
Accuracy of surgical templates with and without metallic sleeves in case of partial arch restorations: A systematic review
Abstract
Introduction: The aim of the present systematic review was to evaluate whether there were any differences in the three-dimensional accuracy and the implant survival rate of implants placed using computer-assisted planning and surgical templates with or without metallic sleeves.
Sources: This systematic review was written according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and registered to the PROSPERO (International prospective register of systematic reviews) database.
Study Selection: PICOS (population, intervention, control, outcomes, and studies) question was assessed, too. Search strategy encompassed the online (MedLine) literature from 1990 up to December 2020 published in English, and evaluating the accuracy of surgical templates with and without metallic sleeves in partial or complete patients. Only in vivo, randomized controlled trial and observational studies were included. Quality assessment of selected full text articles was performed according to the CONSORT (CONsolidated Standards of Reporting Trials) and STROBE (Strengthening the Reporting of Observational studies in Epidemiology) statement guidelines, respectively. For data analysis, the three-dimensional accuracy and the overall implant survival rate was calculated and compared between implants placed using surgical templates with or without metallic sleeves. Data: A total of 12 articles fulfilled the inclusion/exclusion criteria. Data from 264 patients with 614 implants were subjected to quality assessment (templates with metallic sleeves: 279 implants and 136 patients; templates without metallic sleeves: 335 implants and 128 patients). In all the three deviation parameters (angular, vertical, and horizontal), the differences in average accuracy were noticed (angular 2.33◦ ± 2.01◦ versus 3.09◦ ± 1.65◦, vertical: 0.62 ± 0.36 [mm] versus 0.95 ± 0.42 [mm]; and horizontal: 0.62 ± 0.41 [mm] and 1.11 ± 0.57 [mm]. No differences was found regarding overall implant survival rate (0.4891).
Conclusions: With the limitations of the present study, the surgical templates without metallic sleeves demonstrated high level of accuracy in all the three-dimensional measurements, when used to rehabilitate partially edentulous patients. Further randomized controlled trials, reporting according to the CONSORT guidelines are needed to confirm that the differences in accuracy depended on the type of used templates.
Introduction
Computer guided surgery is highly recommended for comprehensive diagnosis and prosthetically-driven implant planning. After that, the use of surgical template (or surgical guide) ensures an accurate implant placement, providing the highest probability of successful treatment outcomes, by reducing risk for technical and biological complications. Over the years, several researches, including prospective studies, randomized controlled trials, and systematic reviews, were written reporting an increasing level of accuracy of virtually planned/-template placed implants. Surgical template is defined as ‘a guide used to assist in proper surgical placement and angulation of dental implants’. The first type of surgical templates had metallic sleeves to drive surgical drills. Recently, surgical templates without metallic sleeves (or sleeveless templates) have been developed and introduced in the dental market, with the goal to make the guided surgery work-flow faster and easier. D’Souza divided available implant guides for (a) non-limiting (b) partially limiting and (c) completely limiting design. Nevertheless with almost 30 years of technological development in field of implant templates, today we can find three main kinds of digital implant templates designs also in the most advanced completely limiting design group: Guide with main metal sleeves, Guide without metal sleeves-plastic only and Open frame plastic or metal guide where not drills but the handpiece is driven by the template. With the development of 3D printing technologies, templates are recently available without metallic sleeves bonded into guide framework. Lack of metallic sleeves generate some advantages as cost reduction, less interdental space required and easier customization. But the question appears if this kind of sleeveless design offer the same accuracy as templates with metallic sleeves?
To the best of our knowledge, at the time of performing this systematic review, there were no other published reviews evaluating the newly developed surgical templates, designed with in-built, fully resin guides. The present review was written as a part of the 2nd Osstem AIC Italy Consensus Conference. Osstem AIC Italy is an independent, nonprofit, scientific community that provides implant education for members, including consensus conferences with founds received from membership. The aim of this consensus was to define the “Accuracy of Digital Technologies” in order to draw specific guidelines for the Osstem users. The present group was assigned the task to review the current knowledge regarding the accuracy of surgical templates with and without metallic sleeves. The focus question of the review was to evaluate whether there were any differences between implants placed using computer-assisted planning and surgical templates with or without metallic sleeves, regarding the three-dimensional accuracy of placed implants and the overall implant survival rate.
Methods
Study registration
The review protocol was registered in the PROSPERO International Prospective Register of Systematic Reviews hosted by the National Institute for Health Research, University of York (https://www.crd.york.ac.uk/prospero/), centre for Reviews and Dissemination, with an identification number (CRD42021229058).
Eligibly criteria
This systematic review was written according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (http://www.prisma-statement.org). Initially, the PICOS strategy (population [P], intervention [I], comparison [C], outcomes and study design [O], study type [S]) used to define the search was: P = Partial or complete edentulous patient treated with computer guided surgery; I = Guided implant placement (static computer-guided surgery) using surgical templates without metallic sleeves; C = Guided implant placement (static computer-guided surgery) using surgical templates with metallic sleeves; O = Implant accuracy, implant survival rate; S = Randomized controlled trials (RCTs), prospective and retrospective clinical trials (case-control studies, cohort studies, and case series). Articles were included in this systematic review if they met the following criteria: (1) human studies designed as randomized controlled clinical trials, case-control studies, cohort studies, and case series; (2) static computer-guided surgery using template with and/or without metallic sleeves; (3) reported as outcome measures the post-operative implant accuracy between the planning and placed implants; (4) and/or implant survival rate; (5) reported at least 10 cases. Moreover, only articles reporting data on implants placed using a fully guided approach were considered for this systematic review. Consequently, the exclusion criteria consisted of the following: (1) case reports or case series, animal studies, ex vivo and in vitro studies; (2) studies lacking measurable clinical outcomes; and (3) lack of objective data for comparing the study group outcomes.
