
Benign tumors of cartilage tissue
Machine translation
Original article is written in RU language (link to read it) .
Benign neoplasms of cartilage tissue include the following tumors:
enchondromas are formed from cartilage tissue localized in the bone marrow canal;
ecchondromas, develops from cartilaginous tissue located in the outer layers of the bone;
osteochondroma, the structure of this tumor contains both cartilage and bone tissue;
chondroblastoma is the most rare tumor of cartilage tissue, occurring mainly in childhood or adolescence.
About the causes of tumors, MRI diagnostics and treatment tactics at the webinar Injuries, tumors, ankylosis of the TMJ. Craniofacial deformities .
Chondroma
Chondroma is a benign neoplasm, which is represented by cartilage tissue. Rarely found in jaw bones.
Chondromas of the jaw bones are usually divided into two types: enchondromas (formed intraosseously), ecchondromas (formed on the outer surface of the jaw, spread exophytically).

Figure 1. Chondroma on x-ray.
Pathogenesis
The mechanism of chondroma formation is not fully understood, but there are several hypotheses in this regard:
B.I. Migunov believes that the source of the development of jaw chondroma are fragments of Meckelian cartilage.
K. Thoma suggests that chondromas of the jaw bones are of embryonic origin.
Ch. Geshickter and Copeland, based on their own observations, suggest that the source of chondromas is zones of natural bone formation.
Chondromas affect the jaw bones mainly in elderly people; they are less common in middle age. Most often, chondromas are observed in women, and their typical location is the median suture on the upper jaw. Chondroma can be detected in the lower jaw in the retromolar region, the condylar process.
Clinical picture
The shape and size of a benign neoplasm made of cartilage tissue can be different, the consistency is cartilaginous, the surface is lumpy, and during surgical removal a fibrous capsule is revealed. Slow growth is typical for chondroma, without pain or other unpleasant sensations.

Figure 2. Histological structure of chondroma.
Pain syndrome occurs in the case of large tumors; paresthesia may occur, mobility of individual teeth, displacement may occur, and in advanced cases, deformation of the bones of the facial skeleton.
The tumor is surrounded on the outside by an unchanged membrane. When the chondroma is located subcutaneously, the skin over the tumor does not change. Palpation of chondroma is usually painless; palpation reveals a dense consistency, smooth or lumpy surface, and the borders of the chondroma are relatively clear. The tumor is never associated with the teeth, but the roots of the teeth located in the tumor area undergo resorption.
In the case of primary localization in the upper jaw, the chondroma often grows into the zygomatic bone, which is accompanied by significant deformation of the face. With chondroma, enlargement of the lymph nodes is not observed.
Echondromas are found mainly on the bones of the upper jaw. The predominant localization is the alveolar process, less often - the thickness of the bone. Large tumors often grow into the orbit, nasal cavity, and maxillary sinus.
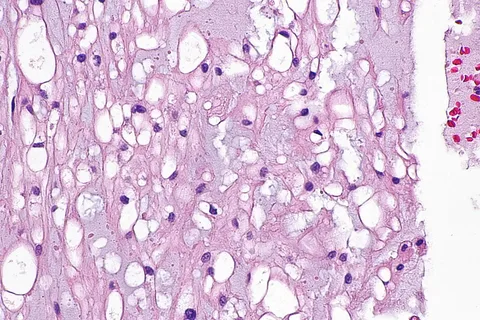
Figure 3. Microscopic examination of chondroma.
Enchondromas occur equally on the upper and lower jaws. An increase in the size of the tumor entails the appearance of toothache, displacement of teeth, and the occurrence of their mobility. During palpation, a motionless tumor of dense consistency is determined. The surrounding soft tissues do not change in color. Tumor growth is slow.
X-ray diagnostics
The following changes are detected on the x-ray:
a focus of clearing that has round or irregular outlines,
sharp border with unchanged bone,
resorption of tooth roots that are located in the growth zone of the tumor.
Macroscopic characteristics of chondroma
pearlescent shade,
the tuberous outer surface of the ecchondroma, and when cut, the enchondroma.
Microscopic structure
Chondroma is represented by hyaline cartilage containing layers of connective tissue in which blood vessels pass. In the thickness of the ground substance there are cartilaginous cells surrounded by a capsule; two nuclei are often found in them.
The main difference between chondroma and chondrosarcoma is rare mitoses, homogeneity of the tumor structure and the almost complete absence of cellular elements.
Histological characteristics of chondroma
Represented by randomly arranged cartilage cells.
The tumor differs from ordinary cartilage tissue in its impressive size.
Cartilaginous cells contain one semicircular nucleus, which is dark-colored; several vacuoles can be identified in the cytoplasm.
Between the cartilage cells you can find calcareous deposits, which are dust-like accumulations, individual bone fragments that do not have vascular canals.
The intercellular substance is edematous, in some cases it can be mucous.
Differential diagnosis
It is necessary to be able to distinguish chondromas from various bone lesions: osteochondral exostoses, osteomas, enchodromas, the latter must be differentiated from osteoblastoclastomas, fibrous dysplasia.
The eccentric location of fibrous dysplasia is not accompanied by swelling of the bone and has a denser consistency. To make an accurate diagnosis, histological examination is necessary.

