
Proposal of relevant values for use in cephalometric studies of the local population
Machine translation
Original article is written in ES language (link to read it) .
Summary
Due to the frequent lack of alignment between the clinical picture presented by the patient and the cephalometric diagnosis obtained by applying the Schwarz Cephalogram, it was decided to corroborate the basis of the values originally published by the author, in relation to a population considered representative of individuals of growth age in the Argentine Republic with the aim of generating a protocol with values adapted to our population.
A random sample of 615 children was taken, from whom a lateral cephalometric radiograph was obtained. After performing the cephalometric tracing of it, it was subjected to Schwarz's analysis, according to the CECLAC program.
Matches were found in the measurements of the angle of inclination of the maxilla and the sizes of the maxillary and mandibular bodies, and discrepancies of varying degrees in the other measured aspects.
After analyzing the obtained data, we obtained a set of values that more accurately reflect the predominant biotype, which is a slightly elongated face and a slightly more convex profile.
Introduction
In our daily clinical task, dedicated to restoring the health of our patients, we have encountered more than once a discrepancy between what the clinical analysis of our patient showed and what the cephalometric study indicated.
Having historically used the Schwarz cephalogram, our teacher, Dr. Miguel Ángel Cacchione, had already attempted to make some interpretation that would bridge this gap, (mainly concerning the interbasal angle).
Faced with the same problem a generation later, we set out to scientifically confront the values obtained from an adult population of Central Europe, whose results were published by Arthur Martin Schwarz in the late 1950s, with the actual values of an Argentine population in growth ages.
At least since the 20th century, cephalometry has become the main aid for the orthodontist and functional orthopedist when arriving at a diagnosis; an aid that, being the sum of a series of objective data, allows for a certain evaluation of the treatment's evolution throughout the process.
This auxiliary has traversed the last century and continues into the present with varying fortunes, depending on the schools and trends, going through all stages, from being given an absolute value to an anecdotal value.
What has been constant is that this set of measurements, mostly taken from classical anthropometry, has become a reference point as a body of statistical values emerging from studies conducted in populations that were never national, but rather European or North American.
Due to the harmony that Schwarz seeks to find between the sizes and positions of the different cranio-maxillofacial structures of the same individual, it has been the body of measurements that we have typically chosen from the long hundred cephalograms available to the orthodontist.
Objectives
- To obtain, based on a sample of the Argentine population in growth ages, the average cephalometric values comparable to those obtained by Schwarz.
- To corroborate whether the same relationships between some of these measurements (linear and angular) are repeated, as published by the aforementioned author.
- To describe the predominant biotype in our population, to correlate it with other cephalometric studies.
- To describe the variation of the data according to age.
Materials and Methods
The sample was taken from the population of the city of Neuquén, province of Neuquén, Argentina. This city exhibits exponential growth, being a recipient of immigrants from other provinces. Initially, there is a strong influence from the original inhabitants of the region, to which migrations with a strong presence of traits from indigenous populations from other regions of the country have been added, as well as other migratory currents that arrived from other continents. These characteristics lead us to consider the Neuquén population representative of Argentina.
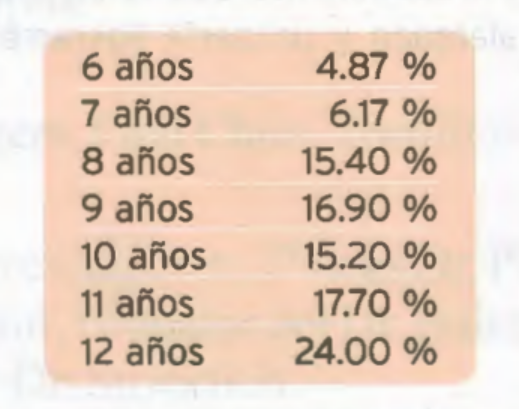
The sample consists of 615 children, aged between 6 and 12 years, randomly selected, who presented for dental consultation between the years 1995 and 2004, distributed by age, as shown in Table I.
