Digital Workflow in Oral Rehabilitation
Machine translation
Original article is written in PT language (link to read it) .
In this second article, we will address the digital workflow in oral rehabilitation. With the evolution of technology in Dentistry, we can nowadays use machines and systems for diagnosis, as we discussed in the first article. After diagnosis and planning, the digital workflow allows our oral rehabilitation to be more predictable, easier in production, and optimized in the time of the work performed, but also with greater comfort and direct participation from the patient in the work, for a higher approval from them. These advantages allow for more rigorous work, in accordance with the patient's expectations.
The use of the intraoral scanner has improved the patient experience by eliminating the need for traditional impression materials, with the possibility of visualizing potential errors at the moment of scanning, which can be erased and rescanned through the intraoral scanner for a more positive result. 3D printing has also allowed for the faster acquisition of physical models with great definition, enabling dental clinics to access all types of models and guides for digital oral rehabilitation.
The digital execution is more predictable, due to the visualization of a possible final result through the prior planning of the dental prosthesis, with a high initial investment, but with a reduction in costs in the long term.
We will give special emphasis to the execution of prosthetic rehabilitation and its stages, with the digital impression, and the computer-aided design and manufacturing systems, CAD--CAM.


One of the simplest and most basic applications is rehabilitation on natural teeth, from inlays, onlays, crowns, ceramic veneers, etc. Sometimes, in analog treatments, the cumulative error for the final result was significant, from the dental preparation that could not be confirmed in the impression, but only in the final model, to the impression that could have distortions, leading to a final result different from what the patient expected. Nowadays, we can directly see the results of our preparations in the intraoral scanner, identify directional errors, see lack of prosthetic space, perform color mapping, or even observe dynamic occlusion with the patient in the chair, which in the past was only observed after the work was already in the dental laboratory. In this clinical case, we present a case of three ceramic veneers and one ceramic crown, made through a digital workflow, where scanning and digital printing made the work more predictable, without associated trials.
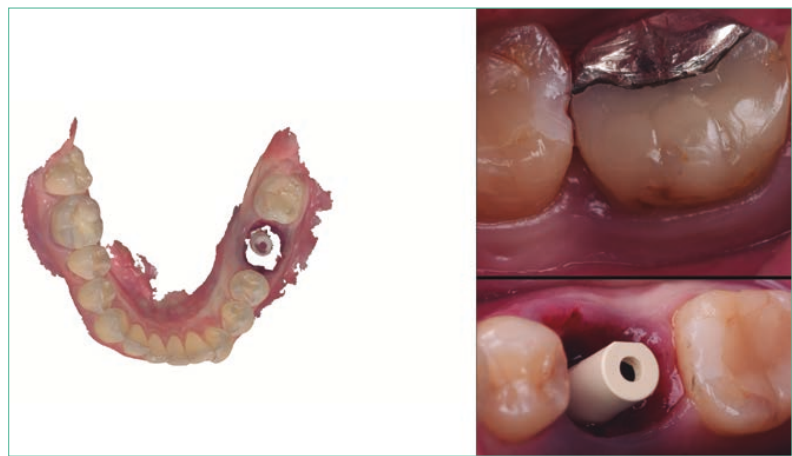
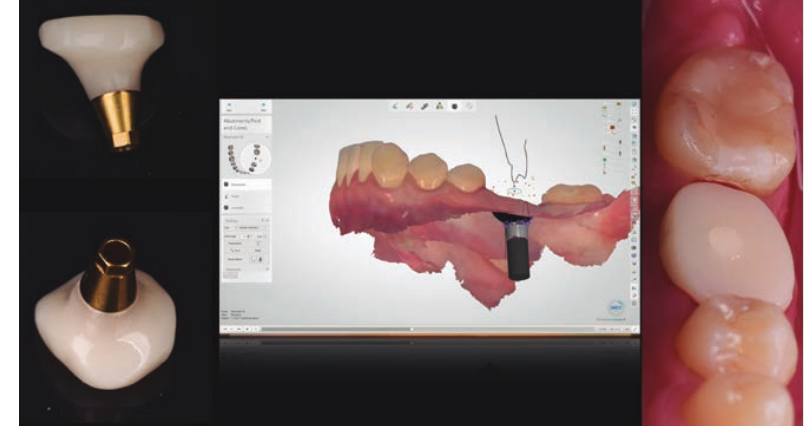
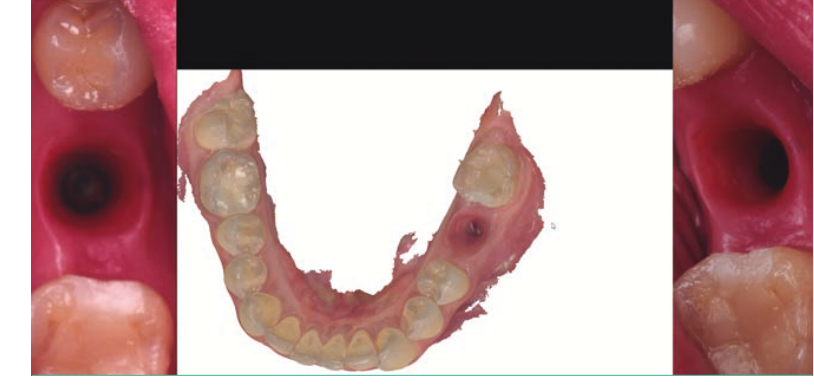
