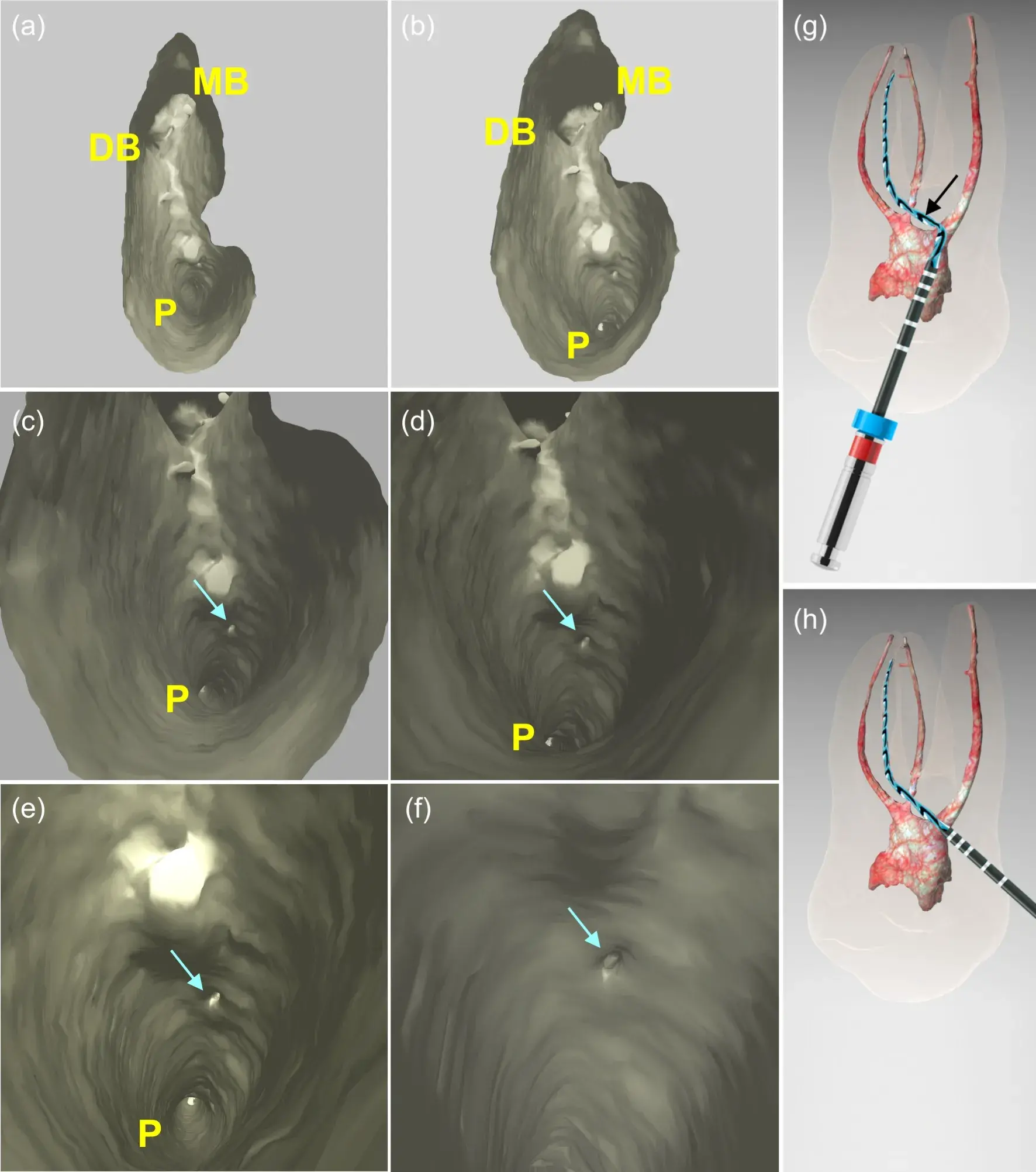 Figure 2 (a-b) Overview of the pulp chamber floor of a maxillary second molar showing the presence of mesiobuccal (MB), distobuccal (DB), and palatal (P) canals; (c-f) High-magnification images of the pulp chamber highlighting the palatal canal and the orifice entrance of the newly discovered palato-mesiobuccal canal (indicated by arrows) located in the coronal third of the palatal canal; (g) A virtual representation of a heat-treated instrument simulating the path it should follow to reach the foramen of the palato-mesiobuccal canal through a conventional access cavity preparation; (h) A virtual representation of a heat-treated instrument simulating the path it should follow to reach the foramen of the palato-mesiobuccal canal through a palatal access cavity preparation performed utilizing a guide rail concept
Figure 2 (a-b) Overview of the pulp chamber floor of a maxillary second molar showing the presence of mesiobuccal (MB), distobuccal (DB), and palatal (P) canals; (c-f) High-magnification images of the pulp chamber highlighting the palatal canal and the orifice entrance of the newly discovered palato-mesiobuccal canal (indicated by arrows) located in the coronal third of the palatal canal; (g) A virtual representation of a heat-treated instrument simulating the path it should follow to reach the foramen of the palato-mesiobuccal canal through a conventional access cavity preparation; (h) A virtual representation of a heat-treated instrument simulating the path it should follow to reach the foramen of the palato-mesiobuccal canal through a palatal access cavity preparation performed utilizing a guide rail concept
Discussion
The systematic study of the root canal system in different groups of teeth began in the late 19th century, with seminal works from Eduard Mühlreiter(12), Adolph Witzel(13), and Greene Vardiman Black(14), followed by Gustav Preiswerk(5) and Guido Fischer(3). With technological advancements, a wide array of techniques have been developed and used to visualize the anatomy of human teeth, leading to a wealth of publications on the subject. Given the extensive research and global contributions, it seemed unlikely that a new discovery in the anatomy of the root canal system would be made, as reported in this brief communication. After conducting a thorough examination of 300 maxillary second molars to identify specific anatomical features for another study, we made a remarkable discovery: a previously unknown anatomical structure in a maxillary second molar, which we named the palato-mesiobuccal (PMB) canal. This finding has profound implications for our comprehension of the complexity of the RCS in this group of teeth and could have a major impact on clinical practice.