The Schwarz Cephalogram was performed on cephalometric casts made by the same professional in lateral head teleradiographs using the CECLAC system.
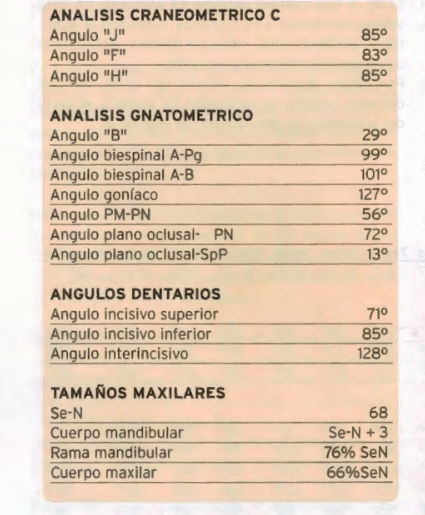
This author divides his analysis into a cranometric study and a gnatometric study.
In a superficial, merely indicative description, we can say that: cranometry studies the inclination and position of the maxilla in relation to the anterior cranial fossa, as well as the vertical position of the TMJ in relation to the middle cranial fossa; while gnatometry mainly informs us about the anteroposterior and vertical relationships between both maxillae, as well as the inclination of the mandible concerning the anterior cranial fossa. A valuable piece of information is also related to sizes, seeking harmony or the lack thereof among the different structures of the cranio-maxillofacial skeleton.
Finally, it proposes a study of the profile, from which we must highlight the possibility of predicting the patient's profile once the dysgnathia has been overcome.
Results
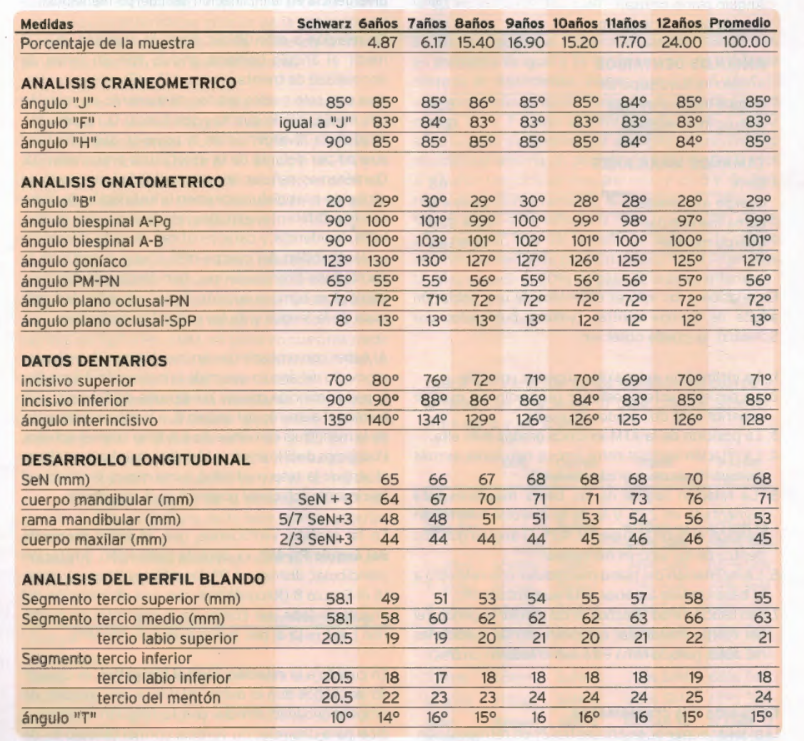
In relation to the values obtained from an adult population in Central Europe, (values published by Schwarz), it can be observed:
- The inclination of the maxilla coincides.
- The average anteroposterior position of the maxilla is two degrees retruded.
- The position of the TMJ is five degrees higher.
- The vertical relationship between both maxillae is more divergent. (nine degrees greater)
- The sagittal relationship of the maxillary bases is increased by 2.7º, and that of the lower alveolar in relation to the maxilla is 4.7º. The gonial angle is within normal values.
