
Effects of Papacarie on children with dental caries in primary teeth: a systematic review and meta-analysis
Background. Caries in primary teeth hinder the child to bite and chew and influence their development. Papacarie has the characteristics of selective removal of decayed tissue and can preserve healthy dentine to the maximum, but its efficiency has not been critically evaluated compared to conventional method.
Aim. This review is aiming at comparing the Papacarie and traditional method in caries removal in primary dental caries with children.
Design. Comprehensive literature searching at PubMed, Embase, Cochrane Central Register of Controlled Trials, and Web of Science to January 2018.
Results. Six randomized controlled trials (RCTs) and four prospective controlled clinical trials (CCTs) were included. The microbiota in caries dentine was significantly reduced using the Papacarie treatment (MD = 0.57, 95% CI 0.04 to 1.09, P = 0.03), and the anxiety feeling declined more in the Papacarie group (MD = 1.01, 95% CI 1.72 to 0.30, P < 0.005). There was a greater 200.79 (MD = 200.79, 95%CI 152.50 to 249.09, P < 0.00001) increase in time taken for the Papacarie treatment compared with the conventional method.
Conclusion. Papacarie exerts a positive effect in reducing the bacteria and decreases the pain during caries removal in primary teeth although it costed a longer treatment time compared with the conventional method.
Introduction
Dental caries are among the most general dental diseases among children, as a result of the consumption of too much candied food, carbonated drinks, and lack of regular oral examination. Dental caries usually destruct and dissolve the tooth tissues locally and may lead to the pulpitis and periapical periodontitis, and eventually result in teeth missing when left untreated, which causes patients to have pain and discomfort. Because the enamel on primary teeth is less calcified and more fragile, primary teeth are more subject to lesion formation and progression than are permanent teeth. Primary teeth, however, helps to develop a proper occlusion in young children, because primary teeth maintain a particular space and served as space retainers for the permanent teeth, and healthy primary teeth are significant in helping children to bite and chew, speak clearly, and promote self-confidence. Hence, caries removal and restoration (fillings) for the primary teeth are a necessary option for the management of oral health in children.
Conventional caries removal method usually means digging and drilling by rotation handpiece to remove the decayed tissue, which is efficient in removing the bacterial dentine but is perceived as uncomfortable, uneasy, and painful by children. Because conventional caries removal method may extend into the sound dentin in the inner, thereby it is therefore to open more dentinal tubules. This effect is usually prone to bringing pain and tension. And the use of local anaesthesia is necessary during treatment.
Currently, painless treatment and minimal intervention are basic principles in paediatric dentistry. The treatment principles of dental caries were transformed by the advances of the physiology and the progress in minimally invasive treatment. The most conspicuous changes contain the selective removal of bacterial dentine and preservation of sound dentine to the maximum. Alternative techniques, such as lasers, air abrasion, ultrasonic technique, and Chemomechanical approaches for caries removal, have been developed. Among these methods, most of them except Chemomechanical approaches are costly and may lead to the hypersensitivity of teeth and therefore infrequently used. In addition, these methods cause pressure on the pulp and deleterious thermal, which contribute to pain and anxiety especially in children. Therefore, the Chemomechanical method is one of the most documented alternative to conventional drilling method. Further details about dental caries in primary teeth treatment are accessible for you to learn in our course "What's new in pediatric dentistry".
Recently, in 2003, Papacarie was released as a proteolytic gel. The collagen degradation features of papain and the bactericide characteristics of chloramines were added to the new medicine. Papain makes the carious dentine softer through the interaction with exposed collagen and then dissolute the decayed tissues, which allows the removal of carious dentine without local anaesthesia and drilling. Flindt demonstrated that papain’s function limited in bacterial tissues because infected tissues lack a plasmatic anti protease, known as anti-trypsin (AI), this is only present in healthy dentine and it inhibits tooth structure destroyed. Dawkins et al. reported that papain can inhibit the growth of Grampositive and Gram-negative organisms. This technique involves the selective removal of degraded collagen fibrils in carious dentin lesions, while preserving the affected demineralized dentine layer. Adopting the Papacarie method in caries removal, clinicians can remove all of the caries dentine and protect the sound dentine without a special instrument. Most children are satisfied with this method, according to research on their preference research of the conventional method and Papacarie. Several investigators, however, have noted the efficacy of Papacarie is questionable, and it may increase the treatment time. This inconclusive evidence is not advantageous for clinical application and the promotion of Papacarie for caries removal in primary teeth among children.
Therefore, a scientific systematic review and meta-analysis are necessary to evaluate the effectiveness and efficient of Papacarie31 in caries removal in primary teeth in children. The evidence-based systematic review and metaanalysis aim to determine whether the application of Papacarie could influence the outcomes of caries removal with primary teeth in children. Specifically, we focus on these outcome variables as follows: including a microbiological assessment before and after caries removal and the influence on child behaviour, pain perception, length of time needed, and preference of the treatment method by children.
Method
This systematic review was performed referring to the guidelines of the PRISMA statement for reporting systematic reviews.
Focused question
According to the PICO framework: ‘Is the efficiency and efficacy of Papacarie in primary dental caries with children better when compared to conventional drilling method (controls)?’