To further study this newly discovered canal, we used the gold standard high-resolution non-destructive micro-CT technology to examine the internal anatomy of the tooth in detail. Our images revealed that the PMB canal is a continuous structure, extending from the buccal aspect of the coronal third of the palatal canal to the apical third of the mesiobuccal root (Figure 1, Figure 2a-f). The presence of this canal may pose a challenge to endodontic therapy as it may harbor infected or inflamed tissue. The unique position of the PMB canal in maxillary second molars can present a challenge for proper shaping using current techniques, as shown in Figure 2g. In such cases, an alternative approach for locating the orifice and preparing the PMB canal may be a palatal access cavity, utilizing a guide rail concept based on cone-beam tomography scans15 (Figure 2h). However, in case of treatment failure, apical surgery at the mesiobuccal root may be necessary.
The authors of this communication were concerned that the existence of the PMB canal may have already been reported in previous studies. To ensure the originality of our findings, we conducted a comprehensive literature search and reached out to renowned authors and experienced clinicians globally with images and videos. However, as we expected, based on our extensive experience in this field, no similar reports were discovered in our literature search and consultations with experts. On the other hand, we noted similarities between the PMB canal and another anatomical variation observed in some maxillary second molars mostly with fused roots, making it important to differentiate them. As previously reported, the occurrence of fused roots in maxillary second molars is often linked to a complex root canal system that includes isthmuses, apical ramifications, and a frequent occurrence of C-shaped configurations(16,17). In certain cases, the orifice of the fourth canal may become displaced close to the palatal canal, leading to confusion with the PMB canal (Figure 3). However, it is important to note that this canal is actually the MB2 and not the PMB canal, as it does not originate from within the palatal canal.
Incidental findings such as the one reported herein can sometimes have important clinical implications, and they may require further investigation or follow-up to determine their significance and appropriate management. So, further research is needed to fully understand the implications of this new anatomical structure, including its prevalence and potential clinical significance. We believe that this discovery represents an important achievement in our understanding of the anatomy of maxillary second molars and we encourage our colleagues in the dental community to consider the implications of this finding in their own clinical practice.
