
Clinical Accuracy and Precision of 3 Multifrequency Electronic Apex Locators Assessed through Micro–Computed Tomographic Imaging
ABSTRACT
Introduction: This study aimed to compare the in vivo accuracy and precision of 3 electronic apex locators (EALs) in determining the position of the major foramen using micro–computed tomographic (micro-CT) technology. Further details about endodontic treatment are accessible for you to learn on our website in Endodontics section.
Methods: After access preparation of 23 necrotic or vital teeth from 5 patients, canals were negotiated, and hand files were used to determine the position of the foramen with 3 EALs: Propex Pixi (Dentsply Maillefer, Ballaigues, Switzerland), Woodpex III (Woodpecker Medical Instrument Co, Guilin, China), and Root ZX II (J Morita, Tokyo, Japan). After fixing the silicon stop to the file, teeth were extracted and scanned in a micro-CT device with and without the instrument inserted into the canal. Data sets were coregistered, and the accuracy and precision of the EALs were determined at a tolerance level of ±0.5 mm by measuring the distance from the tip of the instruments to a tangential line crossing the margins of the foramen. Statistical comparisons were performed using Friedman with post hoc related samples sign and Spearman tests (a = 5%).
Results: A significant difference was detected comparing the accuracy of Root ZX II (100%), Woodpex III (86.96%), and Propex Pixi (52.17%) (P < .05). There was a lack of significance in the relationship between the pulp status and the accuracy of the tested EALs (P > .05). Propex Pixi was significantly less precise than Root ZX II (P < .05), whereas no difference was found between Woodpex III and Root ZX II or Propex Pixi (P > .05).
Conclusions: EALs presented similar precision, but Woodpex III and Root ZX II showed better accuracy to determine the position of the apical major foramen than Propex Pixi.
INTRODUCTION
Most of the clinical and laboratory operational performances of electronic apex locators (EALs) have been assessed by testing their accuracy, precision, and repeatability using scanning electron microscopy(1), stereomicroscopy(2), or radiography(3) with or without grinding the root apex. Collectively, these studies focused on determining the distance from the file tip to some anatomic landmarks at the apical canal. Although these methodological approaches have been successfully used for decades, none of them allow the assessment of the 3-dimensional relationship between the instrument and the anatomic structures of the apex, an approach only able to be precisely done using nondestructive imaging techniques such as micro–computed tomographic (micro-CT) imaging(4-8).
Studies using micro-CT technology have demonstrated that the accuracy of EALs may be affected by the anatomic variations of the root canal system(6,7). Notwithstanding their conclusions pointing out the high precision of different brands of EALs in identifying the apical constriction and the major foramen, micro-CT imaging was used to determine the canal length and not the distance between the file tip and anatomic landmarks because teeth were scanned with no instrument in the canals. This means that it is not possible to identify changes in the trajectory of instruments caused by curvatures, calcifications, or accessory anatomies. Connert et al(4) and Suguru et al8 overcame this methodological limitation by scanning teeth and performing measurements with files fixed inside the root canals. When the numeric
display for the major foramen was used (0.0 mark), Suguru et al(8) reported that none of the tested EALs resulted in measurements extending beyond the foramen, whereas Connert et al(4) observed overestimation of the working length (WL) in all of the tested EALs (5%–71%), demonstrating that even analyses using the top-notch micro-CT imaging method may be still embroiled in controversial results. Although Connert et al(4) did not provide a single image to illustrate how measurements were performed, previous studies on EALs using micro-CT imaging(6,8,9) did not fully explore its high-quality 3-dimensional nature because the relationship between the tip of the instrument and the apex was not assessed. Recently, De-Deus et al(5) tested the clinical accuracy of a wireless apex locator by calculating the difference between the tip of the instrument and a tangent line crossing the margins of the major foramen using micro-CT imaging as an analytical tool. In this study, a double-scan micro-CT protocol was performed, thus allowing the reduction of artifacts produced by the metal alloy of instruments on dentin, which enabled the precise location of the file tip position in relation to the apex.
In the last decades, efforts have been made to further increase the accuracy of EALs by developing devices that measure the impedance characteristics using more than 2 frequencies. The Propex Pixi (Dentsply Maillefer, Ballaigues, Switzerland) is a multifrequency pocket-sized apex locator that uses several frequencies to measure the rapid change of impedance as the minor apical foramen is reached(10). The accuracy of the Propex Pixi in laboratory studies was reported to vary from 63%(11) to 93%(11-13) depending on the anatomic landmark used as reference. The Woodpex III (Woodpecker Medical Instrument Co, Guilin, China) is a recently launched multifrequency device that, according to the manufacturer, has its sensitivity improved by a new algorithm. To date, there is no published study on this device in the PubMed database, and information about its accuracy in the literature is still scarce. Preliminary laboratory data obtained using extracted teeth suggest that the Woodpex III has similar accuracy as the Root ZX mini (J Morita, Tokyo, Japan), Proper Pixi, and Raypex 6 (VDW Dental, Munich, Germany) to determine the WL in single-(14) and multirooted(15) teeth.
Accuracy and precision are 2 important outcome parameters to assess the performance of EALs(16). Accuracy describes how far measurements are away from a specific target, whereas precision describes how far the measurements are away from each other regardless of the target (ie, the scatter of the measurements)(17). Therefore, the present in vivo study was designed to compare the precision and accuracy of the Propex Pixi and Woodpex III apex locators. Root ZX II (J Morita) was used as the reference device, and micro-CT imaging was the analytical tool used to determine the distance between the file tip and the major foramen in different teeth and pulp conditions. The null hypothesis tested was that there would be no difference among the tested EALs in determining the location of the apical foramen in a clinical setting.
MATERIAL AND METHODS
Sample Size Calculation
The minimal sample size for this study was estimated using GPower 3.1 for Mac (G*Power 3.1 for Macintosh; Heinrich Heine, Universitat Dusseldorf, Dusseldorf, Germany) relying on analysis of variance for repeated measures and within factors from the F test family. The effect size input (0.5) was obtained from a previous study(5) with an alpha error of 0.05 and power beta of 0.95. The results indicated a minimal total sample size of 18 teeth to observe significant differences among groups.