Literature search
We conducted a comprehensive search in PubMed, Embase, Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, Ovid, Google Scholar, and Web of science up to 20 January 2018. The following key words were used in literature searches: ‘primary teeth’, ‘caries’, ‘Papacarie’, ‘Chemomechanical Caries Removal’, and ‘Chemomechanical Caries Excavation’. The language or date of publication was not limited and searched the reference lists of all researches for additional studies. Where additional data and figure for some literature were needed, we contacted the related authors.
Inclusion criteria (PICO question: population, intervention, comparison, outcome). Type of participants— Adolescent and child patients with primary molar caries. Only human studies were included without gender restriction. Children without intelligence problem or without receiving sedatives before treatment or any related agents for procedural sedation will be included in this study.
Type of interventions—Patients undergoing Chemomechanical caries removal (Papacarie) or conventional caries removal method in the primary molar teeth.
Types of outcome measures—Microbiological assessment before and after the caries removal, influence on child behaviour, pain perception, length of time needed, and preference of treatment method by children were recorded separately for both the methods.
Trial design—RCTs and prospective CCTs were reviewed, included, and analysed accordingly.
Exclusion criteria
The following types of studies were excluded: (i) restorative treatment; (ii) studies involving teeth with enamel hypoplasia and other structure defects; (iii) studies lack the mean value and standard deviation (SD) of outcomes including time needed to take, pain scale, microbiota reducing before and after caries removal; (iv)When children have presence of spontaneous pain, use of antibiotics within 2 weeks prior to study, teeth with pulpal involvement, furcation or periapical pathology and/or interproximal caries and presence of any systemic disease;(v)studies that conducted in permanent teeth.
Data extraction
The titles, author, and A. A. (date) of retrieved articles were imported into Endnote X7. Then, two reviewers (* and *) invested independently to evaluate the eligibility of the studies. Any dissents were resolved by conversation. In addition, a third author (*) was consulted if needed.
We choose publications according to the inclusion criteria and exclusion criteria. Then, we get full texts for all eligible studies. Data are extracted as follows: (i) author and publication year; (ii) study type; (iii) characteristics of participants: sample size, age, location, group, and overall health conditions; (iv) caries type, moisture control, criteria of caries removal, scale type of pain, outcome variables, and authors’conclusions, among others.
Quality assessment
The Cochrane Handbook on Risks of bias was adopted to evaluate the quality of the eligible studies independently by two reviewers (* and *). For each study, in brief, the selectionbias, performance bias, detection bias, attrition bias, reporting bias, and other bias are assessed. The classification of the parameters was adequate, unclear, or inadequate. A study was evaluated as ‘low risk of bias’ if all the domains were judged as ‘low risk’, ‘moderate risk of bias’ if any of the domains was judged as ‘unclear risk’, and ‘high risk of bias’ if any domain was judged as ‘high risk’. All these data were assessed by two reviewers (* and *), and dissents were settled by discussion or consultation with a third author (*). The decisions on study identification were recorded.
Data analysis
The multiple studies were combined by the weighted mean difference (WMD), standard deviation (SD), and its 95% confidence intervals (CIs) of the outcome variable (the CFU of bacteria, scores of pain scale, and treatment time) were assessed. We analyse the extracted data using Review Manager 5.3. Statistical heterogeneity was explored using the chisquare test with a 10% level of significance as the cut-off value. I2 statistic was used to quantify the impact of statistical heterogeneity. And a 95% confidence interval (CI) of I2 is reported in addition to the point estimate I2. If I2 > 50% (P ≤ 0.10), which means a high heterogeneity. Then, the heterogeneity needs to be explained, a random-effect model was used, otherwise, the fixed-effect model would be chosen. The hypothesis of homogeneity was set invalid for P < 0.05 (2-tailed z tests). If the data were unable to be pooled, they were described.
Results
Studies selection results
In total,203 articles are identified through databases and hand search. A total of 188 studies were removed because they do not meet the inclusion criteria. Fifteen articles with adequately designed and particular treatment method are involved in the qualitative synthesis. Three of the studies are excluded for the deficiency of mean and SD data, and three of them reported the same experiment. Finally, six RCTs and four CCTs are involved in the quantitative synthesis. The flow diagram of study selection is displayed in Fig. 1.
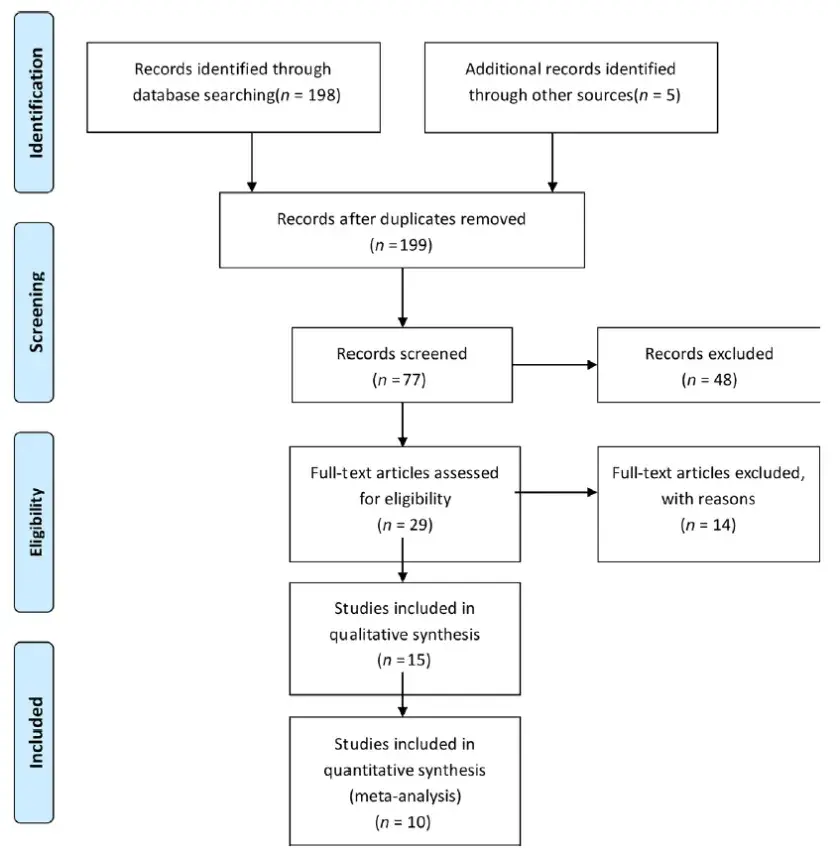 Fig. 1. PRISMA diagram to show the process of study selection.
