
Extra-long implants (20, 22, and 25 mm) for fixed implant-supported total rehabilitation
Machine translation
Original article is written in PT language (link to read it) .
Introduction
The use of dental implants to improve the quality of life of patients has been widely published in Dentistry. The use of extra-long implants in fixed implant-supported total rehabilitation offers patients improvements in chewing, comfort, aesthetics, and phonetics. The use of this type of implant reduces treatment time and cost compared to other modalities of conventional implant treatments. The literature reports favorable parameters in hard tissues and molds for both axial and angled implants.
Very high success rates have been reported in 10-year studies for the mandible and five years for the maxilla. The use of angled implants allows for the avoidance of complicated anatomical structures and maximizes the A-P distance in total rehabilitation, also allowing for the avoidance of highly complex bone grafts, increasing the acceptance of treatment plans by patients. The use of extra-long implants allows for easier achievement of immediate function, as the anchorage of the implants will be located in anatomical areas of greater bone density, meaning there is high primary stability in low-density maxillary bone with bicortical anchorage using extra-long implants (20, 22, and 25 mm).
Clinical case
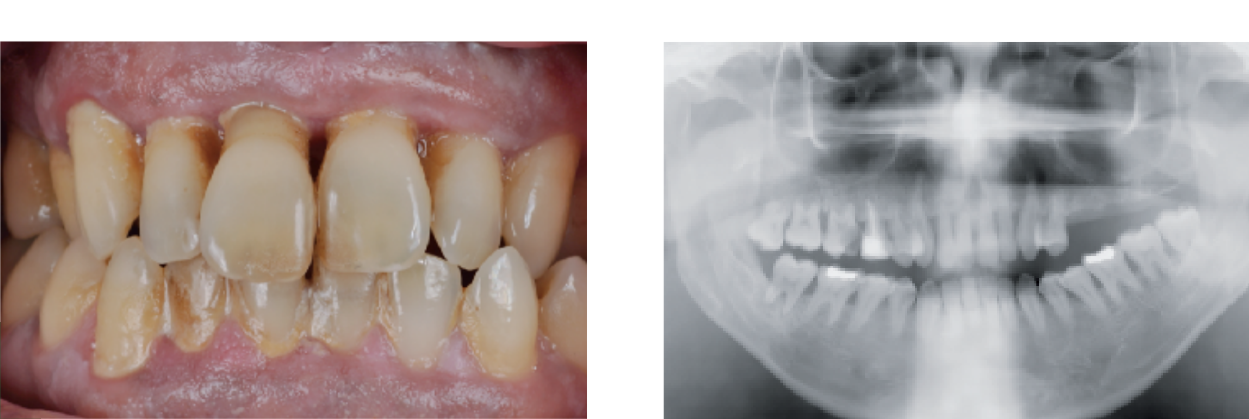
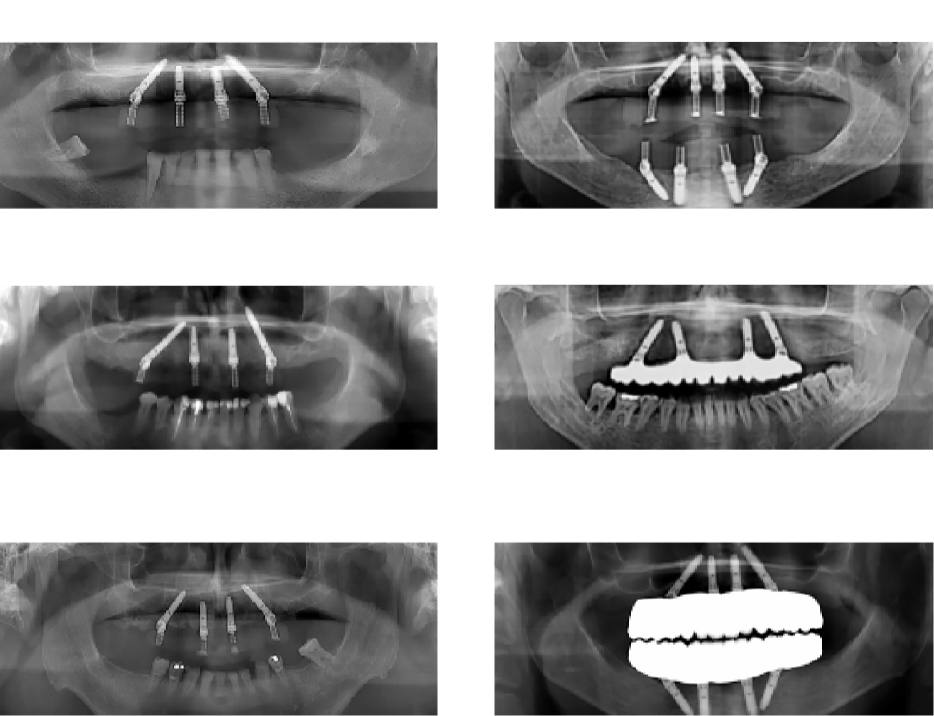
A 47-year-old male patient, smoker, with no relevant medical history, presents to the consultation with mobility of all teeth in the upper jaw. He sought definitive treatment because "the teeth were always shaking." After a pre-treatment evaluation (medical history and patient complaints, dental history, radiographic analyses, intraoral and extraoral examination, and treatment plan), periodontal treatment was performed and extraction of all dental pieces in the upper jaw was proposed, with immediate placement of four implants and a fixed provisional restoration on the day of surgery. After six months, a fixed prosthesis with a Nobel Procera implant bridge, made of layered zirconia with ceramic, was placed.