Sample Selection
Five healthy adult patients referred for the extraction of 23 anterior and posterior teeth due to periodontal or prosthetic reasons participated in this study. Informed consent from all participants was obtained after this research protocol was approved by the local ethics committee (protocol 40352320.9.0000.5243). The inclusion criteria included teeth with complete root development, the presence of visible canals, and the absence of fracture or previous root canal treatment identified in a preoperative periapical radiograph (Digital Sensor 5100; Carestream Dental, Atlanta, GA) (Fig. 1A) as well as the existence of remaining tooth structure that allowed rubber dam isolation. Pulp sensibility was determined (Endo-Ice spray; Hygenic Corp, Akron, OH), and results were confirmed as either vital or necrotic after the pulp was accessed and the vascular status was determined. Demographic data (sex and age), identification of the experimental teeth, pulp status (vital or necrotic), and selected canals of anterior and posterior teeth used in this study are depicted in Table 1.
TABLE 1 - Demographic Data (Sex and Age) of 5 Donors, Identification of Experimental Teeth, Selected Canals of Posterior Teeth, Pulp Status (Vital or Necrotic), and Size of the Instrument Used to Determine the Position of the Apical Foramen at the 0.0 Mark of the Tested Electronic Apex Locators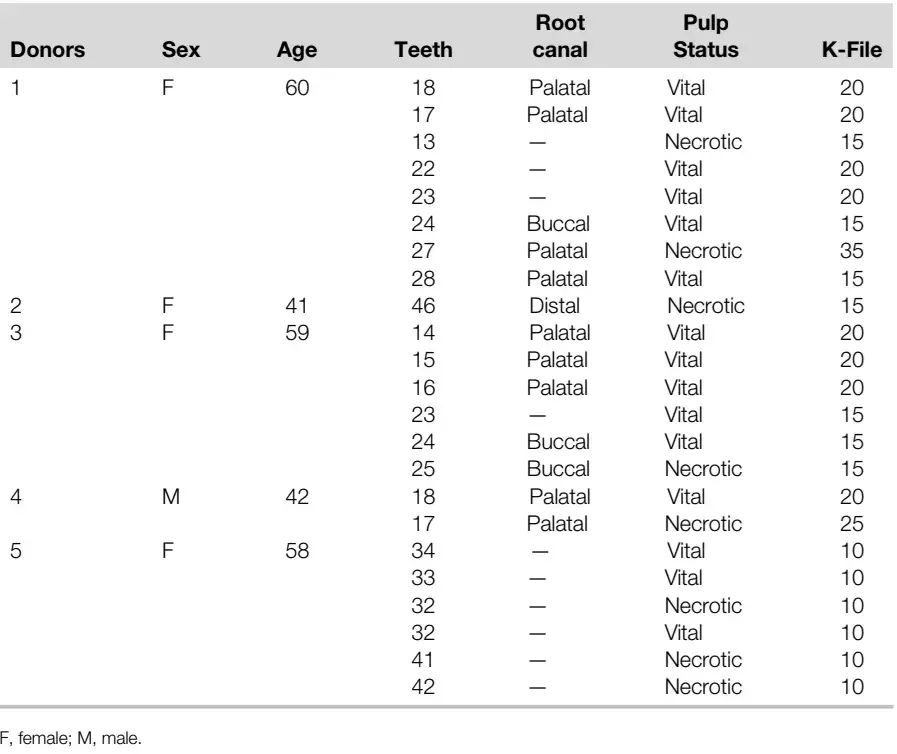
Experimental Procedures
After the administration of local anesthesia and isolation under a rubber dam, existing caries and/or restorations were removed. To establish a plateau serving as a flat and stable reference point for all measurements, the incisal edges or cusps of the elements were flattened with a diamond rotary instrument using a high-speed handpiece under water irrigation. In addition, the dental crown was marked with a notch created by a diamond cylindrical bur that later served as reference for the position of the silicone stop. After conventional access cavity preparation, the pulp chamber was irrigated with 2.5% sodium hypochlorite for 1 minute, and the coronal portion of the canal was enlarged using a Gates-Glidden drill size 1 or 2 (Dentsply Maillefer) depending on the orifice diameter. Then, the selected root canal was negotiated up to the apical third with size 08 and 10 K-files (Dentsply Maillefer) and rinsed with 2.5% sodium hypochlorite, and the pulp chamber was filled with the irrigant solution. After the aspiration of the excess of fluid from the pulp chamber, the WL was determined using 3 EALs (Root ZX II, Woodpex III, and Propex Pixi) in a random order. The lip clip was attached to the patient’s lip, and the largest stainless steel K-file to bind at the WL (Table 1) was connected to the electrode of the first selected device. The measurements were made by advancing the file into the root canal until the flashing bar display of the apex locator read “0.0,” indicating the position of the major foramen according to the manufacturers. Measurements were considered valid if the reading/signal on screen remained stable for at least 5 seconds. The length was electronically rechecked to confirm the file position, and an intraoperative radiograph was taken (Fig. 1B). Then, with the instrument still in the canal, the silicon stop was adjusted to the reference created on the external surface of the crown (Fig. 1C) and glued to the file with a synthetic adhesive composed of cyanoacrylate ester (Super Bonder; Henkel, Dusseldorf, Germany) € (Fig. 1D). After that, the file was withdrawn from the tooth, and a digital caliper (Mitutoyo, Tokyo, Japan) was used to measure the length between the tip of the instrument and the silicon stop to the nearest 0.01 mm. These steps were repeated in the same canal with the second and the third EALs using another file with similar dimensions. Teeth were then extracted and stored in distilled water. All clinical procedures were performed under magnification by an operator with 15 years of clinical experience.
