
Treatment of inflammatory internal root resorption in the right upper canine with bioceramic cement: A case report.
Abstract
Inflammatory internal root resorption is a resorptive pathological process that progressively destroys intra-radicular dentin and dentinal tubules. With a multifactorial etiology, it is diagnosed through radiographic examinations, and it is crucial to initiate endodontic treatment as soon as possible to halt damage to dental structures and prevent their weakening. Recent technological advances have led to the development of numerous dental materials, such as bioceramic cements, which are indicated for the treatment of this pathology. The objective of this study is to demonstrate the treatment of internal root resorption in tooth 13 using a bioceramic cement through a clinical case report. The use of repair cements, such as bioceramics, combined with early diagnosis and appropriate treatment, has shown to be effective in cases of internal resorption, reducing the risk of dental structure weakening and enabling the retention of the tooth in the oral cavity.
Introduction
Inflammatory internal root resorption is an inflammatory pulpal condition that originates inside the pulp chamber or root canal, progressing in an internal-external (centrifugal) direction. It occurs due to damage to the predentin, where clastic cells initiate resorption in a way that the resorbed space is filled with granulation tissue or a combination of mineralized tissue resembling bone or cementum. It is a rare, asymptomatic pathology with progressive destruction of intra-radicular dentin and dentinal tubules, requiring special attention from dental professionals for correct diagnosis and treatment.
As the disease advances, perforation of the root canal wall may occur, communicating the pulp with the periodontium, which weakens the dental structure. Radiographically, it is characterized by a visible and uniform radiolucent enlargement with symmetrical ballooning appearance and regular contours.
With a multifactorial etiology, including trauma, caries, deep restorations, chronic pulpitis, excessive heat during crown preparation in vital teeth, pulpotomies, etc., these factors stimulate the pulpal tissue, initiating an inflammatory process that leads to the conversion of undifferentiated pulp cells into osteoclasts and initiation of dentin resorption.
Usually asymptomatic, conventional radiographs are essential for diagnosis, as they show a uniform enlargement of the pulp canal with distortion of the original root canal outline. Although aiding in early diagnosis, these radiographs are limited in offering two-dimensional images. Therefore, the use of CBCT (cone-beam computed tomography) becomes necessary as it provides greater detail and precision of the pathology.