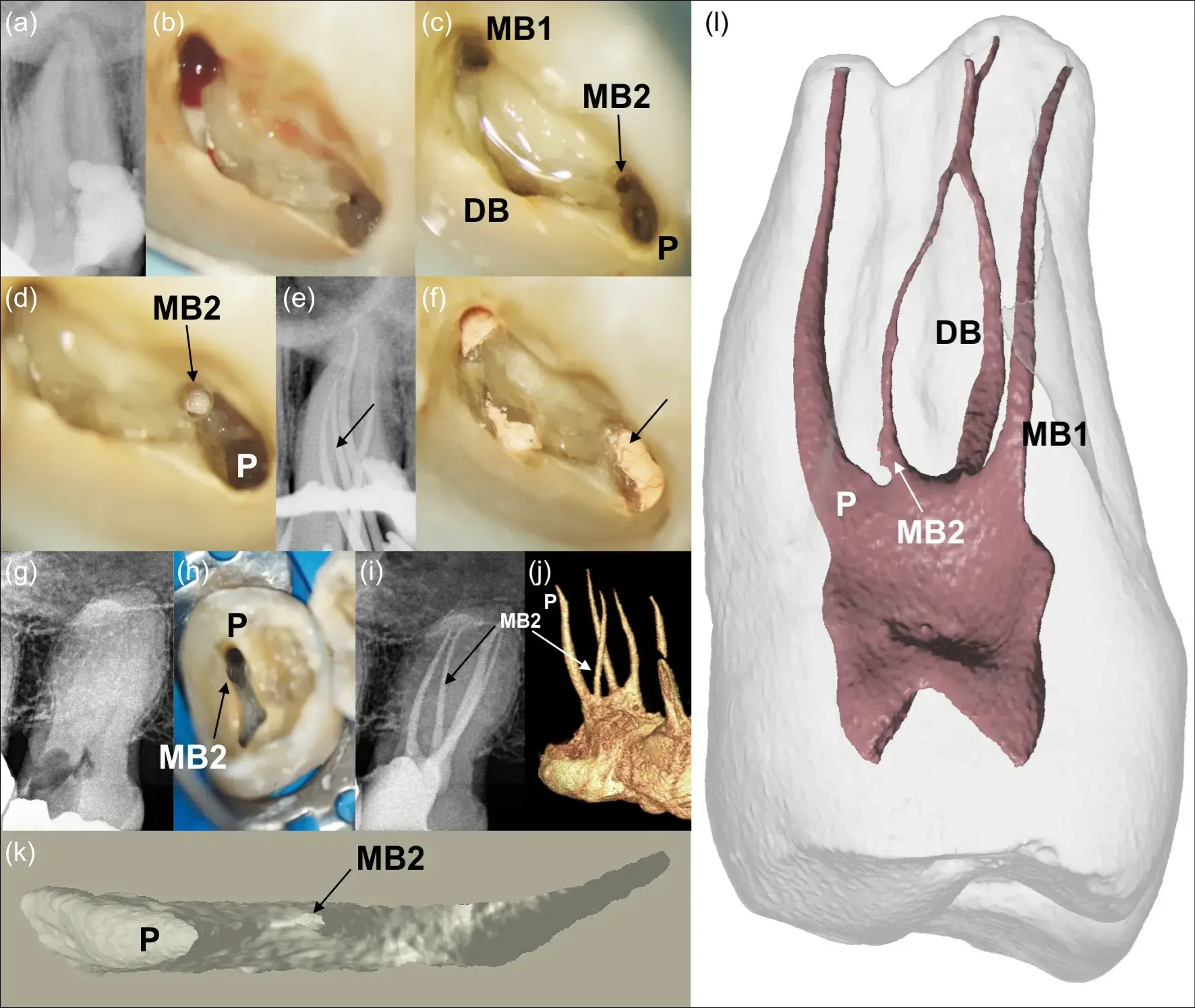 Figure 3 (a-j) Clinical cases showing 2 maxillary left second molars with root fusion Type II (mesiobuccal and palatal roots) in which the orifice entrance of the mesiobuccal canal (MB2) can be seen in close proximity to the palatal canal (indicated by arrows). (k-l) micro-CT images of a maxillary second molar with fused roots showing the orifice of the MB2 canal closed to the palatal canal. Images (a-f) are courtesy of Dr. Roberto Cristescu, while images (g-h) are courtesy of Dr. Viviany Bertollo (MB1 and MB2: 1st and 2nd canal of the mesiobuccal root, respectively; DB: distobuccal canal; P: palatal canal).