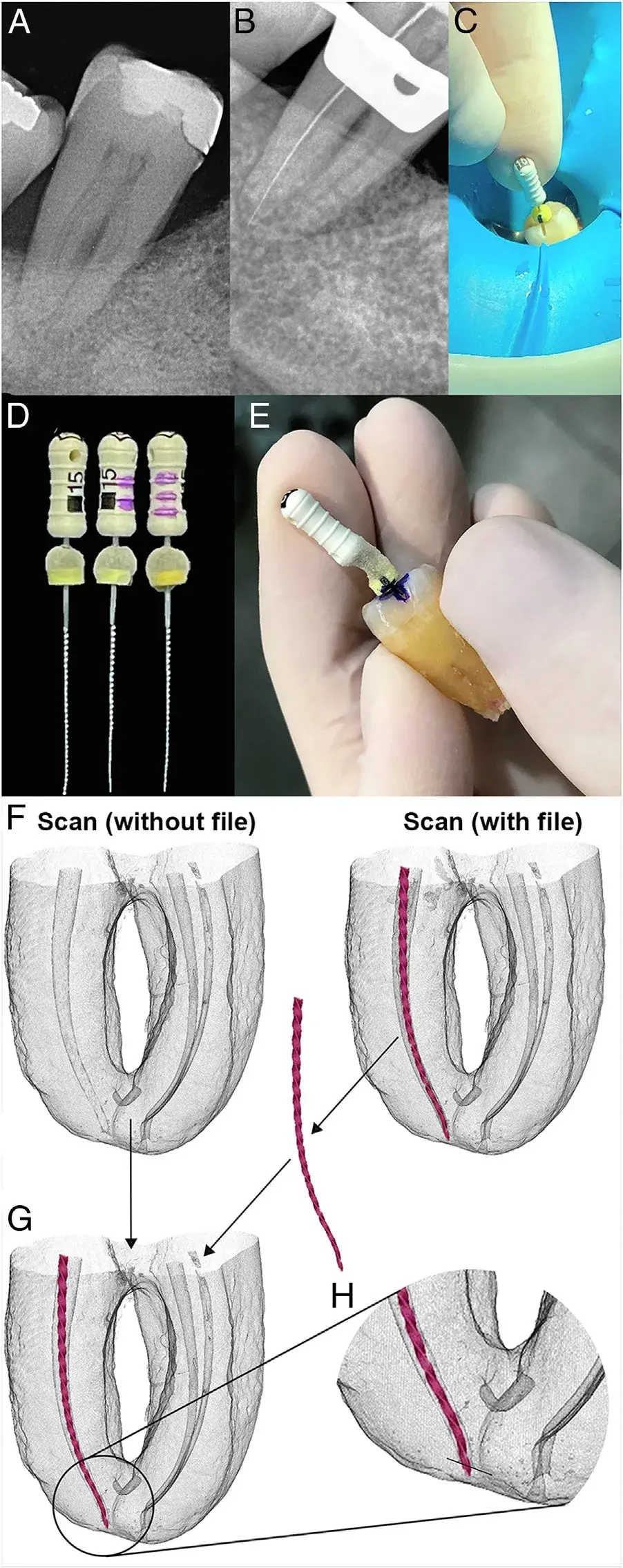 FIGURE 1 – Methodological procedures. (A ) A preoperative periapical radiograph of a mandibular second right molar. (B ) A transoperative radiograph showing a file in the distal canal positioned at the WL defined by the 0.0 mark of the apex locator. (C ) A size 15 K-file adjusted to a reference plateau created on the external surface of the crown. (D ) Three size 15 K-files showing silicon stops glued with a synthetic adhesive composed of cyanoacrylate ester after being adjusted to reference plateaus created on the external surface of the crown. (E ) After extraction, the instrument was reinserted into the root canal space for the scanning procedure. (F–H ) The double-scan protocol; each tooth was scanned in a micro-CT device (F ) without and with a file inserted into the canal. After the coregistration process, binarization thresholding was applied to extract the file from the data set; (G ) the file was added to the data set of the tooth scanned without the instrument using some Boolean operations. (H ) This double-scan protocol allows precise determination of the position of the file tip in relation to the apical foramen because it removes artifacts produced by the metal alloy into the dentin.
FIGURE 1 – Methodological procedures. (A ) A preoperative periapical radiograph of a mandibular second right molar. (B ) A transoperative radiograph showing a file in the distal canal positioned at the WL defined by the 0.0 mark of the apex locator. (C ) A size 15 K-file adjusted to a reference plateau created on the external surface of the crown. (D ) Three size 15 K-files showing silicon stops glued with a synthetic adhesive composed of cyanoacrylate ester after being adjusted to reference plateaus created on the external surface of the crown. (E ) After extraction, the instrument was reinserted into the root canal space for the scanning procedure. (F–H ) The double-scan protocol; each tooth was scanned in a micro-CT device (F ) without and with a file inserted into the canal. After the coregistration process, binarization thresholding was applied to extract the file from the data set; (G ) the file was added to the data set of the tooth scanned without the instrument using some Boolean operations. (H ) This double-scan protocol allows precise determination of the position of the file tip in relation to the apical foramen because it removes artifacts produced by the metal alloy into the dentin.
Micro-CT Scanning and Analyses
After slightly drying, each tooth was scanned 4 times in a micro-CT device (SkyScan 1173; Bruker-microCT, Kontich, Belgium) using the same pixel size (11.93 mm), frame average (5), and filter (1.0-mm-thick aluminum foil). In the first scan, the tooth was imaged without any instrument in the canal after setting the micro-CT device at 70 kV, 114 mA, and 360 rotation with steps of 0.5. The other 3 scans were performed at 90 kV, 88 mA, and 360 rotation with steps of 0.3 with each file used for WL determination with the 3 tested EALs inserted into the selected canal and adjusted to the reference mark at the crown (Fig. 1E). Image reconstructions were performed using standard parameters for ring artifact correction (4) and beam hardening correction (40%), whereas contrast limits varied from 0.0–0.12 (with the file) and from 0.0–0.05 (without the file) (NRecon v.1.7.16 software; Bruker-microCT), resulting in 1000–1200 grayscale cross-sectional images per tooth. Image stacks of teeth without instruments were rendered and coregistered with data sets acquired with the file inserted into the selected canal (3D Slicer 4.6.0 software). Then, a binarization thresholding process was applied to extract the file from the data set followed by some Boolean operations that added it to the data set of the tooth scanned without the instrument(5), allowing the visualization of the anatomic structures of the apex without artifacts created by the metal alloy (Fig. 1F–H). The accuracy and precision of the tested EALs were determined by measuring the distance from the tip of the file to a tangential line crossing the edges of the major apical foramen after aligning the apical third of the tooth in the 3 views (coronal, sagittal, and axial) using FIJI/imageJ (Fiji v.1.51n, Fiji, Madison, WI). Accuracy described how far measurements are away from the referred tangential line, whereas precision characterized the scatter of measurements. The results were recorded in millimeters and categorized according to the position of the instrument’s tip as positive (beyond the foramen), negative (within the canal space), or 0 (at the tangential line) (Fig. 2A–C). All laboratory analyses were performed by an experienced evaluator in micro-CT imaging blinded to the apex locator devices.