Fig. 1. PRISMA diagram to show the process of study selection.
Studies features
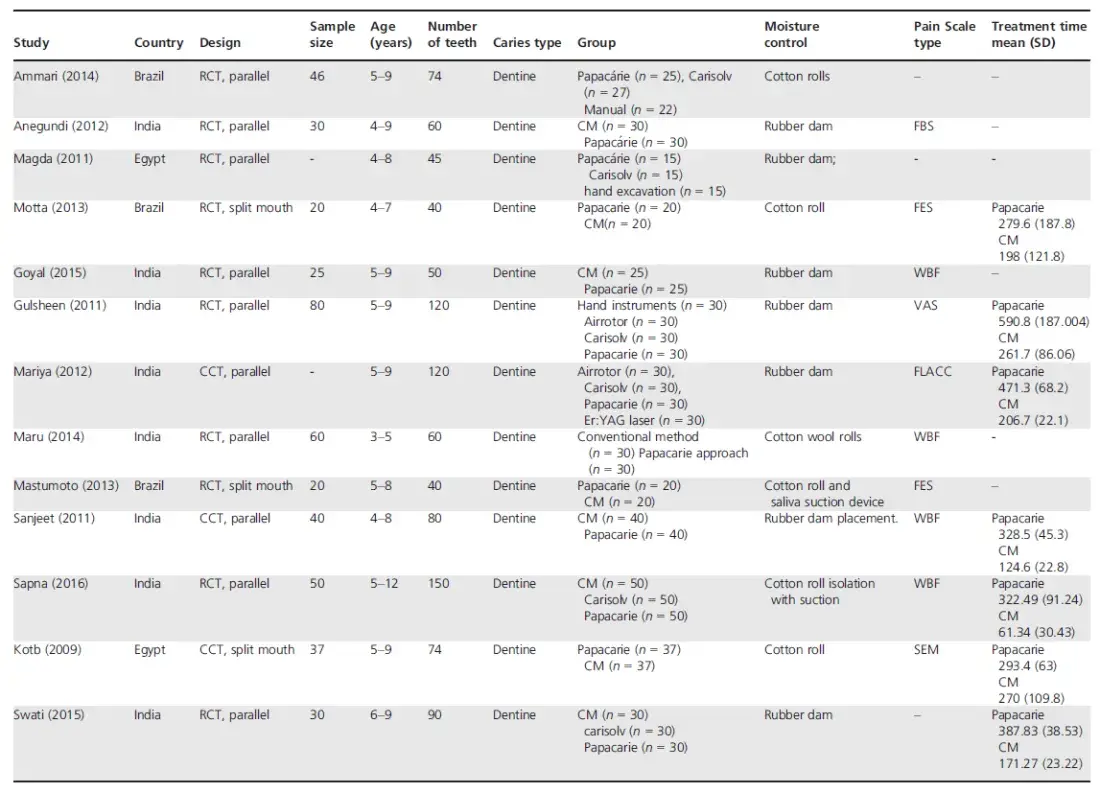
The trials’ publication date was from 2009 to 2016. Among these trials, three articles reported the same experiment; therefore, they were combined as Motta 2013–2014. Different regimens of the Papacarie method were identified in the included articles. The type, generation, and dose of the medicine are different. Among the included studies, five trials discussed the change in bacteria in the caries lesion, and two6 trials were excluded in the meta-analysis for a lack of mean and SD data. In addition, 10 trials assessed the outcomes of pain perception before and after different caries removal methods; nevertheless, the scales used in these trials differ considerably. Only three trials used the Wong-Baker-Face Pain Scale (WBF) to evaluate pain perception and were remained eligible. And seven trials with complete mean and SD data of timeconsumption were included in the meta-analysis. Table 1 shows the summary of the features of included studies.
Table 1. Characteristics of the included studies (n = 13).
 Risk of bias
Risk of bias
A review of the judgement of the authors concerning each risk bias item is presented in Fig. 2, and the assessments of each study’s risk of bias are listed in Fig. 3. Nine of them had a low risk of bias, and the other five studies had a moderate risk of bias. Among the eligible researches, three of them did not make a clear description of the enrolment. As blinding of operators was impossible because operators were clear regarding the treatment type during the treatment, the evaluation of blinding here referred to the data analysers. To avoid detection bias, all the outcome variables were previously calibrated. The other two studies did not notice the blinding of outcome assessment.