- The inclination of the mandibular plane with respect to the anterior cranial base is increased by 9º.
- Regarding sizes, the maxilla and the mandibular body match the author's measurements, but the ramus is increased by 5%
Discussion
Regarding cranometry.
The maxilla is 2º in retroposition, although its size is normal, and we want to emphasize that the inclination matches the measurements taken by the author.
The ATM, which reflects the position of the middle cranial fossa, is five degrees higher.
Regarding gnathometry.
We will first address the vertical relationship between both maxillae, and we will observe that, on average, we have an increase of 9º, if we accept that the author provides an average norm of 20°. If we take into account that the inclination of the upper maxilla is normal, we must locate the responsibility for this divergence in the inclination of the mandibular body.
In relation to the latter, it is noteworthy that when measuring the gonial angle, an angle with a normal range of thirty degrees (123±15), we find only four degrees of increase in relation to the mean, so we must seek the responsibility for the divergence in the position adopted by the body in front of the pre-masseteric notch. We would like to point out the responsibility that has been attributed to dysfunctions in the establishment of this break. Different studies related to the etiology, incidence, and characteristics of this difference in the direction of the mandibular body from the pre-masseteric notch have implicated etiological factors such as digital sucking and abnormal activity of the tongue and orofacial muscles.
Having verified that in our sample, the average value of the angle measuring the inclination of the maxilla coincides with Schwarz's measurements, we attribute the increase in angle B to the greater inclination of the mandible with respect to the anterior cranial base. We could say in other terms, perhaps more graphically, that we attribute the responsibility to a greater tendency for posterior rotational growth of the mandible.
In this sense, we verified that the average value of the angle Pn-MP, that is, the inclination or mandibular rotation, decreased by 9º, the same 9º that angle B increased (Let us remember that a decrease in the angle should be read as a greater posterior rotation. See footnote, point a, angle PN-MP).
Regarding the sagittal bimaxillary relationship, it is known to all that the author establishes a direct proportionality relationship with the vertical relationship, and states: for a normal vertical relationship (angle B) of 20º, a sagittal relationship (Maxillo-mandibular, MM) of 90º corresponds, and for every 10º that B increases, MM must be 7º.
When we conducted our measurement, we found an average value for B of 29º, and for MM of 99º. If we took Schwarz's analysis as a basis, the value of MM should be 96.3°, therefore, we must say that our population has a profile 3º more convex than that on which the author conducted his measurements.
This last data does not surprise us, as the anterior rotational growth is recognized as one of the characteristics of the central European population, a trait that does not repeat in the same proportion within the local population.
Regarding the relationship established by Schwarz, where every 10° of variation of angle B should have a directly proportional variation of 7° of angle MM, in our measurements, starting from an angle B of 29º and an MM of 99º, there is a one-to-one relationship, that is, for every degree that B varies, MM also varies by one degree, and in a directly proportional manner.
The other angle that the author uses to measure the sagittal relationships between both maxillae is the SpP-AB, taking the lower alveolar process as the reference point. For the author, the normal value is the normal of SpP-APg, or MM, while in our measurements there is a difference of +2º indicating a greater flattening of the anteroinferior alveolar region.
Regarding the size of the jaws we see that the size of the mandibular body is still 3mm longer than the distance between Se and N., while we find that the ramus is 596 longer than the measurement proposed by the author, since in the original measurements, the size of the ramus should correspond to 71% of the size of the anterior cranial base.
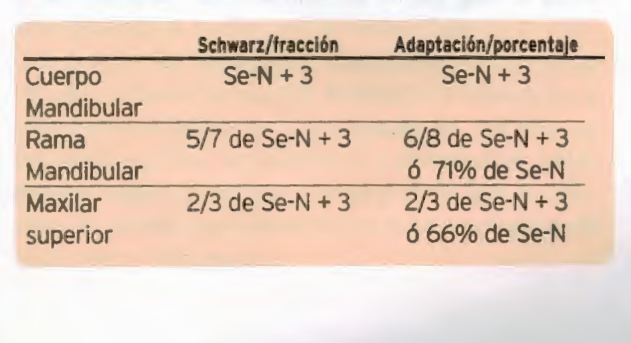
As can be seen, there is a match in the correspondence of the sizes that Schwarz proposes for the mandibular and maxillary sizes, although not for the size of the ramus. We would like to draw attention to the correspondence that is verified between the greater length of the ramus and the greater height of the medial cranial fossa.