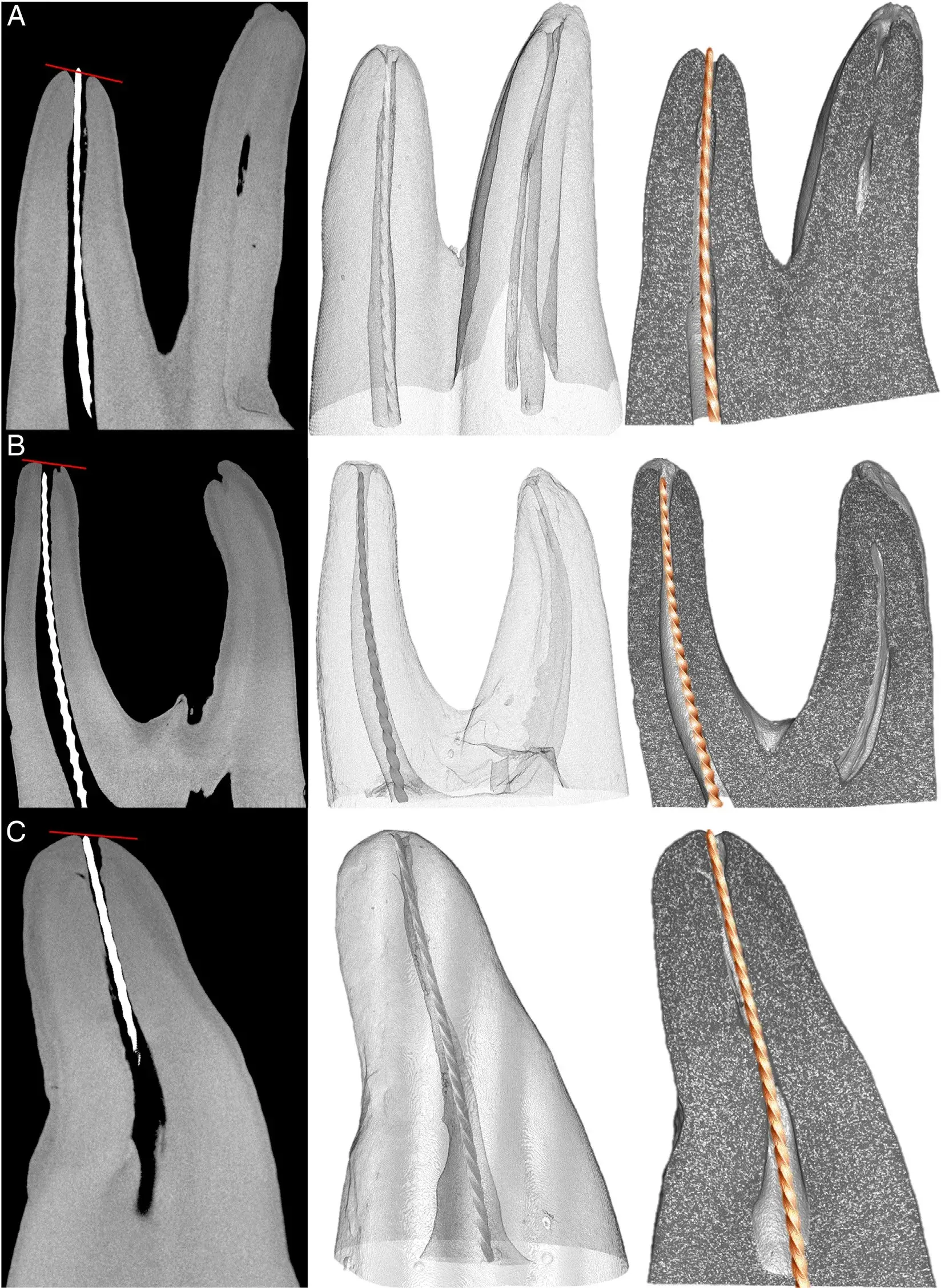 FIGURE 2 – Longitudinal cross sections (on the left ) and 3-dimensional representative models (on the right ) of 3 teeth categorized according to the position of the instrument’s tip as (A ) positive (beyond the foramen), (B ) negative (within the canal space), or (C ) zero (at the tangential line, in red ).
FIGURE 2 – Longitudinal cross sections (on the left ) and 3-dimensional representative models (on the right ) of 3 teeth categorized according to the position of the instrument’s tip as (A ) positive (beyond the foramen), (B ) negative (within the canal space), or (C ) zero (at the tangential line, in red ).
Statistical Analyses
To determine the accuracy of the 3 EALs, the frequency distributions of the measured distances were initially categorized at a tolerance level of ±0.5 mm from the foramen. Frequencies displayed from 10.5 to –0.5 mm were summed up and considered as accurate, whereas the other frequencies were combined and labeled as inaccurate. Accurate and inaccurate ranks were compared using the Friedman test followed by a related samples Wilcoxon signed rank test adjusted for alpha-type error using the Bonferroni procedure for pairwise comparisons. Accuracy categories were also correlated with the status of the pulp (vital or necrotic) using the Spearman test.