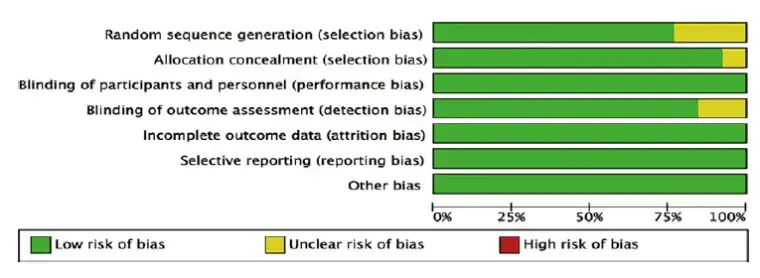 Fig. 2. Risk of bias graph. Review authors’ judgements about each risk of bias item presented as percentages across all included studies. Red, yellow, and green refer to high risk of bias, unclear risk of bias, and high risk of bias.
Fig. 2. Risk of bias graph. Review authors’ judgements about each risk of bias item presented as percentages across all included studies. Red, yellow, and green refer to high risk of bias, unclear risk of bias, and high risk of bias.
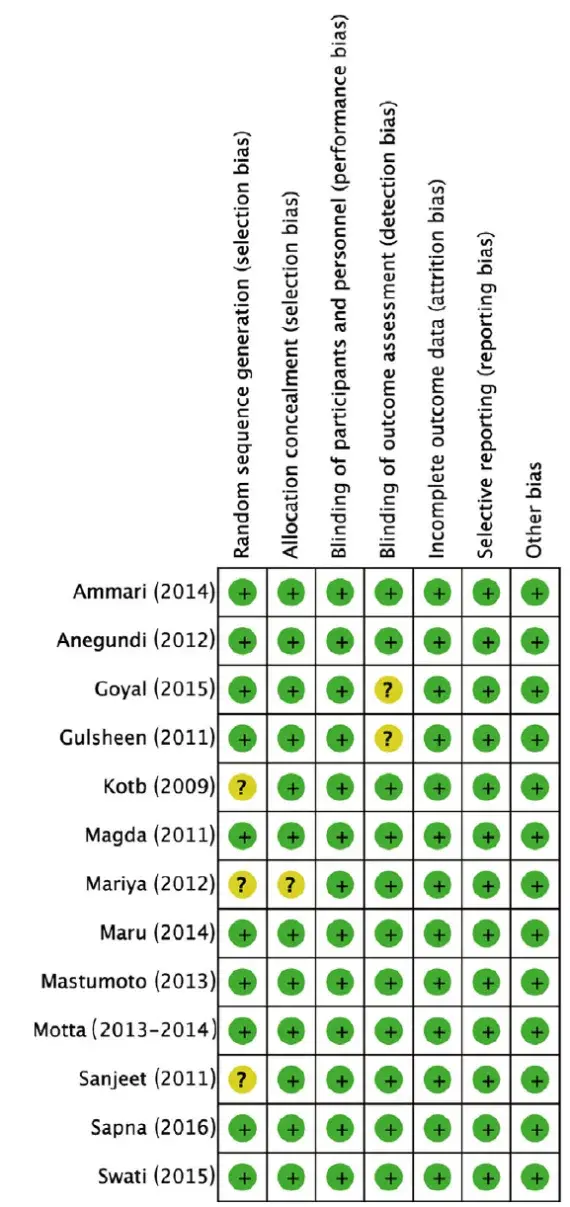 Fig. 3. Risk of bias graph: the review authors’ judgements about each risk of bias item for each included study. Green, yellow, and red refer to low risk of bias, unclear risk of bias, and high risk of bias, respectively.
Fig. 3. Risk of bias graph: the review authors’ judgements about each risk of bias item for each included study. Green, yellow, and red refer to low risk of bias, unclear risk of bias, and high risk of bias, respectively.
Efficacy of Papacarie treatment in reducing the cariogenic microbiota
Five trials reported the outcome for reducing bacteria. Three of these have a data deficiency or differed in the bacteria measurement method. As a result, these trials are excluded in the meta-analysis. Two studies with a detailed mean and SD data of log10 colony forming units (CFUs) were adopted to be used for a meta-analysis and the forest plot was demonstrated in Fig. 4. In sum, 90 patients contributed to this outcome. It was observed that the microbiota in caries dentine was significantly reduced using the Papacarie treatment (MD = 0.57, 95% CI 0.04 to 1.09, P = 0.03), compared with the conventional drilling method, with low heterogeneity detected (v2 = 2.00, P = 0.37, I2 = 0%, 95% CI 0%–98%).
 Fig. 4. Forest plot from the fixed-effect meta-analysis evaluating the difference in bacterial before and after caries removal treatment.
Fig. 4. Forest plot from the fixed-effect meta-analysis evaluating the difference in bacterial before and after caries removal treatment.
Pain perception
Ten studies discussed the pain perception when caries in the primary teeth were treated. Means and SD data of Wong-Baker-FACES (WBF) scores, however, were provided by three studies for meta-analysis. The forest plots were displayed in Fig. 5. Although WBF score is a subjective measurement, it is the relatively easy and convenient way to record the feeling of child patients when they had been treated.