Information sources and search strategy
Electronic and manual literature searches, conducted by two independent reviewers (MT and SMM), covered studies until December 2020 across the National Library of Medicine (MEDLINE by PubMed), using different combinations (and Boolean operators: AND, OR, NOT) of the following search terms/MeSH/keywords: (((Jaw, Edentulous[Mesh]) OR (Jaw, Edentulous, Partially[Mesh]) OR (Complete edentulism) OR (Partial edentulism)) AND ((Surgery, Computer-Assisted[Mesh]) OR (Guided Surgery) OR (Computer*)) AND ((Dental Implants[Mesh]) OR (implant*)) AND ((Accuracy) OR (Precision))). Filters applied: Abstract, Clinical Study, Clinical Trial, Comparative Study, Controlled Clinical Trial, Multicenter Study, Observational Study, Pragmatic Clinical Trial, Randomized Controlled Trial, Humans, English. Additionally, previous systematic reviews investigating guided implant surgery were also screened for possible article identification. Finally, a manual and complete search of related journals was conducted until December 2020, including Clinical Implant Dentistry and Related Research, Clinical Oral Implants Research, Clinical Oral Investigations, Dentistry Journal, Materials (including special issues), International Journal of Oral & Maxillofacial Surgery, Journal of Prosthetic Dentistry, Journal of Prosthodontic Research, Journal of Prosthodontics, The International Journal of Oral & Maxillofacial Implants, The International Journal of Periodontics & Restorative Dentistry, The International Journal of Prosthodontics.
Data extraction
Two reviewers, MT and SMM, independently extracted data from the included studies. Disagreements were again resolved through discussion until a consensus was reached between both reviewers. Where data were unclear or incomplete, the authors of the publication were contacted for further explanation. The data were further analyzed based on the following subgroups: metallic versus plastic sleeves and beginner versus expert.
Quality of the studies
The same reviewers assessed the quality of the studies, and the risk of bias for the included studies using a modification of the guidelines provided by the Consolidated Standards of Reporting Trials (CONSORT) statement, for the evaluation of RCTs (http://www.consortstatement.org;), the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement, for observational studies (http://www.strobe-statement.org), and the modified items from the Cochrane Collaboration Tool for assessing risk of bias. For the adequacy of the respective studies, the items were graded and the percentage of negatively graded items was calculated to define the overall risk of bias. Quality assessment was performed in 2 different phases: in phase I, quality assessment was based on the published full-text articles performed independently by the two reviewers; in phase II, disagreements were resolved with discussion. After collecting the scores of quality assessment at phase II, an overall estimation of plausible risk of bias (low, moderate, or high) was completed for each selected study. A low risk of bias was estimated when all the criteria were met, expect one; a moderate risk was considered when maximum three criteria were not met or partially met; and a high risk of bias was estimated when more than three criteria were not met or partially met (Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0; http://www.cochrane.org/resources/handbook).
Outcomes and analysis of the results
The primary outcome measure of this systematic review was the final accuracy of virtually planned implants. Three deviation parameters (angular, vertical, and horizontal) were defined and calculated between the planned and placed implant positions by superimposition of the postoperative data with the preoperative implanting planning. The implant survival rate, as reported by the studies, was considered the secondary outcomes.
Statistical analysis was done using a specialized analytical package, Medical Kit (Statistica, StatSoft Polska, Cracow, Poland). For data visualization Microsoft office Excel was used (Microsoft Corporation, Redmond, Washington, US). Following parameters were selected for analysis:
- Angular deviation – given in degrees: represents the value of the angle between the central axis of the planned and placed implant.
- Error in depth – given in millimeters: represents the differences in depth (vertical) between the planned and placed implants.
- Error at entry point – given in millimeters: represents the horizontal displacement of site preparation between the planned and placed implants.
- All measurements were presented as mean plus minus standard deviation (SD). The selected studies were clustered in partially and completely edentulous patients, and then grouped, based on the type of surgical guide which were tested:
- Surgical guides with metallic sleeves – group: metallic.
- Surgical guides without metallic sleeves (sleeveless) – group: plastic. The odds ratio (OR), its standard error and 95% confidence interval was used to calculate differences in the proportions of implant failures between implants placed with and without metallic sleeves (dichotomous outcomes). Forest plot arrays point was used to estimates (e.g., mean) and confidence intervals (e.g., 95% CI) three-dimensional accuracy for included studies, summarizing previously published findings. A statistician with expertise in dentistry performed the analysis.
Results
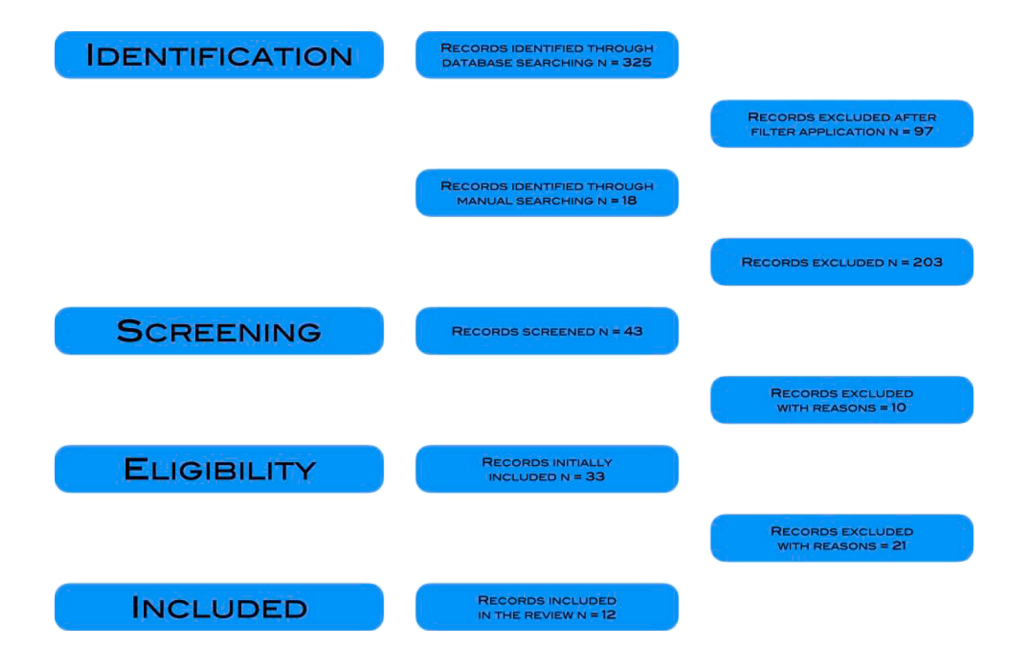
Initially, the electronic database search on PubMed and Gray literature resulted in 325 manuscript. After filters application (abstract, study design, humans, English language.) 97 articles were excluded, resulting in a total of 228 manuscripts. An additional 18 articles were identified with manual searches (previous systematic reviews and gray literature taught internet and personal contacts) yielding a total of 246 articles were available for screening. Of these, 43 articles were finally selected for full-text review by the two reviewers. Most of the manuscripts were excluded as they reported data on dynamic dental implant navigation system, zygomatic implants, orbital Implants, orthodontic mini implants. After application of the inclusion and exclusion criteria, 10 articles were excluded with reasons. Of these, four articles were in vitro, three manuscripts had no correct data acquisition, and others three involved less than 10 patients. After prescreening evaluation of the remained 33 manuscripts, none of these reported data of complete edentulous patients treated with surgical template without metallic sleeves. It was decided to excluded the cluster of complete edentulous patients, including only teeth-supported template used for the treatment of partially edentulous patients. Therefore, a further 21 studies were excluded, resulting in 12 manuscripts selected for inclusion (Fig. 1).