In digital implant-supported rehabilitation, there have been many advances in the field of implantology. One of the first steps after placing the implant would be the fabrication of a temporary tooth or, in some cases, the placement of a healing abutment. With the digital workflow, we can immediately during the surgery fabricate a healing abutment, customized and adapted to the socket of the tooth we just extracted, which allows for a more stable maintenance of the gum architecture of the tooth, using materials with a more biological behavior like the one we presented in this case, with a titanium and PMMA abutment, which allowed for the maintenance of the shape of the extracted molar tooth during the three months of gum healing.



Interdisciplinarity in oral rehabilitation and the use of different materials has always made mixed cases (rehabilitation on natural teeth and dental implants) complex. Nowadays, these cases have become simpler, as they can be copied before surgery, incorporating the mock-up for provisional rehabilitation, as well as for final rehabilitation.
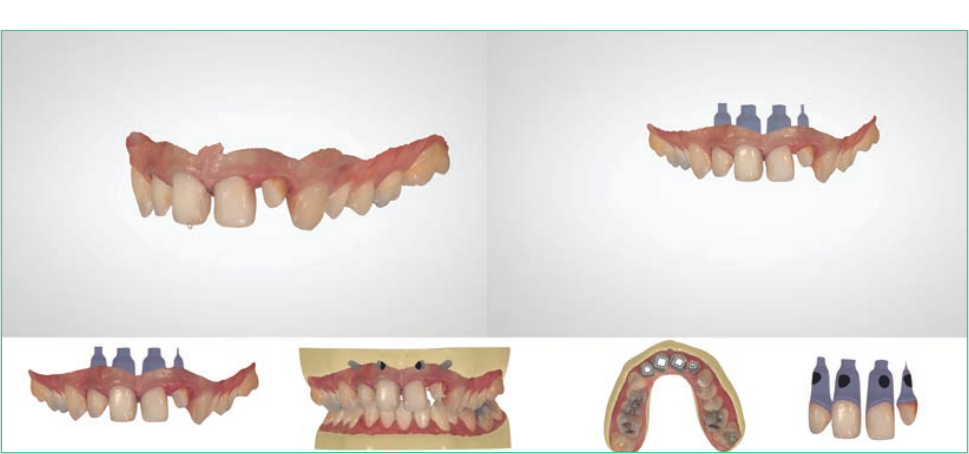
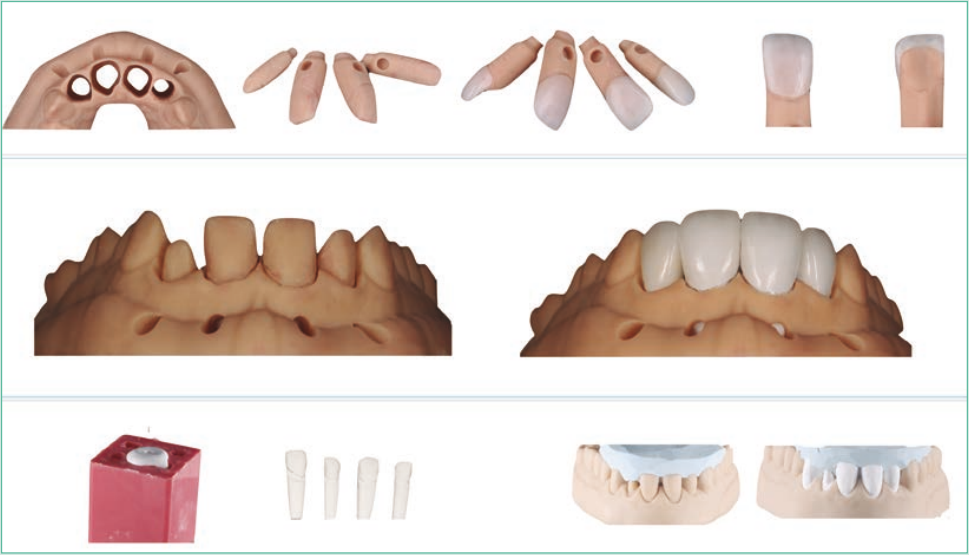
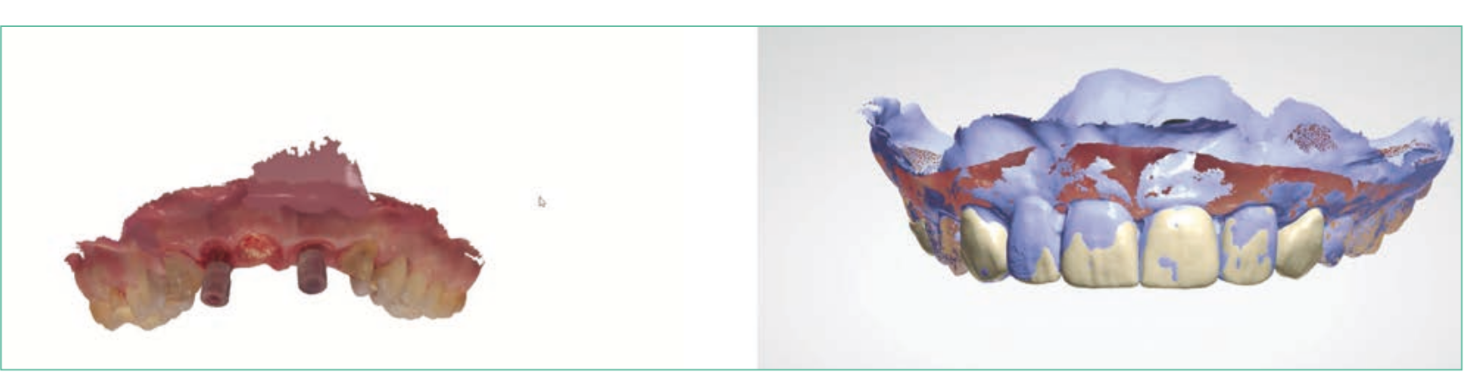
In this clinical case, the patient lost an anterior bridge, and on the day of the surgery, implants, crowns, and provisional veneers were placed in a digital workflow, which was then copied for the final rehabilitation in ceramic. The 3D design software (in this case, 3Shape) allows for the combination of all images, such as initial situation, 3D design, implant positions, and dental preparation positions in a predictable manner, to achieve an ideal final result.