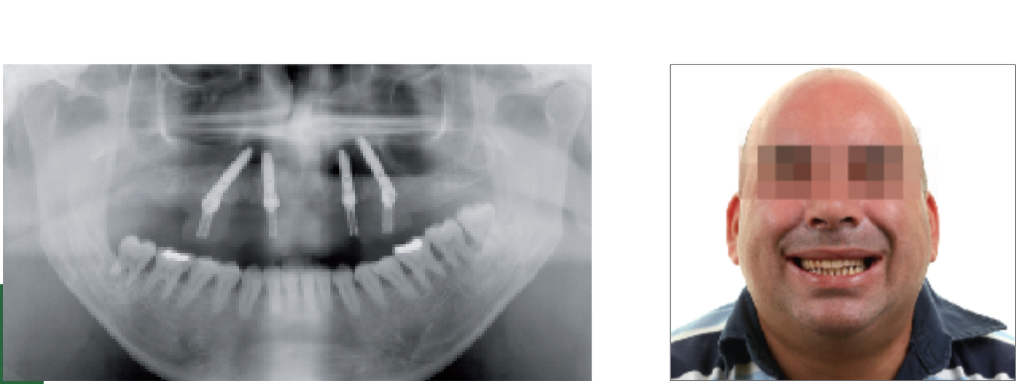
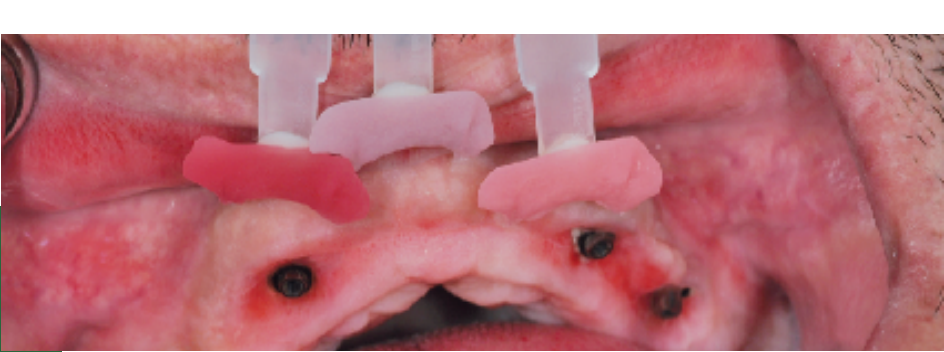
During the dental implant placement surgery, local-regional anesthesia was performed, and all dental pieces in the upper jaw were extracted. The four implants placed were Nobel Speedy, with the anterior ones being axial at 18 mm and the posterior ones angled at 20 mm. Primary stability was greater than 35 N. Subsequently, angled posterior and straight anterior multi-unit abutments were placed, and a provisional acrylic fixed prosthesis was installed on the day of surgery.
The healing occurred over six months without any significant negative aspects.
After this period, final rehabilitation was carried out, starting from the duplication of the immediate acrylic prosthesis, which was mounted on an articulator to maintain the same vertical dimension.