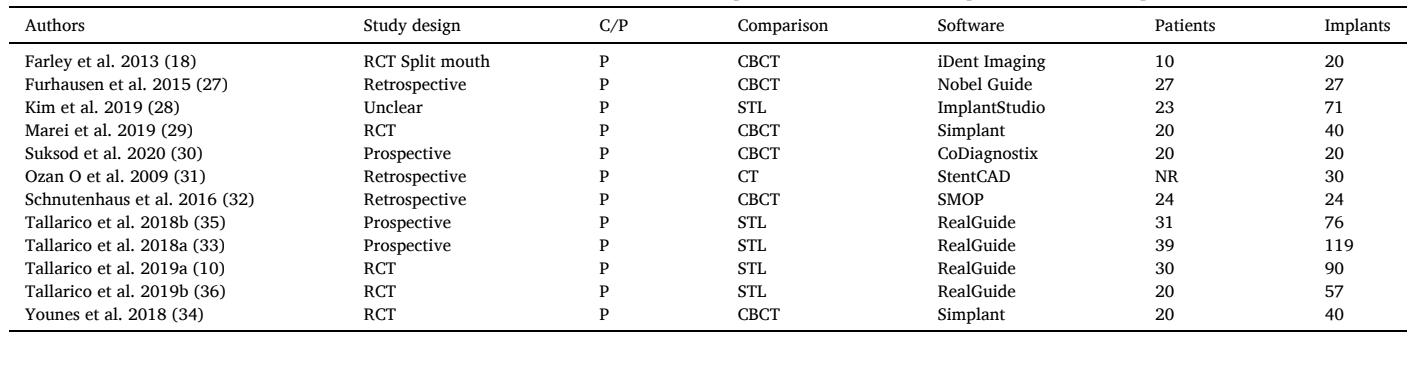
A total of 12 articles were included for qualitative synthesis and assessment. Of these, four studies reported data only of surgical template without metallic sleeves; only one randomized controlled trial reported data of both; while, eight manuscript reported data on surgical templates with metallic sleeves. Overall, two studies, one randomized controlled trial and one comparative prospective study reported data of expert versus beginners. Nevertheless, only one of these reported data using surgical template without metallic sleeves, and the second reported data using only surgical template with metallic sleeves. The characteristics of the included studies are reported in the Table 1.
Overall, data from 264 patients (data from 11 out of 12 articles) with 614 implants were analyzed. Of these, 279 implants on 136 patients were placed using surgical templates with metallic sleeves, while 335 implants on 128 patients were installed using surgical template without metallic sleeves. Quality of the available data and differences in measurement method did not allow to conduct a full meta-analysis.
Quality of the studies
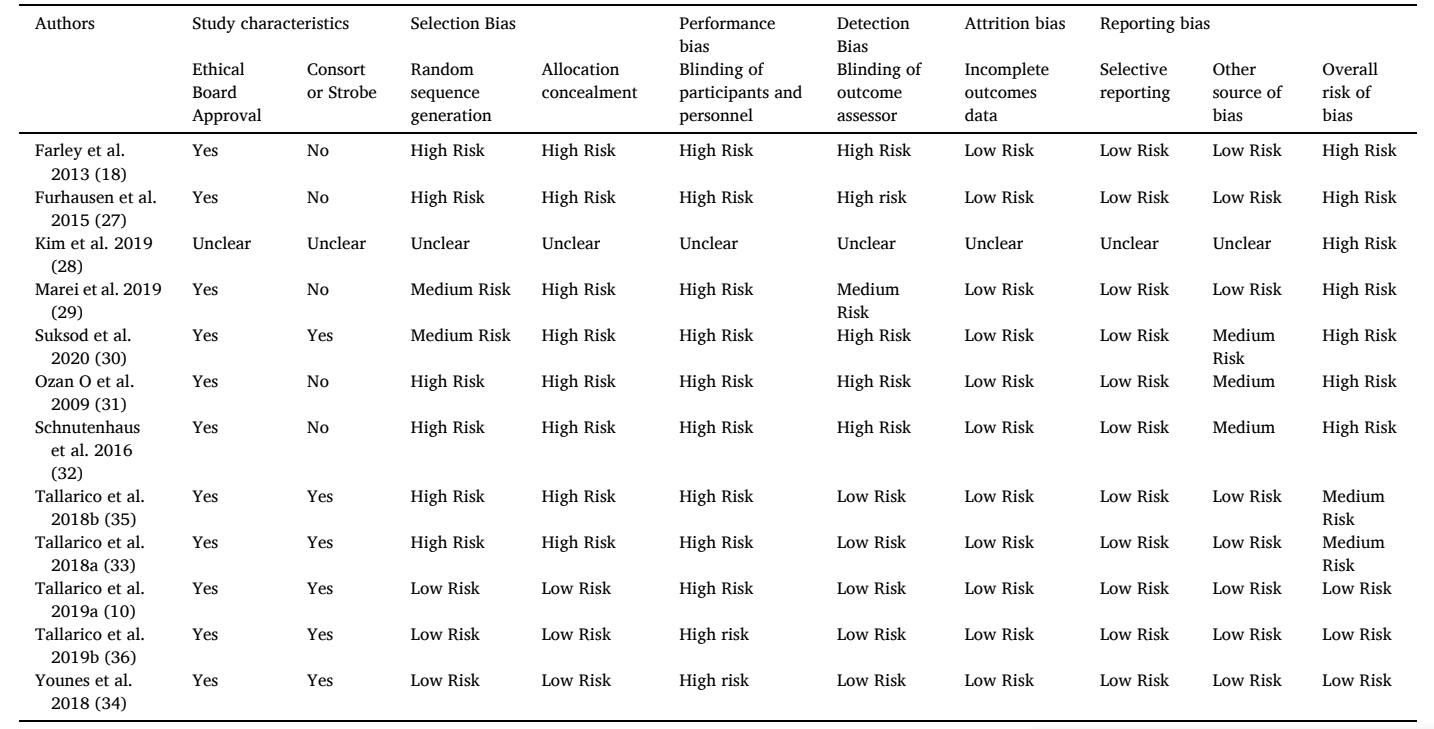
The 12 selected studies were published from 2009 to 2020. Of these, five articles were RCTs with a parallel-group design; three were prospective studies, two of these involved a single cohort, while the other one is a comparative prospective evaluation; three articles