It was observed that pain scores evaluated before and after caries removal were reduced in both the Papacarie and conventional method. Because I2 = 86% (95%CI 60%–95%) showed high degrees of heterogeneity between studies, a random-effect model was adopted. When comparing the two groups, the anxiety feeling declined more in the Papacarie group (MD = 1.01, 95% CI 1.72 to 0.30, P < 0.005).
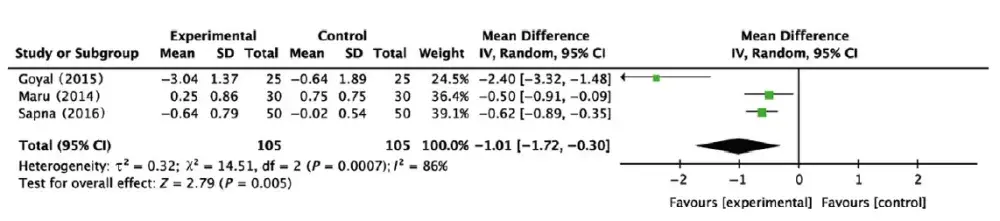 Fig. 5. Forest plot from random effects meta-analysis for the comparison of Wong-Baker-FACES (WBF) scores in conventional method and Papacarie treatment.
Fig. 5. Forest plot from random effects meta-analysis for the comparison of Wong-Baker-FACES (WBF) scores in conventional method and Papacarie treatment.
Time taken for caries removal
Eight researches demonstrated the outcomes of the treatment time. Nevertheless, only seven were eligible for the meta-analysis. The forest plot was described in Fig. 6. There was a greater, that is, 200.79 (MD = 200.79, 95% CI 152.50 to 249.09, P < 0.00001) increase in time taken for the Papacarie treatment compared with the conventional method. The results of the time taken had a high heterogeneity (v2 = 128.89, P < 0.00001, I2 = 95%, 95%CI 93%–97%). Maybe the different studies lack of consistency regarding the measurement and analysis of the time. Therefore, we chose random effects model to describe the outcomes.
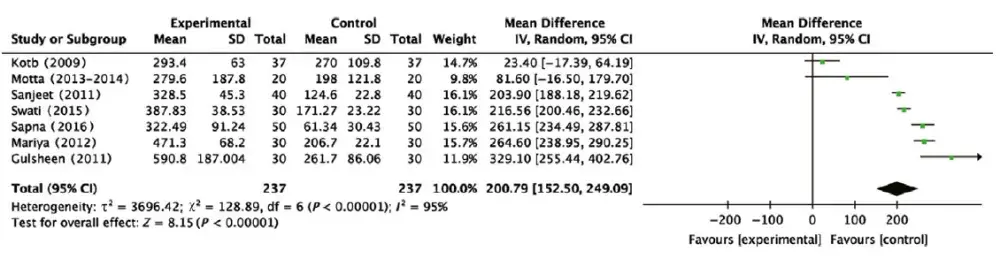 Fig. 6. Forest plot from the fixed-effect meta-analysis evaluating the difference in time taken of caries removal.
Fig. 6. Forest plot from the fixed-effect meta-analysis evaluating the difference in time taken of caries removal.
Patient acceptability
The preference of the different caries removal method was evaluated in three studies. Anegundi recorded the preference of the conventional method and Papacarie, in which the Papacarie group had a higher proportions of 60% compared with 36.7% for the conventional method. In Goyal’s study, a majority (80%) of the children in the study preferred the Papacarie method. In addition, Swait compared the conventional method, Carisolv and Papacarie for patient acceptability through a visual analogue scale (VAS). In their study, the patient acceptance rate was observed to be higher with Papacarie method. These results can be explained by the fact that less pain and anxiety were experienced in patients with the Papacarie method. This finding is in accordance with the results of pain perception scaled by Wong-Baker-FACES (WBF) scale.
Follow-up
According to all of the included studies, only two studies reported the long-term follow-up of the Papacarie method. One study recorded the retention of the filling material and the incidence of secondary caries 1 month later, and the use of a different caries removal method was analysed. In addition, the restoration was predominantly present and without defects following both procedures. In the other study, the participants received regular clinical follow-up of the caries treatment. The density of the remaining dentin was assessed through radiographic examination. The record time includes immediately after the caries removal treatment and one (T1), six (T2), and 18 (T3) months later. In both groups, the mean radiographic density was improved after treatment in different evaluation times, and no secondary decay was observed in the two groups.
Discussion
Painless dentistry and minimal intervention providing comfort, relief, solace, and instillationof a positive attitude towards dental health care are among the factors justifying the specialty of paediatric dentistry. A gentle and painless treatment experience may affect the patients’ whole life of oral health. Because many of the school-age children are afraid of the dentist, they may consequently avoid dental care. This negative behaviour is often linked to early traumatic experiences and negative attitudes in the patient’s family. Consequently, fearful dental patients often do not receive optional and regular dental care. Thus, minimal invasive caries removal treatment is of great importance in dental care for children. In addition, the concept of preserving sound dentine in the Chemomechanical caries removal (CMCR) method is of great interest among dental researchers and patients. Chemomechanical caries removal (CMCR) is a non-invasive intervention that removes decayed dentine, preserves sound dental tissues, and avoids pulp annoyance and patient discomfort. Recently, Papacarie has been established as a Chemomechanical caries removal method, which is a combination of papain, chloramine, toluidine blue, and salts that facilitates removal of the decayed tissue.