The length of the body of the maxilla is equal to the ratio proposed by Schwarz.
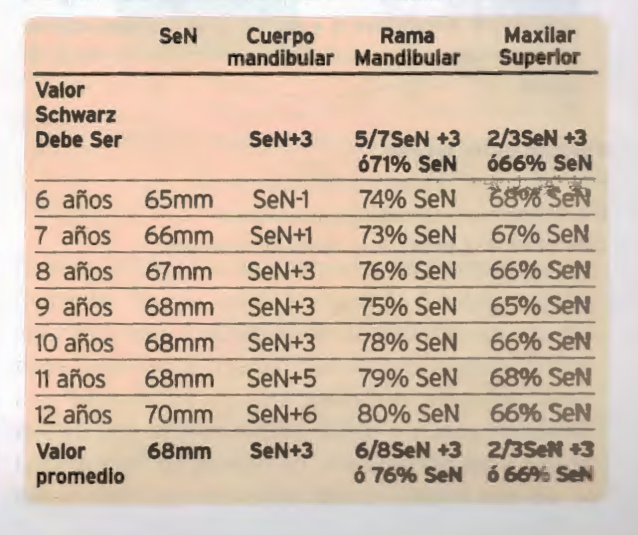
When dividing the sample into age groups, we find that these values are not constant throughout growth.
Thus, while the size of the mandibular body, on average, is equal to Se-N +3mm, it is not so throughout all growth. We see that at 6 years old, the average value is equal to the cranial base size minus 1mm. And then it increases until it reaches 12 years old when it is 6mm greater than this; mandibular growth alternates a period of activity between 6 and 7 years with another of rest between 8 and 10 years, resuming again between 11 and 12 years.
Regarding the size of the mandibular ramus, at 6 years old it measures 74% of the size of the anterior cranial base, gradually increasing until it reaches 80% of the anterior cranial base at 12 years old.
Conclusions
By making the measurements described by Schwarz on a representative local population group, we found the repetition of some values and the non-coincidence of others.
The coincidences are in the inclination of the upper jaw, and in the sizes of the mandibular and maxillary bodies.
The variations have appeared in the other analyzed data, and they have allowed us to develop a body of data that is harmonious with the clinical findings.
We have achieved a reference protocol regarding the biotype of our population in growth ages. Statically, we offer the average data between 6 and 12 years (Table III), and in a dynamic view, we conduct an analysis according to the age group, which will be submitted for the reader's consideration in a future publication.
Silvia Galetti, Graciela I. Lorenz
Bibliographic
- Schwarz AM. The roentgenostallk-Urban 6 Scharzenberg Vienna, 1958.
- Castellino A. Hercules Provera Romén Santini. Transcript of "Cephalometry in Orthodontic Diagnosis" First Edition - 1956 Editorial La Médica Rosario – Argentina
- Galetti S. Adaptation of the Schwarz Cephalogram to the population of the city of Neuquén. Research work. Specialist course in Orthodontics I.A.C.O. Neuquén - Argentina 2006.
- Zielinsky L. Methodology for cephalometric analysis as a basis for staged decisions. Rev Ateneo Argent Odontol 1987; 22(2):2t-38.
- Dung D. Smith. R. Cephalometrics and Clinical Diagnoses of open bite tendency. American Journal of Orthodontics 1988; 484-490.
- Lowe A.A. Correlations between orofacial muscle activity and craniofacial morphology in a sample of control and anterior open bite subjects. American Journal of Orthodontics 1980; 78: 89-92.