were with a retrospective design; and in the last case, the study designed was unclear. None of the selected human studies fulfilled all the requisites (Table 2). However, a positive figure was that all the research, expect one, received an Ethical Board Approval. Overall, seven studies were a high risk of bias, two were a medium risk, and only three were a low risk of bias. All of these are randomized controlled trial. The other included articles received minimum grading for selection and performance bias, including randomization procedures and blinding of the participants.
Accuracy
All the included articles reported data on accuracy (Table 3.). In seven studies the accuracy was evaluated by matching the postoperative CT or CBCT scan with the data extrapolated from the virtual implant planning. In the other five studies, the final implant position was evaluated by using the STL files derived from a digital intraoral impression taken immediately after implant placement. Only one randomized controlled trial compared the accuracy of placed implants with and without metallic sleeves.
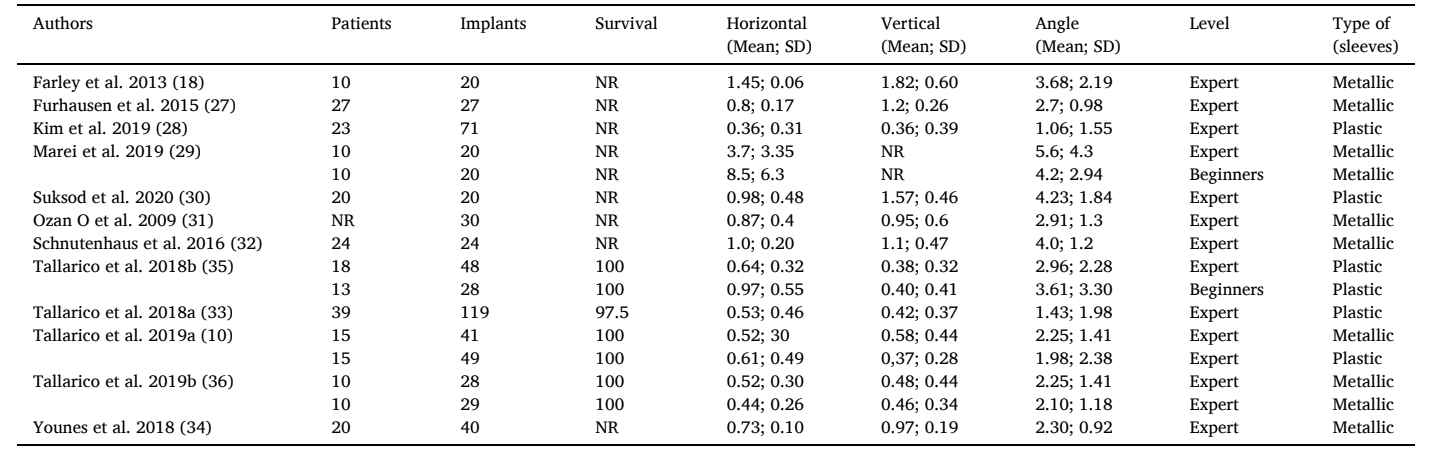
Comparison of angular deviation reported in analyzes studies is showed on the forest plot (Fig. 2). The mean angular deviation was lower in group of implant placed with surgical templates without metallic sleeves, rather than in group of implants placed using surgical guides with metal sleeves – respectively: 2.33◦ ± 2.01◦ versus 3.09◦ ± 1.65◦.