Figure 4. Diagnosis of chondroma.
Treatment
Chondromas can only be treated surgically (radical excision of the tumor within healthy tissue). It is important to take into account the fact that recurrence and malignancy are typical for chondroma. The tumor is excised together with adjacent tissues; approximately 1 cm should be retreated from the tumor border. To prevent recurrence of ecchondroma, partial resection of bone tissue is performed. Since the surgical procedure involves resection of the jaw, a fixation splint is pre-made so that bone grafting can be performed immediately. At least 4 months after surgery, orthopedic treatment begins.
Chondroblastoma
Chondroblastoma is a type of benign neoplasm of cartilage tissue; it is a little studied tumor, since it is quite rare. It was first described by Codman in 1931, its first name was epiphyseal chondromatous giant cell tumor. This name is due to the fact that the tumor can simultaneously contain chondroblasts along with osteoclasts (giant cells).
Chondroblastoma is considered by scientists to be an intermediate form of tumor, occupying a middle position between osteoblastoclastomas and chondromas. Today, the term “chondroblastoma” is recognized by specialists from all over the world, indicating the cartilaginous genesis of the neoplasm.
In addition to benign chondroblastomas, there are also malignant forms.
Clinical picture
Chondroblastoma is observed mainly in young people who have not yet completed epiphyseal growth, these are children and adolescents, less often young people, but not older than 20 years. Clinical manifestations are identical to those of chondroma.
X-ray features of chondroblastoma
A single lesion, small in size, no more than 5 mm in diameter.
The outlines of the lesion are round or oval.
The location relative to the bone is eccentric.
The cortex is very thin and rises above the tumor.
A periosteal reaction is observed.
The lesion has a background of inhomogeneous structure, since the cartilage tissue contains many inclusions of bone.
Histological characteristics
Chondroblastoma is represented by a cartilaginous base, which includes cells of mature hyaline cartilage, as well as chondroblasts - embryonic unformed cells. The tumor has blood vessels, which distinguishes it from chondroma.
Differential diagnosis with chondrosarcoma: absence of cell atypia and polymorphism, mitoses and binucleate cells are rare, mucosal degeneration is not typical.

Figure 5. Tumor removal requires bone grafting.
Since the tumor also contains foci of bone tissue, it is necessary to carry out a differential diagnosis of chondroblastoma with neoplasms of bone tissue: osteochondroma, osteoblastoclastoma, osteogenic sarcoma.
The greatest difficulty is the differential diagnosis of the malignant form of this tumor. Detection of a periosteal reaction during an X-ray examination is often a diagnostic sign of cartilaginous or osteogenic sarcoma.
Treatment of chondroblastoma can only be surgical. During surgery, the pathologically altered area of bone tissue is excised within healthy tissue.
More up-to-date information on maxillofacial surgery is available in the section of our website called Maxillofacial Surgery Training .