Treatment should be initiated as soon as possible to prevent progression, subsequent perforation, and tooth loss. However, irregularities in the root canal space make biomechanical preparation and obturation challenging. Removal of pulp and granulation tissue, along with filling the resorbed lacuna, is essential in managing cases of internal root resorption.
Complete and hermetic obturation is one of the main challenges during the treatment of this pathology. Due to difficulties in filling internal defects, the use of new materials such as bioceramic cements is becoming increasingly common. Bio-c Repair (bio-ceramic repair) demonstrates good marginal adaptation, biocompatibility, and excellent sealing ability in moist environments, in addition to the advantage of easy insertion into the resorptive cavity.
Thus, the present study aims to report the treatment of internal root resorption in tooth 13 using the bioceramic cement (Bio-c Repair).
Case description
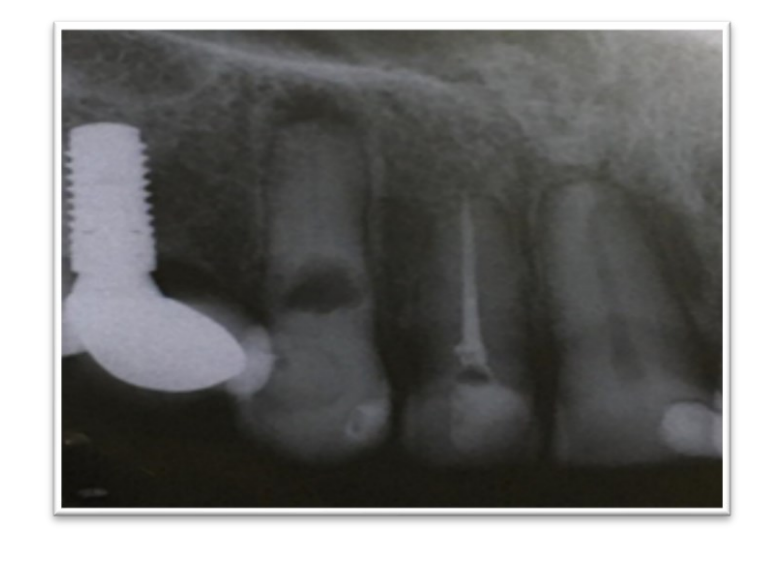
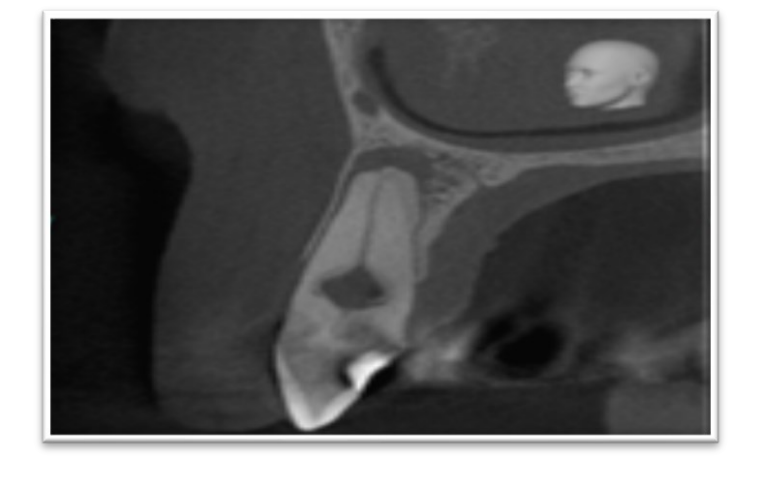
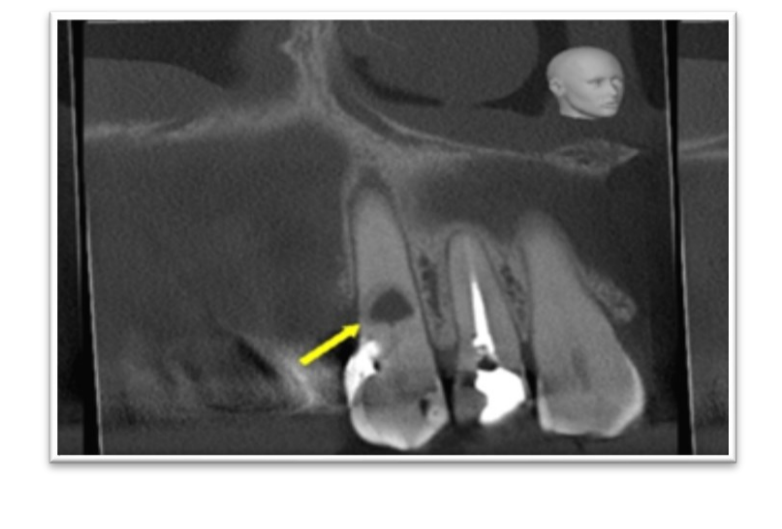
Patient M.W.S.O., a 55-year-old female with hypothyroidism, sought the Postgraduate Dental Center in the interior of Ceará, reporting discoloration in tooth 13 as the main complaint. During the intraoral clinical examination, there was a negative response to vertical percussion, palpation, and thermal sensitivity to cold. The periapical radiographic examination revealed an oval radiolucent image altering the contour of the root canal of tooth 13, suggesting the presence of internal root resorption (Figure 1). In this context, a cone-beam computed tomography (CBCT) was requested as a complementary examination to establish the diagnosis. The CBCT examination revealed a radiolucency in the cervical third of tooth 13, without communication with the external environment, suggesting the presence of inflammatory internal root resorption in the cervical third with irregular contours (Figure 2 and 3).
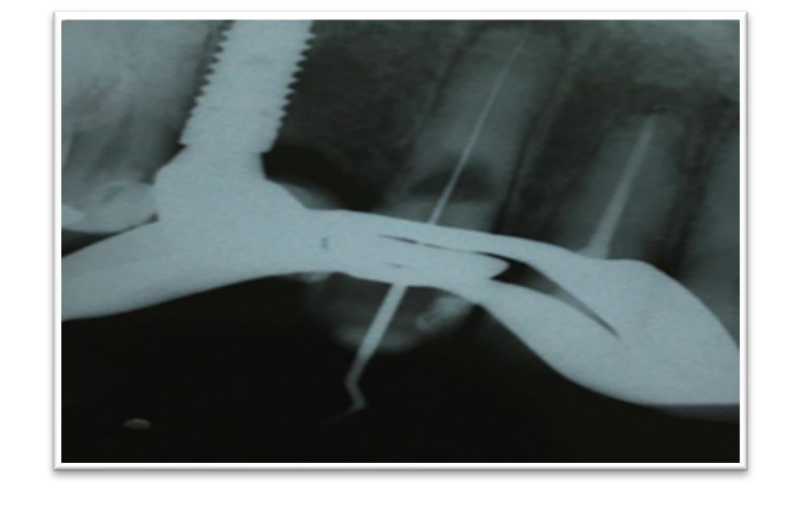
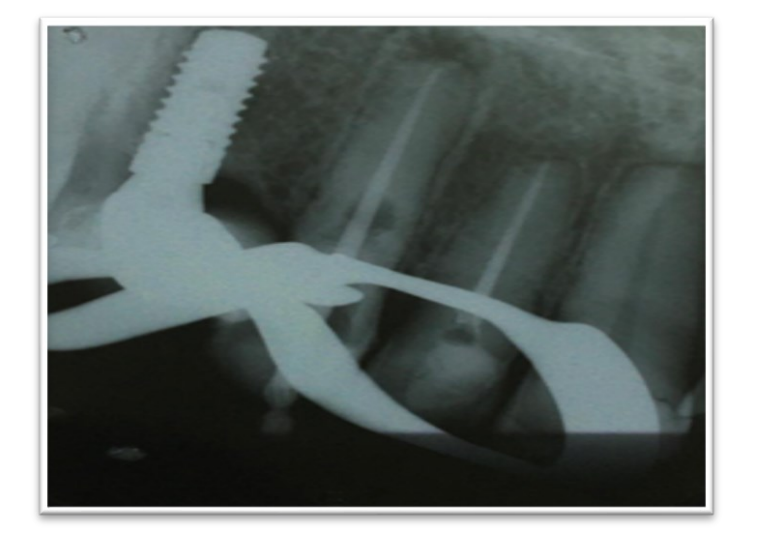
In the first appointment, the septic content was neutralized using 2.5% sodium hypochlorite, and the apparent canal length was measured (CAD) and catheterized at CAD-3 with Kerr #10 file (Dentsply-Mailefer). The preparation of the cervical third was performed with the Primary file from the WaveOne Gold system. Then, odontometry was performed with an electronic apex locator (confirmed with X-ray - Figure 4), reaching the true working length - TWL 24 mm.