To determine the precision of the EALs, the absolute distances from the file tip to the tangential line per group were firstly checked for skewness (Shapiro-Wilk, P < .05) and further compared using the related samples statistical procedure (Friedman test). Pairwise comparisons were made using the related samples sign test adjusted for alpha-type error using the Bonferroni procedure. All statistical procedures were performed with an alpha error of 5% (SPSS v.24 for Windows; IBM Corp, Armonk, NY).
There are additional information about modern techniques of endodontic treatment that you can gain in our course "What's new in endodontics: from anesthesia to obturation".
RESULTS
The percentage frequency distribution and descriptive data regarding the distance from the file tip to the tangential line positioned at the major foramen are presented in Table 2.
Figure 3A displays the distances from the file tip to the tangential line measured in each specimen as well as the accuracy range (±0.5 mm from the apical foramen). A significant difference was detected comparing the accuracy of Root ZX II (100%), Woodpex III (86.96%), and Propex Pixi (52.17%) (P = .001) (Table 2, Fig. 3B). The related samples Wilcoxon signed rank test indicated that Propex Pixi was less accurate than Root ZX II (P = .001) and Woodpex III (P = .021), whereas no difference was detected between Root ZX II and Woodpex III (P = .083). In 4 root canals (17.39%), measurements with Root ZX II and Woodpex III were performed exactly at the major foramen, whereas Propex Pixi resulted in measurements longer or shorter than 1.0 mm in 8 root canals (34.78%). The Spearman correlation test indicated a lack of significance in the relationship between the pulp status and the accuracy of Woodpex III (P= 20.012, r 2 = 0.957) and Propex Pixi (P = .492, r 2 = 20.151). Root ZX could not be correlated because its accuracy was 100%. A comparison of EALs regarding precision showed a significant difference among them (P = .034, Friedman test). The related samples sign test was able to detect that Propex Pixi was significantly less precise than Root ZX II (P = .035), whereas no difference was found when comparing Woodpex III (95% confidence interval [CI], 20.21 to 0.04) with either Root ZX II (95% CI, 20.06 to 0.04) (P = .302) or Propex Pixi (95% CI, 21.38 to 0.23) (P = .289).
TABLE 2 - The Percentage Frequency Distribution and Descriptive Data Regarding the Distance from the File Tip to the Tangential Line Positioned at the Major Foramen Determined by 3 Electronic Apex Locators (n = 23)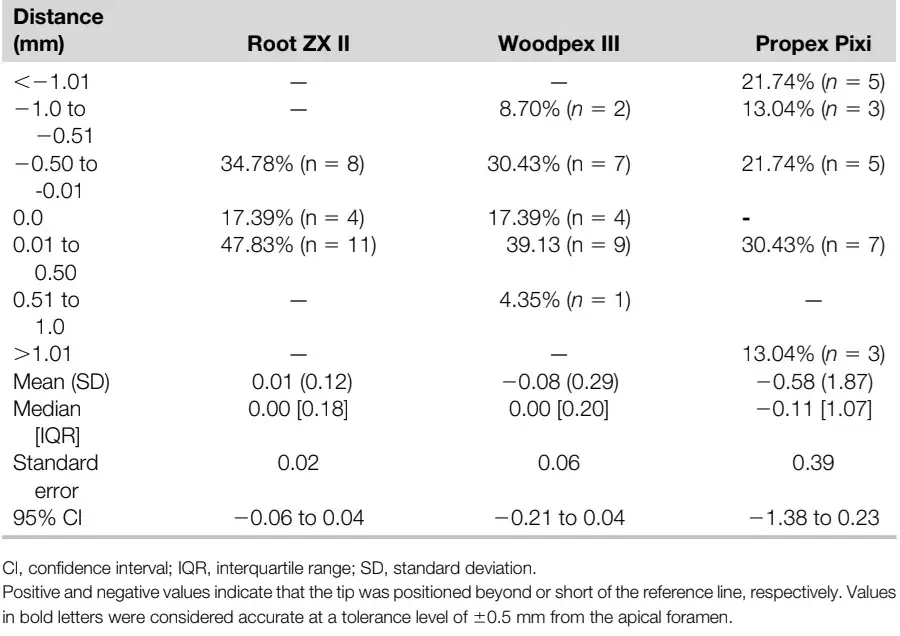
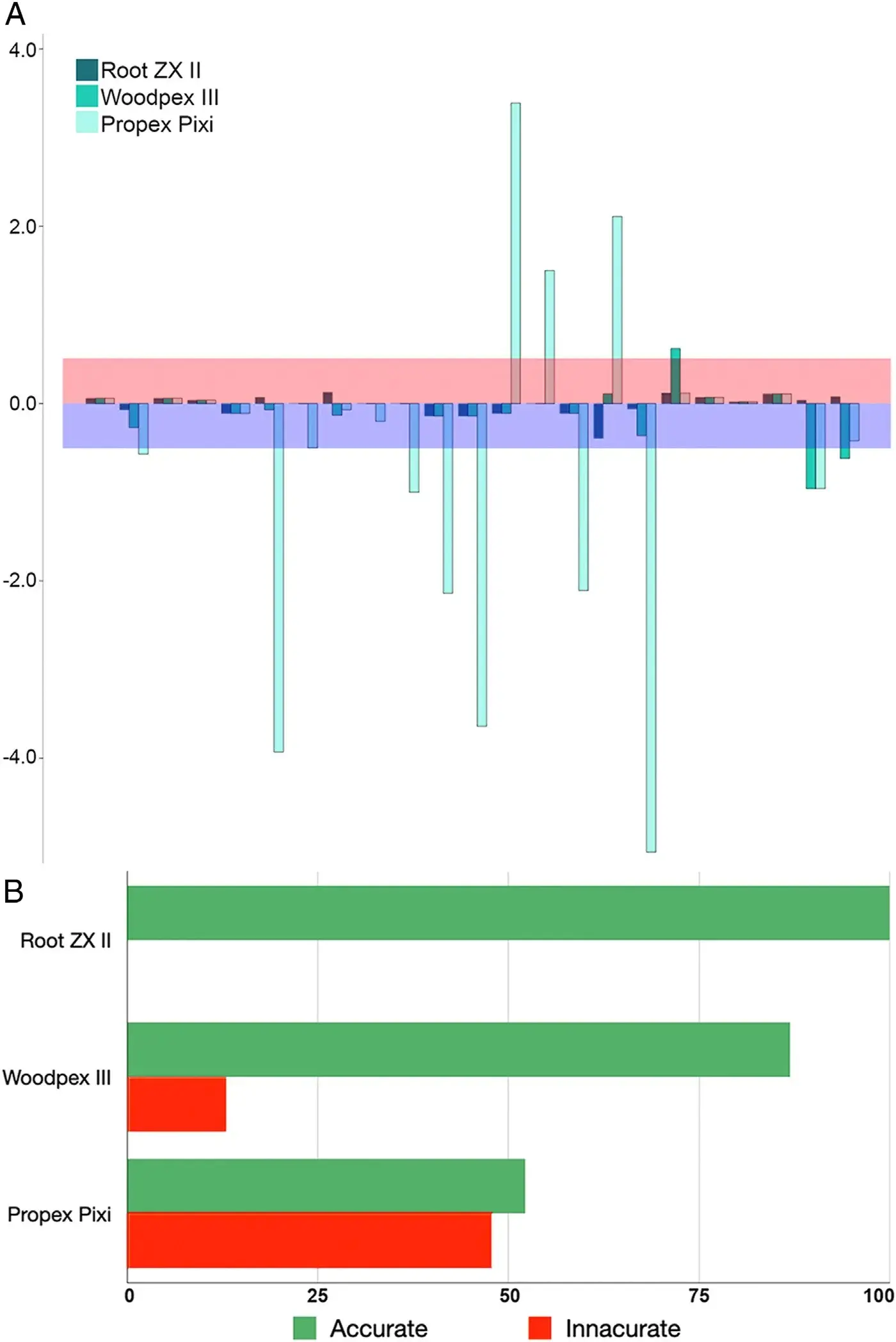 FIGURE 3 – (A ) A graphic representation showing the distances from the file tip to the tangential line measured in each specimen as well as the accuracy range (±0.5 mm) of measurements obtained beyond (pink stripe) and short (purple stripe) of the apical foramen. (B ) Accurate and inaccurate percentage frequencies obtained after measuring the distances from the file tip to the tangential line acquired after using Root ZX II, Woodpex III, and Propex Pixi apex locators in 23 teeth.
FIGURE 3 – (A ) A graphic representation showing the distances from the file tip to the tangential line measured in each specimen as well as the accuracy range (±0.5 mm) of measurements obtained beyond (pink stripe) and short (purple stripe) of the apical foramen. (B ) Accurate and inaccurate percentage frequencies obtained after measuring the distances from the file tip to the tangential line acquired after using Root ZX II, Woodpex III, and Propex Pixi apex locators in 23 teeth.
DISCUSSION