Papain, which is the basic component of Papacarie, is responsible for its bactericidal, bacteriostatic, and anti-inflammatory properties. In addition, Papacarie was observed to have no ability to destroy the underlying healthy collagen fibres and sound dentine, as Papain can digest only dead cells. The ease of application and no need for special devices is an added advantage of Papacarie. Currently, many clinical studies have been conducted to evaluate its efficiency in caries removal. The main outcome variables discussed in these researches studies are bacteria removing efficiency, pain perception, and time taken for caries removal. These research findings, however, were inconsistent and hinder the clinical application of Papacarie. There is a great deficiency of systematic review on the efficacy of the Papacarie method in caries removal in primary teeth. In addition, a previous published systematic review of Chemomechanical caries removal (CMCR) primarily considers only permanent teeth and research is lacking on primary teeth. Primary teeth, however, are more prone to lesion formation and progression than permanent teeth, and caries in primary teeth influence the children in biting, chewing, speaking, and their self-confidence. In addition, the outcome variables in previous systematic reviews are also limited. Mainly previous studies only compare the treatment time. Therefore, there is a lack of the comparison in reducing the cariogenic microbiota before and after the caries removal and pain perception in caries removal treatment. Hence, we performed a systematic review and meta-analysis in an attempt to elucidate the effectiveness and reliability of the Papacarie method.
Interpretation of the results
A bacteriological analysis was chosen as the method of assessment chosen in this study to test the effectiveness of both methods (conventional drilling method and Papacarie) for the completeness of caries removal. A reduction in the cariogenic bacterial counts responsible for the occurrence of dental caries was monitored as the presence of bacteria has been considered by many investigators to be an accurate indicator of infected carious dentine.
Five included studies discussed bacteria removal, but only two studies reported the specific results of colony forming units (CFU) reduction and included in the meta-analysis, which demonstrated that Papacarie could significantly decrease the bacteria remains in residual dentine more compared to the conventional drilling method. That finding is observed because Papacarie possesses a potent antimicrobial effect on all cariogenic bacteria, especially lactobacilli, as it diffuses by its low viscosity through the open dentinal tubules and eliminates cariogenic bacteria and thus leaves the cavity clean or even yielding bacterial counts of no clinical significance. And the heterogeneity of the colony forming units (CFU) reduction is I2 = 0% (95%CI 0%–98%). The point estimate I2 is low, but the range of 95% confidence interval (CI) of I2 is relatively broad. So the I2 statistic is not that precise to evaluate the heterogeneity. And the small number of studies included for the outcome induced the heterogeneity.
Pain perception is a very subjective judge, and various scales have been used to record the children’s feeling after caries removal. Pain perceptions were recorded by Wong-Baker-FACES (WBF) scores using the WSF Pain Rating Scale before and after different treatment methods in the included studies. Three studies were included in the present research, and the quality analysis shows that among the three studies, two had a low risk of bias, and the other one study had a moderate risk of bias, thus, the included data are reliable. Because pain perception is a very subjective judge, children’s personality and dental experience explained the heterogeneity (I2 = 86%, 95%CI 60%–95%). We observed that the patients experience considerably more pain when treated with the conventional drilling method because the loud noise and pressure on the sound dentine could cause additional pain. Contrary to the conventional drilling method, the Papacarie would only have a function for dead cells, and the dentine would be protected more completely. That property is close to the minimal invasive concept of paediatric dentistry. Only in this way can we protect as much sound dentin as possible and provide a patient relief during caries treatment. Although several studies also suggested that the patient’s fear of the dentist increased in the Papacarie group and decreased slightly in the conventional drilling method group. These researchers attributed this outcome to the longer treatment time needed for the CMCR group.
In this paper, we chose treatment time as an outcome to evaluate the efficacy and efficiency of caries removal in different methods. Among the seven studies, we made a conclusion that the Papacarie method is more timeconsuming than the conventional method. The heterogeneity of treatment time is, however, high, and it can be explained by that there is a lack of consistency guideline of the measurement of treatment time. Next, when we conducted the sensitivity analyses, I2 was 95% (95%CI 93%–97%), and a high heterogeneity still existed. This finding may be explained by the different location of the caries lesion, the size of the lesion and the different experiment environment. Despite all of the confounding factors above, the heterogeneity of our study is acceptable. In addition, a more strong conclusion needs further randomized controlled trials of good quality.
Advantages and limitations of the review
Several meta-analyses analysed the application of Chemomechanical caries removal in dental caries. Different from either published meta-analysis, the pain perception and evaluation of the reduction of the cariogenic microbiota, however, were finite. Few reviews have been completed on this topic. In the present study, we searched all of the related researches with only the inclusion of caries removal used in primary teeth were included. In our study, strict inclusions were implemented, and those studies comparing the efficient of caries removal methods between permanent teeth were excluded from this analysis. Risk of bias was minimized through rigorous study design and that increased reliability in the conclusion. More outcomes, such as patients’ acceptance and follow-up of the restorations, have also been evaluated in this study.