Figure 3 (a-j) Clinical cases showing 2 maxillary left second molars with root fusion Type II (mesiobuccal and palatal roots) in which the orifice entrance of the mesiobuccal canal (MB2) can be seen in close proximity to the palatal canal (indicated by arrows). (k-l) micro-CT images of a maxillary second molar with fused roots showing the orifice of the MB2 canal closed to the palatal canal. Images (a-f) are courtesy of Dr. Roberto Cristescu, while images (g-h) are courtesy of Dr. Viviany Bertollo (MB1 and MB2: 1st and 2nd canal of the mesiobuccal root, respectively; DB: distobuccal canal; P: palatal canal).
Conclusion
This brief communication reports the discovery of a novel anatomy in a three-rooted maxillary second molar, named as palato-mesiobuccal canal. This new configuration provides important insights into the complexity of the RCS in this group of teeth and underscores the need for continuous research and advancements in the field.
If you enjoyed reading this article and would like to explore MB2 canal treatment further, we encourage you to enroll our course "Complex cases in Endodontics. Original program created by Michael Solomonov".
List of authors:
Marco A. Versiani, Tamer Taşdemir, Ali Keleş
References
Balic A, Thesleff I. Tissue interactions regulating tooth development and renewal. Curr Top Dev Biol. 2015;115:157-186.
Nanci A. Ten Cate's oral histology : development, structure, and function. 9th ed. St. Louis, Mo.: Elsevier; 2017.
Fischer G. Über die feinere Anatomie der Wurzelkanäle Menschlicher Zähne. Deutsche Monatschrift fur Zahnheilkunde. 1907;25:544-553.
Versiani MA, Basrani B, Sousa-Neto MD. The root canal anatomy in permanent dentition. 1st edition. ed. Switzerland: Springer International Publishing; 2018.
Preiswerk G. Leherbuch und Atlas der Zahnheilkunde mit Einschluβ der Mund-Krankheiten. Munich: J. F. Lehmann; 1903.
Adloff P. Das Durchsichtigmachen von Zähnen und unsere Wurzelfüllungsmethoden. Deutsch Mschr Zahnheilk. 1913;31:445.
Fasoli, Arlotta. Sull'anatomia dei canali radicolari dei denti umani. Giugno: Stomatologia; 1913.
Moral H. Ueber das Vorkommen eines vierten Kanals in oberen Molaren. ÖstUng Vschr Zahnheilk. 1915;33:313-325.
Zürcher E. Zur Anatomie der Wurzelkanale des menschliches Milchgebisses und der 6 Jahr-Molaren. Zurich; ; 1922.
Hess W, Zürcher E. The anatomy of the root canals of the teeth of the permanent and deciduous dentitions. London: John Bale, Sons & Danielsson, Ltd.; 1925.
Okumura T. Anatomy of the root canals. J Am Dent Assoc. 1927;14:632-636.
Mühlreiter E. Anatomie des menschlichen Gebisses von med. Th. E. de Jonge Cohen. Leipzig: Arthur Felix; 1870.
Witzel A. Compendium der pathologie und therapie der pulpakrankheiten des zahnes. Hagen: Risel & Co.; 1886.
Black GV. Descriptive anatomy of the human teeth. Philadelphia: The Wilmington Dental Manufacturing Co.; 1890.
Zehnder MS, Connert T, Weiger R, Krastl G, Kühl S. Guided endodontics: accuracy of a novel method for guided access cavity preparation and root canal location. Int Endod J. 2016;49:966-972.
Keskin C, Keleş A, Versiani MA. Mesiobuccal and palatal interorifice distance may predict the presence of the second mesiobuccal canal in maxillary second molars with fused roots. J Endod. 2021;47:585-591. Ordinola-Zapata R, Martins JN, Bramante CM, Villas-Boas MH, Duarte MH, Versiani MA. Morphological evaluation of maxillary second molars with fused roots: a micro-CT study. Int Endod J. 2017;50:1192-1200.