The present study was performed in a clinical setting to evaluate the performance of Root ZX II, Woodpex III, and Propex Pixi EALs. After extraction, the nondestructive micro-CT technology was used as the analytical tool to determine the distance between the file tip and the major foramen in different teeth and pulp conditions. Within a tolerance level of ±0.5 mm, the results showed significant differences in the accuracy and precision among the tested EALs (Table 2, Fig. 3); thus, the null hypothesis was rejected. Root ZX II and Woodpex III were able to precisely detect the position of the major foramen in 4 root canals (17.4%), and measurements were within the tolerance level in 23 (100%) and 20 (86.9%) canals, respectively. On the other hand, Propex Pixi was unable to detect the exact position of the major foramen, and measurements were outside the tolerance range in 11 root canals (47.8%), and in 8 of them (34.7%), the tip of the file was positioned in distances higher than 1 mm from the apical foramen.
Because it is well established that poorer outcomes are associated with overfilling of the root canal(18), if a strict clinical tolerance limit is applied (only values within 0.5 mm short of the foramen) to the results(17), accuracies are reduced to 52.1% (Root ZX II), 47.8% (Woodpex III), and 21.7% (Propex Pixi), suggesting that in clinical conditions WL determination with these EALs using the 0.0 mark would require an adjustment of the file to keep it within the limits of the root canal space(5).
Root ZX has been the most tested EAL in the endodontic literature17; it is considered the gold standard against which newer EALs are compared(19). In the literature, 4 in vivo studies using conventional methods have tested the Root ZX at the 0.0 mark as in the current research(1,16,20,21), but only 1 calculated its accuracy(1). According to Pagavino et al(1), the in vivo accuracy of the Root ZX was 82.75% at a tolerance range of ±0.5 mm, a lower value than the present findings (100%), which can be explained by methodological differences because those authors used scanning electron microscopy for the analysis. More recently, De-Deus et al(5) used the same methodological approach used herein to test the Root ZX II and reported accuracies of 81.8% (using strict limits) and 100% (at a tolerance limit of ±0.5 mm), which are in line with the present results. Although Root ZX II was the only EAL in this study that was accurate in all selected root canals (Table 2), a strict tolerance limit indicated measurements beyond the apical foramen in 47.8% of them (n = 11). These findings are corroborated by other authors who also observed extension of the file tip beyond the major foramen using Root ZX in 40%(22), 32.1%(23), 30.8%(24), 27.3%(5), 26%(25), and 16.7%(13,19) of their samples. Because of these results, some authors have proposed that when determining the WL using the 0.0 mark of the apex locator, the instrument should be withdrawn by approximately 0.5 mm(3,19,22). However, this practice is not accepted universally, and differences remain among clinicians with respect to their preferences for the ideal WL(19).
In the present study, Woodpex III showed similar accuracy and precision compared with Root ZX II. Both devices were able to precisely determine the position of the apical foramen in 17.3% of the root canals and showed no measurement away from the apical foramen by more than 1 mm (Table 2, Fig. 3). The results achieved by the multifrequency Woodpex III might be supported by its innovative anti-interference algorithm implemented to make it more stable, as stated by the manufacturer. Considering there are still no published data on this device in the scientific indexed literature, it is not possible to compare the present results with other studies. However, results from laboratory studies using extracted teeth and published in non-English journals(14,26) reported similar accuracies of Woodpex III and Root ZX to determine the WL, corroborating the present findings.