Several limitations of the present study should be recognized. First, all of the studies were conducted in India, Egypt, and Brazil, which limits the generalizability of the results. Hence, discrepancies in the caries removal among countries might have influenced the results. More clinical studies conducted in different countries are needed. Second, the power of formal tests was limited in this meta-analysis due to the lack of a long-term follow-up of the restorations, which indicates meaning that potential publication bias might have influenced our findings. Furthermore, it is necessary to use the subsequent caries rate as an outcome to evaluate the efficacy of Papacarie. Third, the caries type is not clear in the limited included studies, and the location of the caries may influence the efficacy of the caries removal. Further criteria regarding the baseline of caries type and specific treatment procedures may minimize heterogeneity between trials.
Conclusions
Papacarie is effective and efficient with the feature of selective caries removal considering the minimal invasive philosophy in paediatric dentistry. Papacarie displayed advantages in reducing the bacteria in carious dentine and decreasing the pain perception during caries removal in primary teeth among children, although it had a longer treatment time compared with the conventional method. Further studies applied Papacarie in caries removal in primary teeth in different countries are required.
Why this paper is important to paediatric dentists
It compared the efficiency of conventional caries removal method and Papacarie, which would help paediatric dentists to make treatment choices on their clinics based on the best scientific evidence available.
Paediatric dentists could know that Papacarie is an alternative to conventional caries removal method when making treatment choice for children who are afraid of drills and burs.
It explores the significance of following the painless treatment and minimal intervention principles in paediatric dentistry.
There are additional details about pediatric dentistry that you can obtain on our website.
List of authors:
YUEJIA DENG
GE FENG
BO HU
YUNCHUN KUANG
JINLIN SONG
References:
1 Musaiger AO, Takruri HR, Hassan AS, Abutarboush H. Food-based dietary guidelines for the Arab Gulf countries. J Nutr Metab 2012; 2012: 905303.
2 Sohn W, Burt BA, Sowers MR. Carbonated soft drinks and dental caries in the primary dentition. J Dent Res 2006; 85: 262.
3 Li R, Zhao Y, Ye L. How to make choice of the carious removal methods, Carisolv or traditional drilling? A meta-analysis. J Oral Rehabil 2014; 41: 432–442.
4 Fejerskov O, Larsen MJ, Richards A, Baelum V. Dental tissue effect of fluoride. Adv Dent Res 1994; 8: 15–31.
5 Lynch RJM. The primary and mixed dentition, posteruptive enamel maturation and dental caries: a review. Int Dent J 2013; 63(Suppl s2): 3–13.
6 Yengopal V, Harnekar SY, Patel N, Ni S. Dental fillings for the treatment of caries in the primary dentition. Cochrane Database Syst Rev 2016; 10(2): CD004483.
7 Berggren U, Meynert G. Dental fear and avoidance: causes, symptoms, and consequences. J Am Dent Assoc 1984; 109: 247.
8 Green RM, Green A. Adult attitudes to dentistry among dental attenders in South Wales. Br Dent J 1985; 159: 157–160.
9 Ayer WA Jr, Domoto PK, Gale EN, Joy ED Jr, Melamed BG. Overcoming dental fear: strategies for its prevention and management. J Am Dent Assoc 1983; 107: 18.
10 Allen KL, Salgado TL, Janal MN, Thompson VP. Removing carious dentin using a polymer instrument without anesthesia versus a carbide bur with anesthesia. J Am Dent Assoc 2005; 136: 643.
11 Rafique S, Fiske J, Banerjee A. Clinical trial of an air-abrasion/chemomechanical operative procedure for the restorative treatment of dental patients. Caries Res 2003; 37: 360–364.
12 Gupta S, Singh C, Yeluri R, Chaudhry K, Munshi AK. Clinical and microbiological evaluation of the carious dentin before and after application of Papacarie gel. J Clin Pediatr Dent 2013; 38: 133–138.
13 Ammari MM, Moliterno LFM. Remoc~ao quımicomec^ anica da carie: evid^encias atuais. Rev Bras Odontol 2005; 62: 125–127.
14 Bussadori SK, Castro LC, Galv~ao AC. Papain gel: a new chemo-mechanical caries removal agent. J Clin Pediatr Dent 2005; 30: 115.
15 Chadwick BL, Evans DJ. Restoration of class II cavities in primary molar teeth with conventional and resin modified glass ionomer cements: a systematic review of the literature. Eur Arch Paediatr Dent 2007; 8: 14–21.
16 Maragakis GM, Hahn P, Hellwig E. Clinical evaluation of chemomechanical caries removal in primary molars and its acceptance by patients. Caries Res 2001; 35: 205–210.
17 Anusavice KJ, Kincheloe JE. Comparison of pain associated with mechanical and chemomechanical removal of caries. J Dent Res 1987; 66: 1680.
18 Pandit IK, Srivastava N, Gugnani N, Gupta M, Verma L. Various methods of caries removal in children: a comparative clinical study. J Indian Soc Pedod Prev Dent 2007; 25: 93.
19 Inglehart MR, Peters MC, Flamenbaum MH, Eboda NN, Feigal RJ. Chemomechanical caries removal in children: an operator’s and pediatric patients’ responses. J Am Dent Assoc 2007; 138: 47–55.
20 Bussadori SK, Guedes CC, Bachiega JC, Santis TO, Motta LJ. Clinical and radiographic study of chemical-mechanical removal of caries using Papacarie: 24-month follow up. J Clin Pediatr Dent 2011; 35: 251–254.