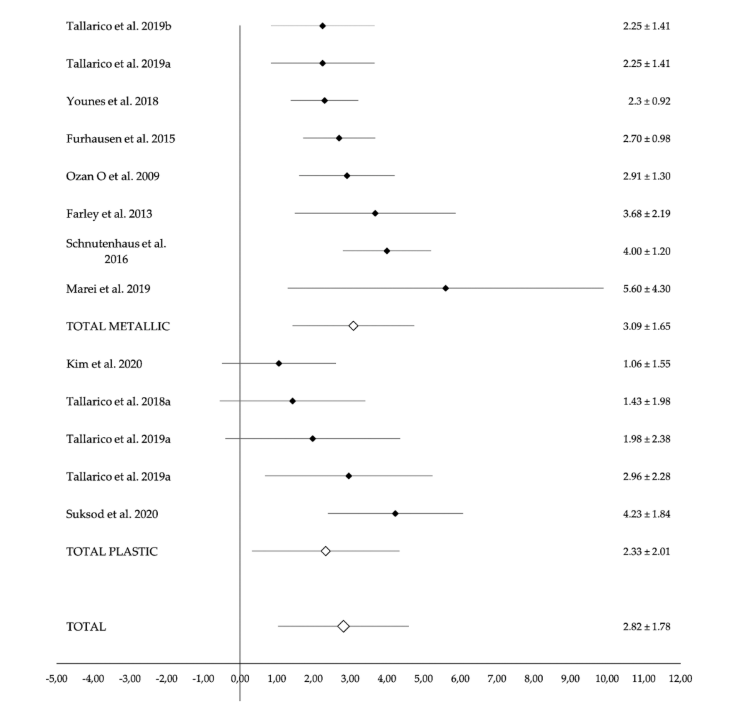
Fig. 3 shows the mean differences in depth (vertical) of implant placement for each of selected studies. The results was more like between groups: 0.62 ± 0.36 [mm] for implants placed with surgical guides without metallic sleeves and 0.95 ± 0.42 [mm] for implants placed with surgical template with metallic sleeves.
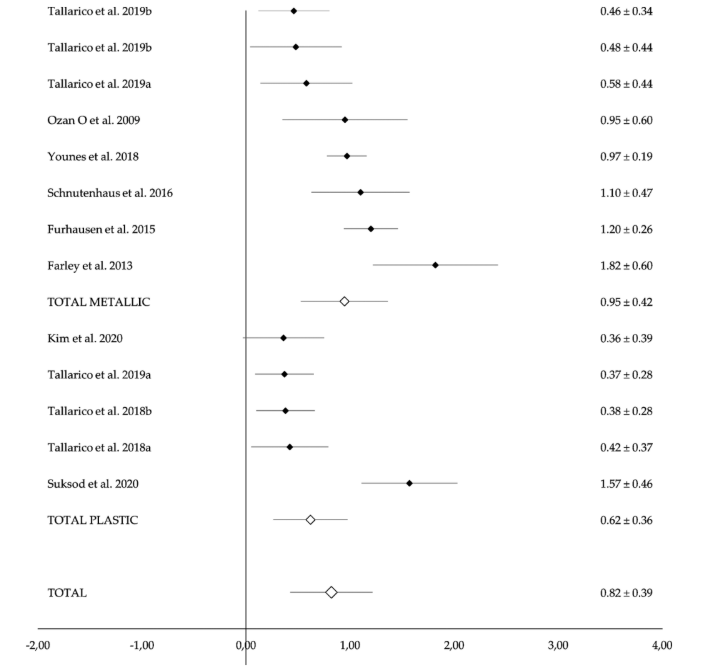
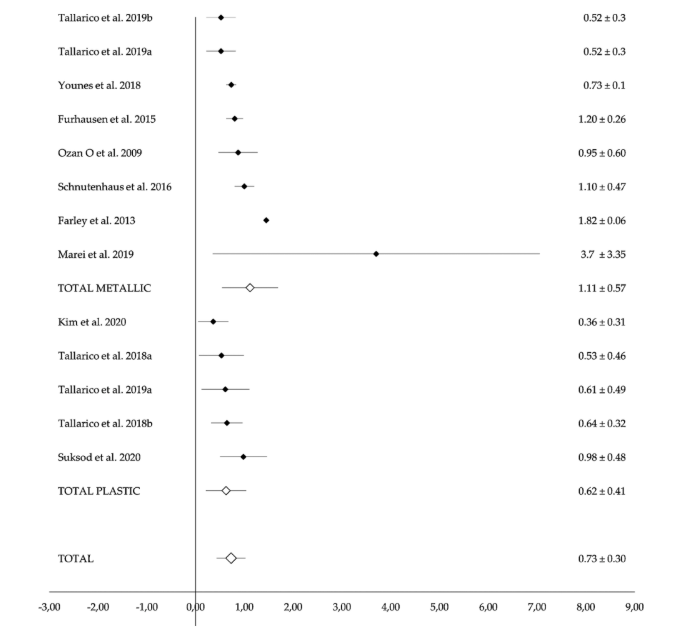
Fig. 4 clearly demonstrates the differences between groups in the horizontal placement of implant, at the entry point. The deviations in the group of surgical guides without metallic sleeves are lower than in group of surgical guides with metal sleeves – respectively: 0.62 ± 0.41 [mm] and 1.11 ± 0.57 [mm].
Four studies reported data on survival rate. Overall, three out of 244 implants failed when placed with templates without metallic sleeves, and none out of 98 implants failed in the other group (metallic sleeves). Difference was not statistically significant (P = 0.4891; Odds ratio 0.3503; 95% CI: 0.0179 to 6.8442). When analyzed individually, three randomized controlled trials reported 100% of survival rate for all the tested group, including templates with and without metallic sleeves, expert versus beginners using templates without metallic sleeves, and digital and analog workflow in combination with templates with metallic sleeves[10]. The fourth study analyzed 119 implants placed in 39 patients, reporting three implant failures experienced before prosthesis delivery. The mean survival rate was 97.5% evaluated in follow-up period ranging from 3 to 24 months after definitive loading. In all of the other studies the follow-up was not available due to the nature of the primary outcome (only implant accuracy).
Discussion
The purpose of this systematic review was to evaluate whether there were any differences between implants placed using computer-assisted planning and surgical templates with or without metallic sleeves, regarding the three-dimensional accuracy of placed implants and the overall implant survival rate.