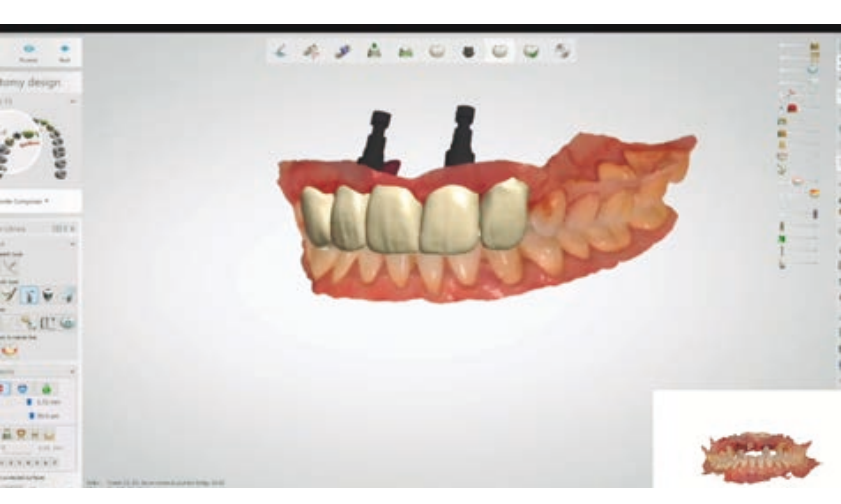
In total rehabilitations on implants, the great difficulty has always been the creation of a digital immediate load. In this case, one of the strategies used was the maintenance of four teeth during the total implant surgery, to be able to combine the images in the immediate load design software (initial image, 3D design, implant position, and future immediate load), allowing on the day of the surgical procedure the creation of a totally digital fixed complete prosthesis, with the ideal position in the Smilecloud design (which we addressed in the first article), plus the dental and occlusal position stipulated before the surgery, plus the final position of the placed dental implants. At the end of the surgery, we managed to place a fixed complete prosthesis in CAD-CAM milled PMMA over six dental implants.

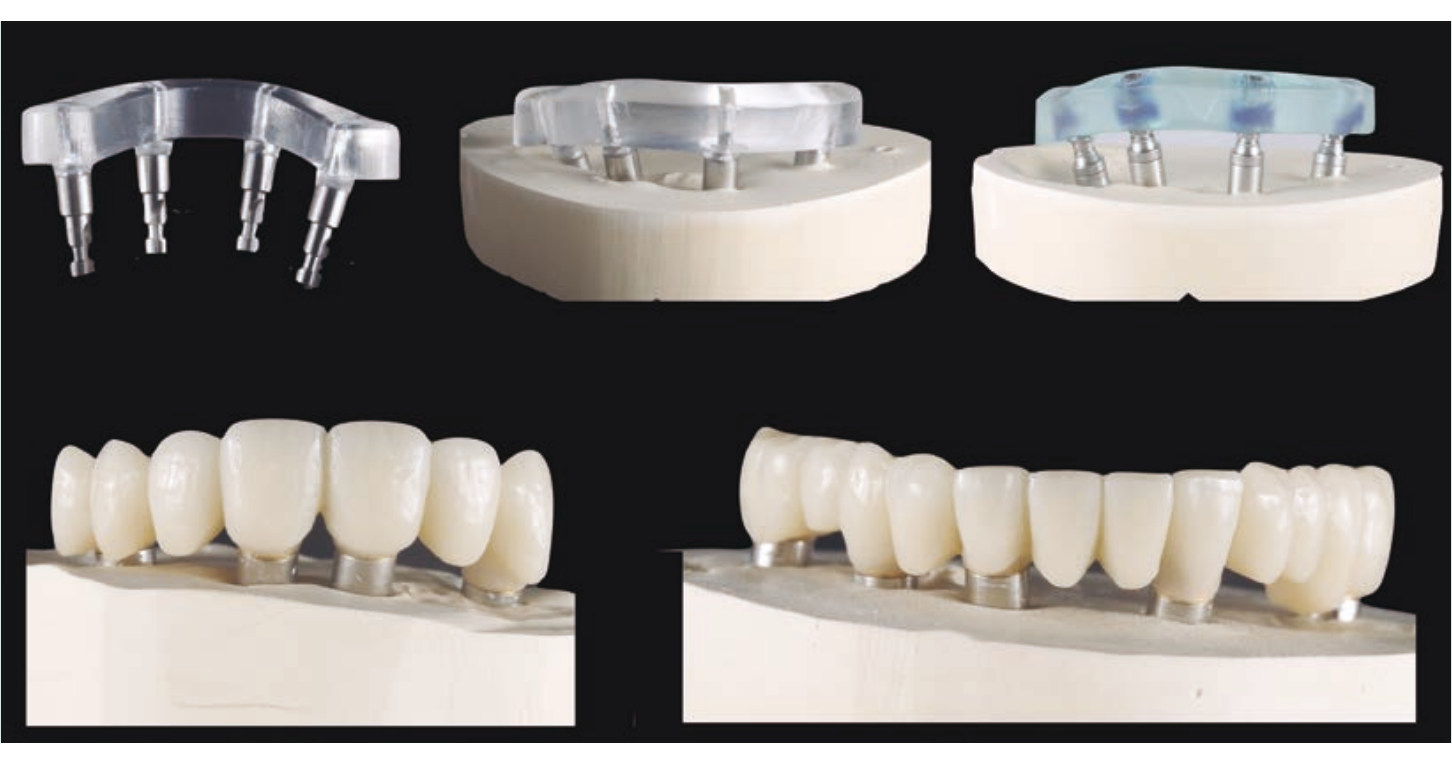
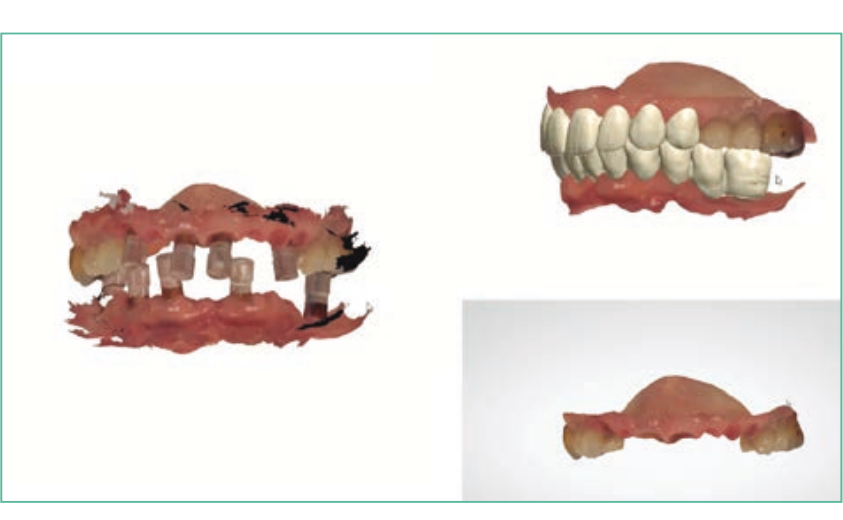

The process of creating total fixed ceramic prostheses on implants elevates the digital to the most complex level. The difficulty of creating passive structures is due to the challenge of fully scanning edentulous arches, where the error becomes cumulative. This is perhaps the Achilles' heel of intraoral scanning. One of the strategies is to save the initial files from the immediate loading, so that they can be overlaid in the definitive rehabilitation, with only the need to scan the gingival modification that occurred during the period of osseointegration of the implants. In the presented case of definitive bimaxillary rehabilitation in zirconia, the files from the scanbodys used in the immediate loading were saved to construct a passive fit. After the passive fit was approved, scans of the gingival tissue were performed for the fabrication of the final bimaxillary rehabilitation in zirconia.