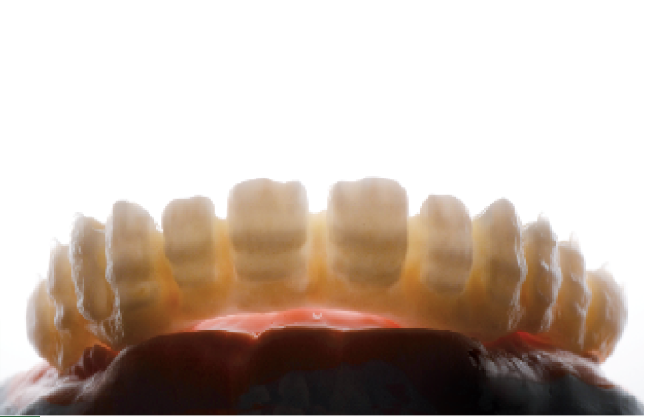
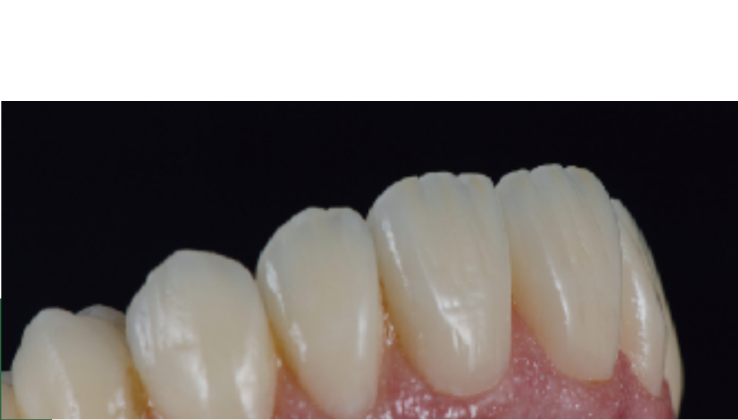
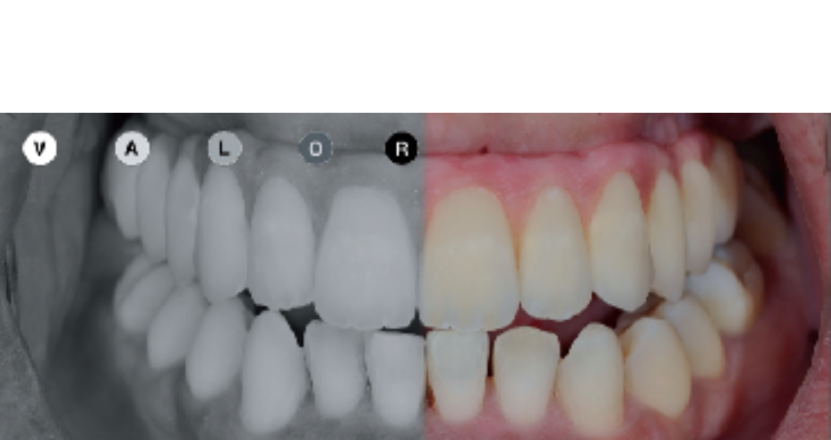
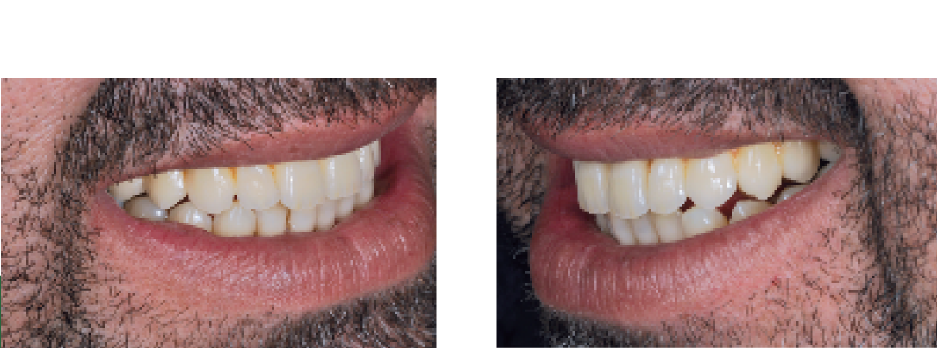
After a consultation for the approval of a try in model, the final rehabilitation was performed with a Nobel Procera bridge made of layered zirconia.
Discussion/conclusion
The literature reports very high rates in total implant-supported rehabilitation with four dental implants. The use of extra-long implants seems to allow for greater primary stability in maxillary bone with low density through bicortical anchorage, as it allows access to anatomical areas with better quality and bone density, although there are no studies for long implants (20, 22, and 25 mm).














João Mouzinho, Catarina Vitorino, Pedro Brito
Bibliography
- Weinstein R, Agliardi E, Fabbro MD, Romeo D, Francetti L. Immediate rehabilitation of the extremely atrophic mandible with fixed full-prosthesis supported by four implants. Clin Implant Dent Relat Res 2012; 14: 434-41.
- Mozzati M, Arata V, Gallesio G, Mussano F, Carossa S. Immediate post-extractive dental implant placement with immediate loading on four implants for mandibular full-arch rehabilitation: a retrospective analysis. Clin Implant Dent Relat Res 2013; 15: 332-40.
- Babbush CA, Kanawati A, Kotsakis GA, Hinrichs JE. Patient-related and financial outcomes analysis of conventional full-arch rehabilitation versus the All-on-4 concept: a cohort study. Implant Dent 2014; 23: 218–24.
- Babbush CA. Posttreatment quantification of patient experiences with full-arch implant treatment using a modification of the OHIP-14 questionnaire. J Oral Implantol 2012; 38: 251-60.
- Francetti L, Romeo D, Corbella S, Taschieri S, Del Fabbro M. Bone level changes around axial and tilted implants in full-arch fixed immediate restorations. Interim results of a prospective study. Clin Implant Dent Relat Res 2012; 14: 646-54.
- Malo P, de Araujo Nobre M, Lopes A, Francischone C, Rigolizzo M. All-on-4 immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes. Clin Implant Dent Relat Res 2012;14 Suppl 1:e139-50.
- Malo P, de Araujo Nobre M, Lopes A, Moss SM, Molina GJ. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. J Am Dent Assoc 2011; 142: 310-20.
- Balshi TJ, Wolfinger GJ, Slauch RW, Balshi SF. A retrospective analysis of 800 Brånemark system implants following the All-on-Four™ protocol. J Prosthodont. 2014 23: 83-8.