In this investigation, Propex Pixi was significantly less accurate and precise than Root ZX II and significantly less accurate than Woodpex III. Measurements longer or shorter than 1.0 mm were observed in 8 root canals (34.7%), and accuracy was 52.1% at a tolerance range of ±0.5 mm. The accuracy of the multifrequency pocket-size Propex Pixi in laboratory studies was reported to be 87%–93% at the major foramen(11-13), 80%–83% ±0.5 mm of the minor foramen(13,27,28), and 63%–67% 1 mm short of the apical foramen(11). Çinar & Ustun 29 reported similar in vivo accuracy of Propex Pixi, Mini Root ZX, and Raypex 5 (VDW, Munich, Germany) to determine the position of the apical constriction under different intracanal contents in 18 patients (25 teeth). The authors used micro-CT scans of the extracted teeth to identify the position of the apical constriction and to calculate its distance from the major foramen but reported only absolute values.
In another in vivo study, Serna-Pena et al ~ 13 tested the accuracy of Root ZX mini, Apex ID (Kerr Dental, Brea, CA), and Propex Pixi in 30 single-rooted teeth. The authors used the 0.5 display mark of EALs and compared the length of the file used for measurement with the actual WL established 0.5 mm short of the major foramen, which was calculated after tooth extraction. The accuracy of Propex Pixi was 83.3% at a tolerance limit of ±0.5 mm of the actual WL, and the file tip extended beyond the major foramen in 13.3% of the canals. The accuracy values of Propex Pixi in the literature are higher than that reported in the present study, which may be partially explained by methodological differences. Another possible explanation might be related to its clinical use. We noticed that this EAL was the only one that took more time to achieve a stable reading/signal on screen during WL determination. In fact, several attempts were made with this device until it reached 5 seconds of stability with the file positioned at the WL, as determined in our research protocol. Further in vivo studies with this device using reliable methodological approaches are recommended to corroborate the present findings.
In the literature, several clinical studies using conventional methodologies have tested the accuracy of EALs in different groups of teeth and used the 0.5 display mark as reference for WL determination(2,19,22-25,30-33).
Manufacturers have claimed that this display mark determines the position of the apical constriction, whereas, in fact, it has been considered an arbitrary indicator of the apical position of the file(16). This statement is supported by our findings and previous studies using micro-CT technology(4,5).
Therefore, in the present study, the major foramen (0.0 display mark of the EAL) rather than the minor foramen(11,16,19,22) was chosen as the reference point not only because its position canbe consistently reproduced but also because of the possibility of being reliably identified in the acquired micro-CT images(5).
This study also established the tolerance range at ±0.5 mm from the apical foramen because this margin of error has been considered an acceptable limit of agreement for WL measurements made by EALs in most of the in vivo studies(1,2,16,22-25,31,33).
Apical periodontitis is an infectious disease of periapical tissues with an endodontic origin that activates immune/inflammatory responses and may alter the morphology of the root apex, resulting in apical canal diameter enlargement, apical foramen deviation, and partial or even complete distortion of the apical constriction, which may influence the accuracy of EALs(34). In the present study, a lack of significance in the relationship between the pulp status and the performance of Root ZX II, Woodpex III, and Propex Pixi was observed, a finding consistent with previous studies showing that the pulp condition has no significant effect on the accuracy of EALs(9,22,25,34). In the absence of relevant apical root resorption, this would be an expected outcome considering that modern EALs determine the WL by measuring impedance with different frequencies, reducing the influence of several factors on its precision. However, it may be of interest that most of the registered positive values (measurements beyond the foramen) were achieved in teeth with necrotic pulp and apical periodontitis, which was also observed by Saatchi et al(34). Therefore, clinicians should consider the potential of overinstrumentation in teeth with apical periodontitis when using the 0.0 mark of the EAL as the reference for WL determination. The main advantages of the present study are that it was performed in a clinical environment using the nondestructive and reliable micro-CT technology as an analytical tool, which allowed the comparison of different EALs in the same root canals, instead of testing in different teeth(4).
In addition, the use of a double-scan protocol provided the possibility of evaluating the real position of instruments without interferences of artifacts created by the metal alloy during the scanning procedure. Although this study included a relatively large sample size for an in vivo study (23 teeth), a limitation of this study was related to the small number of donors (n 5 5) with ages ranging from 41–60 years old, which did not allow for a high variability of intraoral conditions. Future studies should be focused on validating conventional techniques by comparing them with the present methodology in order to determine the accuracy of different EALs in the same teeth through micro-CT scanning.
CONCLUSIONS
Within the limitations of this in vivo study, the tested EALs presented similar precision, but Woodpex III and Root ZX II showed better accuracy in determining the position of the major apical foramen than Propex Pixi.
You have the opportunity to gather more in-depth information about endodontic treatment protocols in complex cases in our course "Endodontics: from classic protocols to extreme".
List of authors:
Gustavo De-Deus, Viviany Cozer, Erick Miranda Souza, Emmanuel Joao Nogueira Leal Silva, Felipe Gonçalves Belladonna, Marco Simoes-Carvalho, Marco Aurelio Versiani
References
Pagavino G, Pace R, Baccetti T. A SEM study of in vivo accuracy of the Root ZX electronic apex locator. J Endod 1998;24:438–41.
Kim E, Marmo M, Lee CY, et al. An in vivo comparison of working length determination by only root-ZX apex locator versus combining root-ZX apex locator with radiographs using a new impression technique. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:e79–83.
Pascon EA, Marrelli M, Congi O, et al. An in vivo comparison of working length determination of two frequency-based electronic apex locators. Int Endod J 2009;42:1026–31.
Connert T, Judenhofer MS, Hulber JM, et al. Evaluation of the accuracy of nine electronic apex locators by using Micro-CT. Int Endod J 2018;51:223–32.