21 Flindt M. Health and safety aspects of working with enzymes. Process Biochem 1978; 13: 3–7.
22 Dawkins G, Hewitt H, Wint Y, Obiefuna PC, Wint B. Antibacterial effects of Carica papaya fruit on common wound organisms. West Indian Med J 2003; 52: 290.
23 Beeley JA, Yip HK, Stevenson AG. Chemo chemical caries removal: a review of the techniques and latest developments. Br Dent J 2000; 188: 427–430.
24 Anegundi RT, Patil SB, Tegginmani V, Shetty SD. A comparative microbiological study to assess caries excavation by conventional rotary method and a chemo-mechanical method. Contemp Clin Dent 2012; 3: 388.
25 Swati C, Sonali S, Firoza S et al. Recent vs conventional methods of caries removal: a comparative in vivo study in pediatric patients. Int J Clin Pediatr Dent 2015; 8: 6.
26 Matsumoto SF, Motta LJ, Alfaya TA et al. Assessment of chemomechanical removal of carious lesions using Papacarie Duo TM: randomized longitudinal clinical trial. Indian J Dent Res 2013; 24: 488–492.
27 Peters MC, Flamenbaum MH, Eboda NN, Feigal RJ, Inglehart MR. Chemomechanical caries removal in children: efficacy and efficiency. J Am Dent Assoc 2006; 137: 1658.
28 Goyal PA, Kumari R, Kannan VP, Madhu S. Efficacy and tolerance of papain gel with conventional drilling method: a clinico-microbiological study. J Clin Pediatr Dent 2015; 39: 109–112.
29 Hamama HH, Yiu CK, Burrow MF, King NM. Systematic review and meta-analysis of randomized clinical trials on chemomechanical caries removal. Oper Dent 2015; 40: E167–E178.
30 Singh S, Singh DJ, Jaidka S, Somani R. Comparative clinical evaluation of chemomechanical caries removal agent papacarie with conventional method among rural population in india - in vivo study. Braz J Oral Sci 2012; 10: 193–198.
31 Higgins J, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Naunyn-Schmiedebergs Archiv fu¨ r experimentelle Pathologie und Pharmakologie 2011;5: S38.
32 Tsesis I, Rosen E, Taschieri S et al. Outcomes of surgical endodontic treatment performed by a modern technique: an updated meta-analysis of the literature. J Endod 2013; 39: 332–339.
33 Motta LJ, Bussadori SK, Campanelli AP et al. Pain during removal of carious lesions in children: a randomized controlled clinical trial. Int J Dent 2013; 2013: 896381.
34 Motta LJ, Bussadori SK, Campanelli AP et al. Randomized controlled clinical trial of long-term chemo-mechanical caries removal using Papacarie TM gel. J Appl Oral Sci 2014; 22: 307.
35 Motta LJ, Bussadori SK, Campanelli AP et al. Efficacy of Papacarie in reduction of residual bacteria in deciduous teeth: a randomized, controlled clinical trial. Clinics (Sao Paulo) 2014; 69: 319–322.
36 Ammari MM, Moliterno LF, Hirata JR et al. Efficacy of chemomechanical caries removal in reducing cariogenic microbiota: a randomized clinical trial. Braz Oral Res 1900; 28: 1–6.
37 El-Tekeya M, El-Habashy L, Mokhles N, El-Kimary E. Effectiveness of 2 chemomechanical caries removal methods on residual bacteria in dentin of primary teeth. Pediatr Dent 2012; 34: 325.
38 Bohari MR, Chunawalla YK, Ahmed BM. Clinical evaluation of caries removal in primary teeth using conventional, chemomechanical and laser technique: an in vivo study. J Contemp Dent Pract 2012; 13: 40–47.
39 Kochhar GK, Srivastava N, Pandit IK, Gugnani N, Gupta M. An evaluation of different caries removal techniques in primary teeth: a comparitive clinical study. J Clin Pediatr Dent 2011; 36: 5–9.
40 Kotb RM, Abdella AA, El Kateb MA, Ahmed AM. Clinical evaluation of Papacarie in primary teeth. J Clin Pediatr Dent 2009; 34: 117–123.
41 Lozano-Chourio MA, Zambrano O, Gonzalez H, Quero M. Clinical randomized controlled trial of chemomechanical caries removal (CarisolvTM). Int J Pediatr Dent 2010; 16: 161–167.
42 Maru VP, Kumar A, Badiyani BK et al. Behavioral changes in preschoolers treated with/without rotary instruments. J Int Soc Prev Community Dent 2014; 4: 77.
43 Maru VP, Shakuntala BS, Nagarathna C. Caries removal by chemomechanical (CarisolvTM)vs.rotary drill: a systematic review. Open Dent J 2015; 9: 462–472.
44 Divya G, Prasad MG, Vasa AAK et al. Evaluation of the efficacy of caries removal using polymer bur, stainless steel bur, carisolv, papacarie – an invitro comparative study. J Clin Diagn Res 2015; 9: 42–46.
45 Motta LJ, Martins MD, Porta KP, Bussadori SK. Aesthetic restoration of deciduous anterior teeth after removal of carious tissue with Papacarie. Indian J Dent Res 2009; 20: 117.
46 Suzan S, Kumar VAA, Divya G et al. Effectiveness of chemomechanical caries removal agents Papacarie and Carie-CareTM in primary molars: an in vitro study. J Int Soc Prev Community Dent 2016; 6: 391.