Unfortunately, the original PICOS question was not fully respected, since there was no studies reported the accuracy of placed implants with surgical template without metallic sleeves, in complete edentulous patients. However, with the limitation of the present research, and in partial edentulous patients, the implants placed using surgical guides without metallic sleeves, seems to be more accurate than same procedures performed with surgical guides with metal sleeves, in all the three deviation parameters. Comparing application of templates with or without metallic sleeves it is important to analyze preparation of these different designs. Cassetta et al. found, placing a prefabricated metal sleeve within the template can induce an error itself during the fabrication of a surgical guide. Metal sleeve guides often are use with additional reduction sleeves for each drill in the sequence. Double the clearance margins between the main sleeve and reduction sleeve for particular drill and between the reduction sleeve and the drill can result in inaccuracies during surgery. Therefore, three-dimensionally printed surgical guides with in-built nonmetal sleeves of small diameter have been suggested by Schneider et al. for reducing lateral drill movements and instrument tolerances. Moreover, incorporating metal sleeve into 3D printed frame may need up to one mm more interdental space to design the guide. This fact can make some limitations clinically when limited interdental space is available, e.g. pre- molars or lower incisors sites. It is also important that when plastic only, 3D printed guide frame is used as a surgical template the device and 3D printing technology used for its manufacturing may be a key point for the accuracy. Another factor important for accuracy of guided surgery are proportions and distances. The higher the guiding part of the template is and the shorter drill is used the higher accuracy may be achieved.
Within this systematic review the greatest inaccuracy was found in the angular deviation. Tallarico et al., in a randomized controlled trial reported a statistically significant higher accuracy in angle and vertical plan in case of implants placed with surgical templates without metallic sleeves, when compared with implants placed with conventional surgical guide with metallic sleeves. A possible confounding factor derived from the study of Marei et al. that reported a high standard deviation of the results. Nevertheless, although error in depth was not reported in this study, same differences in accuracy for different types of surgical templates were reported.
Another benefit of the plastic templates is that the in-build sleeves can be customized. Open side holes can be printed allowing for a fully guided implant placement even in case of short mouth opening. In a prospective multicenter clinical trial conducted by Tallarico et al., although great accuracy was found in all the parameters measured, open sleeves templates were less accurate, particularly in angle deviation. It is the author’s opinion that open sleeves should be used with caution in the molar region and only in case of reduced inter-arch space. The higher accuracy of the surgical template without metallic sleeves might be connected firstly with the quality of surgical guide, including high quality of printing machine, as well as, dedicate resin materials. Nevertheless, the main benefits of plastic templates is that they can be fully customized before printing, avoiding any misfit with adjacent hard of soft tissue, as well as, improving the guidance between the implant drills and the surgical template itself.
In the present systematic review, no statistically significant difference was found regarding the implant survival rate, nevertheless, all the included study presented a short follow-up. Further study with longer follow-up are needed to confirm this results.
This systematic review presented several limitations. First of all, no articles was found reporting accuracy or survival rate of implants placed with surgical templates without metallic sleeves in complete edentulous patients. For the latter, the results of this systematic review can be apply only in partial edentulous patients. The second limitation was the heterogeneity of the included study. The main differences were the study design and the method to compare the accuracy of the placed implants. Seven studies used the DICOM files derived from the post-operate CT or CBCT scan, while, the other five studies used the STL files derived from an intraoral impression. Moreover, eight different implant planning software were used. Nevertheless, despite all the limitations, on 614 implants placed in 264 patients were reported in the qualitative analysis, allowing to draw some conclusions.
Previous systematic reviews with meta-analysis focused on the accuracy of guided surgery comparing partial versus complete edentulous patients, as well as, different surgical protocols, such us fully guided, pilot drill guidance, and free-hand approach. Tahmaseb et al. concluded that the accuracy of static computer-aided implant surgery is within the clinically acceptable range in the majority of clinical situations, including partial and complete arch restorations. There is no doubt that computer-assisted / template-based implant placement allow to higher accuracy in all the clinical scenarios. In two comparative studies, higher accuracy can be expected also when the implants were placed by inexpert clinicians. Cassetta et al. also demonstrated that the learning curve could be reduced when a static computer-assisted implant surgery was used. However, it is the authors’ opinion that a safety margin of 2 mm must to be always recommended, particularly for beginners. In another systematic review, Gargallo-Albiol et al. concluded that a fully guided approach has the highest accuracy, followed by half-guided surgery. The same systematic review and meta-analysis also demonstrated that the freehand implant placement provides the least accuracy. It is important to underline that computer-assisted, template-based implant placement need not necessarily be performed using a flapless approach. Unfortunately, this is non-scientific. In case of complex clinical scenario, reduced keratinized tissue, and/or safety margins of less than 2 mm, the authors suggest a combined approach including flap elevation and guided implant placement. The main benefits of guided surgery remain the improved accuracy and predictability, according to a pre-established prosthetic plan, as well as, easier immediate loading procedures. It also help to avoid nearby anatomical structure, take advantages from the residual bone volume. Moreover, the surgical templates without metallic sleeves are the possibility to be customized, the potentially lower cost, and the possibility to be used in narrow space and limited mouth opening. All of these benefits are of great importance, particularly, but not limiting to anterior area and complete arches restorations, which requires very careful case selection and high surgical skill levels, especially if high esthetic outcomes are to be achieved.
A possible limitation of surgical template without metallic sleeves, is that the drills work very close to the resin, potentially transporting some resin dust inside the implant site. Nevertheless, the present systematic review failed to find any significant difference in survival rate between groups. A possible explanation is that the characteristics of surgical template materials are wear‑resistant, compared with previous templates. In fact, biocompatible Class I material, developed for the printing of surgical templates must be used. On the other hand there is also o shift in drills design. Recent drills have a smooth guiding part which stays in contact with the tracking part of the printed template. Active part of that kind of drill does not touch the template material. Nevertheless, wash of the implant site with sterile saline before implant placement should be recommended. More randomized controlled trials with longer follow-up are needed to confirm this preliminary results regarding survival rate.
Conclusions
With the limitations of the present systematic review, the surgical templates without metallic sleeves demonstrated a high level of accuracy in all the three-dimensional measurements. This preliminary results can be applied only in partial edentulous patients due to the lack of data regarding accuracy of implant placed using surgical template without metallic sleeves to rehabilitate complete edentulous patients. Data on the survival rates must be interpreted with caution due to the short follow-up period. Further randomized controlled trials, reported according to the CONSORT guidelines, are needed to confirm this preliminary results.