De-Deus G, Cozer V, Souza EM, et al. Micro-CT study of the in vivo accuracy of a wireless electronic apex locator. J Endod 2022;48:1152–60.
Piasecki L, Carneiro E, da Silva Neto UX, et al. The use of micro-computed tomography to determine the accuracy of 2 electronic apex locators and anatomic variations affecting their precision. J Endod 2016;42:1263–7.
Piasecki L, Jose Dos Reis P, Jussiani EI, Andrello AC. A micro-computed tomographic evaluation of the accuracy of 3 electronic apex locators in curved canals of mandibular molars. J Endod 2018;44:1872–7.
Suguro H, Nishihara A, Tamura T, et al. The use of micro-computed tomography to determine the accuracy of electronic working length with two apex locators. J Oral Sci 2021;63:167–9.
Piasecki L, Carneiro E, Fariniuk LF, et al. Accuracy of Root ZX II in locating foramen in teeth with apical periodontitis: an in vivo study. J Endod 2011;37:1213–6.
Ustun Y, Aslan T, Sekerci AE, Sagsen B. Evaluation of the reliability of cone-beam computed tomography scanning and electronic apex locator measurements in working length determination of teeth with large periapical lesions. J Endod 2016;42:1334–7.
Oliveira TN, Vivacqua-Gomes N, Bernardes RA, et al. Determination of the accuracy of 5 electronic apex locators in the function of different employment protocols. J Endod 2017;43:1663–7.
Bernardo RCFD, Alves LS, Bruno AMV, et al. The accuracy of electronic apex locators for determining working length: an in vitro study with artificial teeth. Aust Endod J 2021;47:217–21.
Serna-Pena G, Gomes-Azevedo S, Flores-Trevino J, et al. ~ In vivo evaluation of 3 electronic apex locators: Root ZX Mini, Apex ID, and Propex Pixi. J Endod 2020;46:158–61.
Mansilla M. Eficacia in vitro de dos localizadores electronicos apicales Woodpex III y Propex Pixien piezas uniradiculares. Vis Odontol 2018;5:34–40.
Mio-Suclupe RE, García-Rupaya CR. Comparacion de la precision de la longitud de trabajo decuatro localizadores apicales electronicos con limas de acero inoxidable y níquel-titanio enconductos mesiovestibulares de primeras molares inferiores. Rev Cient Odontol 2020;8:e28–36.
Adorno CG, Solaeche SM, Ferreira IE, et al. The influence of periapical lesions on the repeatability of two electronic apex locators in vivo. Clin Oral Investig 2021;25:5239–45.
ElAyouti A, Connert T, Dummer P, Lost C. A critical analysis of research methods and experimental models to study working length determination and the performance of apex locators–a narrative review with recommendations for the future. Int Endod J 2022;55(Suppl 2):281–94.
Ng YL, Mann V, Rahbaran S, et al. Outcome of primary root canal treatment: systematic review of the literature–part 2. Influence of clinical factors. Int Endod J 2008;41:6–31.
Stober EK, Duran-Sindreu F, Mercade M, et al. An evaluation of Root ZX and iPex apex locators: € an in vivo study. J Endod 2011;37:608–10.
Orosco FA, Bernardineli N, Garcia RB, et al. In vivo accuracy of conventional and digital radiographic methods in confirming root canal working length determination by Root ZX. J Appl Oral Sci 2012;20:522–5.
Williams CB, Joyce AP, Roberts S. A Comparison between in vivo radiographic working length determination and measurement after extraction. J Endod 2006;32:624–7.
Wrbas KT, Ziegler AA, Altenburger MJ, Schirrmeister JF. In vivo comparison of working length determination with two electronic apex locators. Int Endod J 2007;40:133–8.
Duran-Sindreu F, Gomes S, Stober E, et al. In vivo evaluation of the iPex and Root ZX electronic apex locators using various irrigants. Int Endod J 2013;46:769–74.
Shabahang S, Goon WW, Gluskin AH. An in vivo evaluation of Root ZX electronic apex locator. J Endod 1996;22:616–8.
Dunlap CA, Remeikis NA, BeGole EA, Rauschenberger CR. An in vivo evaluation of an electronic apex locator that uses the ratio method in vital and necrotic canals. J Endod 1998;24:48–50.
Plos AC, Perez Fernandez N, Pizarro Meneses C, et al. Comparacion de la conductometría electronica en conductos curvos simulados antes y despues de la colocacion de hidroxido de calcio. Rev Fac Odont Buenos Aires 2021;35:7–11.
Gehlot PM, Manjunath V, Manjunath MK. An in vitro evaluation of the accuracy of four electronic apex locators using stainless-steel and nickel-titanium hand files. Restor Dent Endod 2016;41:6–11.
Saxena D, Saha SG, Bharadwaj A, et al. A comparative evaluation of accuracy of three electronic apex locators using histological section as gold standard: an ex vivo study. J Conserv Dent 2017;20:251–4.
Çinar F, Ust € un Y. € Ex vivo evaluation of the accuracy of 3 electronic apex locators in different environments: a micro-computed tomography study. Eur Endod J 2020;5:226–30.
Fadel G, Piasecki L, Westphalen VP, et al. An in vivo evaluation of the auto apical reverse function of the Root ZX II. Int Endod J 2012;45:950–4.
Haffner C, Folwaczny M, Galler K, Hickel R. Accuracy of electronic apex locators in comparison to actual length–an in vivo study. J Dent 2005;33:619–25.
Mandlik J, Shah N, Pawar K, et al. An in vivo evaluation of different methods of working length determination. J Contemp Dent Pract 2013;14:644–8.
Welk AR, Baumgartner JC, Marshall JG. An in vivo comparison of two frequency-based electronic apex locators. J Endod 2003;29:497–500.
Saatchi M, Aminozarbian MG, Hasheminia SM, Mortaheb A. Influence of apical periodontitis on the accuracy of 3 electronic root canal length measurement devices: an in vivo study. J Endod 2014;40:355–9.