Marco Tallarico, Marta Czajkowska, Marco Cicciù, Francesco Giardina, Armando Minciarelli, Łukasz Zadrożny, Chang-Joo Park, Silvio Mario Meloni
References
- M. Tallarico, S.M. Meloni, Retrospective Analysis on Survival Rate, Template- Related Complications, and Prevalence of Peri-implantitis of 694 Anodized Implants Placed Using Computer-Guided Surgery: results Between 1 and 10 Years of Follow-Up, Int. J. Oral & Maxillofac. Implants 32 (5) (2017).
- M. Tallarico, M. Esposito, E. Xhanari, M. Caneva, S.M. Meloni, Computer-guided vs freehand placement of immediately loaded dental implants: 5-year postloading results of a randomised controlled trial, Eur J Oral Implantol 11 (2) (2018) 203–213.
- A. Tahmaseb, V. Wu, D. Wismeijer, W. Coucke, C. Evans, The accuracy of static computer-aided implant surgery: a systematic review and meta-analysis, Clin. Oral. Implants Res. 29 (Suppl 16) (2018) 416–435.
- N. Van Assche, M. Vercruyssen, W. Coucke, W. Teughels, R. Jacobs, M. Quirynen, Accuracy of computer-aided implant placement, Clin. Oral. Implants Res. 23 (Suppl 6) (2012) 112–123.
- J.Y. Park, Y.W. Song, S.H. Park, J.H. Kim, J.M. Park, J.S. Lee, Clinical factors influencing implant positioning by guided surgery using a nonmetal sleeve template in the partially edentulous ridge: multiple regression analysis of a prospective cohort, Clin. Oral. Implants Res. 31 (12) (2020) 1187–1198.
- P. Tack, J. Victor, P. Gemmel, L. Annemans, 3D-printing techniques in a medical setting: a systematic literature review, Biomed. Eng. Online 15 (1) (2016) 115.
- A. Louvrier, P. Marty, A. Barrabé, E. Euvrard, B. Chatelain, E. Weber, C. Meyer, How useful is 3D printing in maxillofacial surgery? J Stomatol Oral Maxillofac Surg 118 (4) (2017) 206–212.
- M. Javaid, A. Haleem, Current status and applications of additive manufacturing in dentistry: a literature-based review, J Oral Biol Craniofac Res 9 (3) (2019) 179–185.
- M. Colombo, C. Mangano, E. Mijiritsky, M. Krebs, U. Hauschild, T. Fortin, Clinical applications and effectiveness of guided implant surgery: a critical review based on randomized controlled trials, BMC Oral Health 17 (1) (2017) 150.
- M. Tallarico, M. Martinolli, Y. Kim, F. Cocchi, S.M. Meloni, A. Alushi, E. Xhanari, Accuracy of Computer-Assisted Template-Based Implant Placement Using Two Different Surgical Templates Designed with or without Metallic Sleeves: a Randomized Controlled Trial, Dent J (Basel) 7 (2) (2019).
- G. Van de Wiele, W. Teughels, M. Vercruyssen, W. Coucke, A. Temmerman, M. Quirynen, The accuracy of guided surgery via mucosa-supported stereolithographic surgical templates in the hands of surgeons with little experience, Clin. Oral. Implants Res. 26 (12) (2015) 1489–1494.
- Ł. Zadrożny, M. Czajkowska, E. Mijiritsky, L. Wagner, Repeatability of Freehand Implantations Supported with Universal Plastic Sleeves-In Vitro Study, Int J Environ Res Public Health 17 (12) (2020).
- M. Tallarico, F.M. Ceruso, L. Muzzi, S.M. Meloni, Y.-.J. Kim, M. Gargari, M. Martinolli, Effect of simultaneous immediate implant placement and guided bone reconstruction with ultra-fine titanium mesh membranes on radiographic and clinical parameters after 18 months of loading, Materials (Basel) 12 (10) (2019) 1710.
- J. Gargallo-Albiol, S. Barootchi, J. Marques-Guasch, H.-.L. Wang, Fully Guided Versus Half-Guided and Freehand Implant Placement: systematic Review and Meta-analysis, Int. J. Oral Maxillofac. Implants 35 (6) (2020).
- M. Tallarico, A.I. Lumbau, R. Scrascia, G. Demelas, F. Sanseverino, R. Amarena, S. M. Meloni, Feasibility of Using a Prosthetic-Based Impression Template to Improve the Trueness and Precision of a Complete Arch Digital Impression on Four and Six Implants: an In Vitro Study, Materials (Basel) 13 (16) (2020) 3543.
- A.o. Prosthodontics, The glossary of prosthodontic terms, Mosby 1999.
- K.M. D’Souza, M.A. Aras, Types of implant surgical guides in dentistry: a review, J. Oral Implantol. 38 (5) (2012) 643–652.
- N.E. Farley, K. Kennedy, E.A. McGlumphy, N.L. Clelland, Split-mouth comparison of the accuracy of computer-generated and conventional surgical guides, Int. J. Oral Maxillofac. Implants 28 (2) (2013).
- M. Tallarico, M. Caneva, N. Baldini, F. Gatti, M. Duvina, M. Billi, G. Iannello, G. Piacentini, S.M. Meloni, M. Cicciù, Patient-centered rehabilitation of single, partial, and complete edentulism with cemented-or screw-retained fixed dental prosthesis: the First Osstem Advanced Dental Implant Research and Education Center Consensus Conference 2017, Eur J Dent 12 (04) (2018) 617–626.
- D. Moher, A. Liberati, J. Tetzlaff, D.G. Altman, P. Group, Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement, PLoS Med. 6 (7) (2009), e1000097.
- K.F. Schulz, D.G. Altman, D. Moher, CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials, Trials 11 (1) (2010) 1–8.
- E. Von Elm, D.G. Altman, M. Egger, S.J. Pocock, P.C. Gøtzsche, J. P. Vandenbroucke, S. Initiative, The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies, Int. J. Surg. 12 (12) (2014) 1495–1499.
- F. Graziani, E. Figuero, D. Herrera, Systematic review of quality of reporting, outcome measurements and methods to study efficacy of preventive and therapeutic approaches to peri-implant diseases, J. Clin. Periodontol. 39 (2012) 224–244.
- J.P. Higgins, D.G. Altman, P.C. Gøtzsche, P. Jüni, D. Moher, A.D. Oxman, J. Savović, K.F. Schulz, L. Weeks, J.A. Sterne, The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials, BMJ 343 (2011).
- J.P. Higgins, J. Thomas, J. Chandler, M. Cumpston, T. Li, M.J. Page, V.A. Welch, Cochrane Handbook for Systematic Reviews of Interventions, John Wiley & Sons, 2019.
- M. Cumpston, T. Li, M.J. Page, J. Chandler, V.A. Welch, J.P. Higgins, J. Thomas, Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions, Cochrane Database Syst. Rev. 10 (2019), ED000142.
- R. Fürhauser, G. Mailath-Pokorny, R. Haas, D. Busenlechner, G. Watzek, B. Pommer, Esthetics of flapless single-tooth implants in the anterior maxilla using guided surgery: association of three-dimensional accuracy and pink esthetic score, Clin. Implant Dent. Relat. Res. 17 (2015) e427–e433.
- L.S. Kim YJ, Digital workflow for implant dentistry, 2019 Tokyo OFF-LINE, 2019.
- H.F. Marei, A. Abdel-Hady, K. Al-Khalifa, H. Al-Mahalawy, Influence of surgeon experience on the accuracy of implant placement via a partially computer-guided surgical protocol, Int. J. Oral Maxillofac. Implants 34 (5) (2019).
- N. Suksod, C. Kunavisarut, J. Kitisubkanchana, Accuracy of computer-guided implantation in the placement of one-piece ceramic dental implants in the anterior region: a prospective clinical study, PLoS One 15 (9) (2020), e0237229.
- O. Ozan, I. Turkyilmaz, A.E. Ersoy, E.A. McGlumphy, S.F. Rosenstiel, Clinical accuracy of 3 different types of computed tomography-derived stereolithographic surgical guides in implant placement, J. Oral Maxillofac. Surg. 67 (2) (2009) 394–401.
- S. Schnutenhaus, C. Edelmann, H. Rudolph, R.G. Luthardt, Retrospective study to determine the accuracy of template-guided implant placement using a novel nonradiologic evaluation method, Oral Surg Oral Med Oral Pathol Oral Radiol 121 (4) (2016) e72–e79.
- M. Tallarico, Y.J. Kim, F. Cocchi, M. Martinolli, S.M. Meloni, Accuracy of newly developed sleeve-designed templates for insertion of dental implants: a prospective multicenters clinical trial, Clin. Implant Dent. Relat. Res. 21 (1) (2019) 108–113.
- F. Younes, J. Cosyn, T. De Bruyckere, R. Cleymaet, E. Bouckaert, A. Eghbali, A randomized controlled study on the accuracy of free-handed, pilot-drill guided and fully guided implant surgery in partially edentulous patients, J. Clin. Periodontol. 45 (6) (2018) 721–732.
- M. Tallarico, M. Martinolli, M. Abadzhiev, F. Cocchi, Y.-.J. Kim, A safe and predictable treatment option for experts and beginners, EDI Journal 14 (3) (2018) 52–57.
- W. Zhou, Z. Liu, L. Song, C.L. Kuo, D.M. Shafer, Clinical Factors Affecting the Accuracy of Guided Implant Surgery-A Systematic Review and Meta-analysis, J Evid Based Dent Pract 18 (1) (2018) 28–40.
- K.C. Oh, J.M. Park, J.S. Shim, J.H. Kim, J.E. Kim, J.H. Kim, Assessment of metal sleeve-free 3D-printed implant surgical guides, Dent. Mater. 35 (3) (2019) 468–476.
- G.R. Deeb, R.K. Allen, V.P. Hall, D. Whitley, D.M.Laskin 3rd, S. Bencharit, How Accurate Are Implant Surgical Guides Produced With Desktop Stereolithographic 3-Dimentional Printers? J. Oral Maxillofac. Surg. 75 (12) (2017) 2559.e1–2559.e8.
- K. El Kholy, S.F. Janner, M. Schimmel, D. Buser, The influence of guided sleeve height, drilling distance, and drilling key length on the accuracy of static Computer-Assisted Implant Surgery, Clin. Implant Dent. Relat. Res. 21 (1) (2019) 101–107.
- A. Keßler, V. Le, M. Folwaczny, Influence of the tooth position, guided sleeve height, supporting length, manufacturing methods, and resin E-modulus on the in-vitro accuracy of surgical implant guides in a free end situation, Clin. Oral. Implants Res. (2021).
- K.C. Oh, J.-.M. Park, J.-.S. Shim, J.-.H. Kim, J.-.E. Kim, J.-.H. Kim, Assessment of metal sleeve-free 3D-printed implant surgical guides, Dent. Mater. 35 (3) (2019) 468–476.
- M. Cassetta, F. Altieri, M. Giansanti, M. Bellardini, G. Brandetti, L. Piccoli, Is there a learning curve in static computer-assisted implant surgery? A prospective clinical study, Int. J. Oral Maxillofac. Surg. 49 (10) (2020) 1335–1342.
- M. Tallarico, R. Scrascia, M. Annucci, S.M. Meloni, A.I. Lumbau, A. Koshovari, E. Xhanari, M. Martinolli, Errors in implant positioning due to lack of planning: a clinical case report of new prosthetic materials and solutions, Materials (Basel) 13 (8) (2020) 1883.
- S.M. Meloni, Accuracy of computer-assisted template-based implant placement using conventional impression and scan model or intraoral digital impression: a randomised controlled trial with 1 year of follow-up, Int J Oral Implantol (Berl) 12 (2) (2019) 197–206.
- M. Cassetta, A. Di Mambro, M. Giansanti, L.V. Stefanelli, C. Cavallini, The intrinsic error of a stereolithographic surgical template in implant guided surgery, Int. J. Oral Maxillofac. Surg. 42 (2) (2013) 264–275.