Subsequently, manual files #10 and #15 (Dentsply-Mailefer) were used at TWL, followed by the small and Primary files from the WaveOne Gold system at the true working length, always with abundant irrigation of 2.5% sodium hypochlorite between file changes, using the E1 insert (Helse) for agitation of the irrigant solution. After the biomechanical preparation, the final irrigation protocol was performed using the same ultrasonic E1 insert to agitate sodium hypochlorite and EDTA, with cycles of 3x20 s for both irrigants.
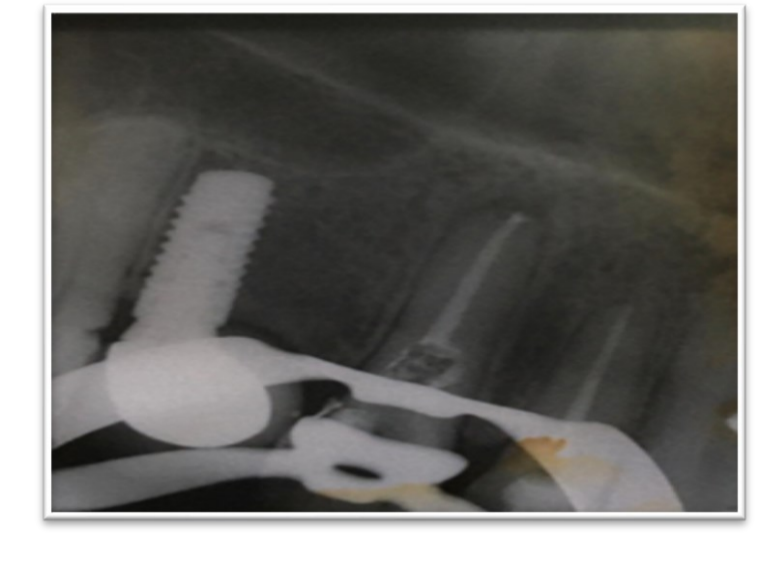
The root canal was dried with sterile absorbent paper points, and the root canal was filled with Calen paste with PMCC for 15 days (Figure 5).
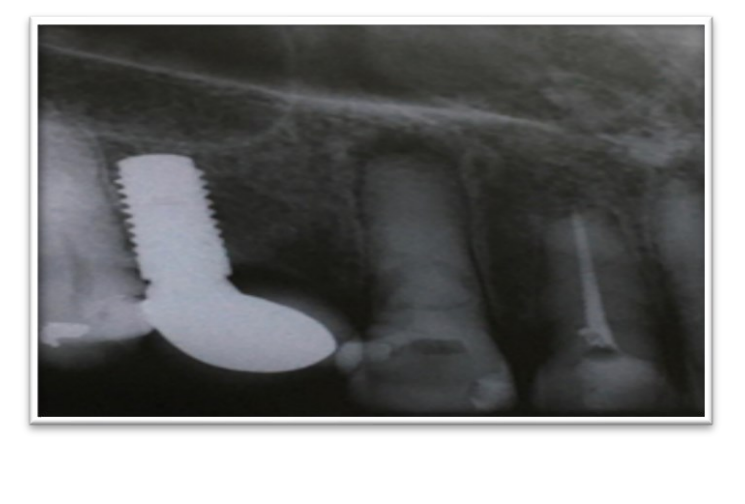
In the second session, after removing the intracanal medication, the root canal was slightly enlarged with the Medium and Large files from the WaveOne Gold system at TWL. After completing the irrigation protocol, conometry was performed with the Large cone from the WaveOne Gold system, followed by periapical radiography (Figure 6).
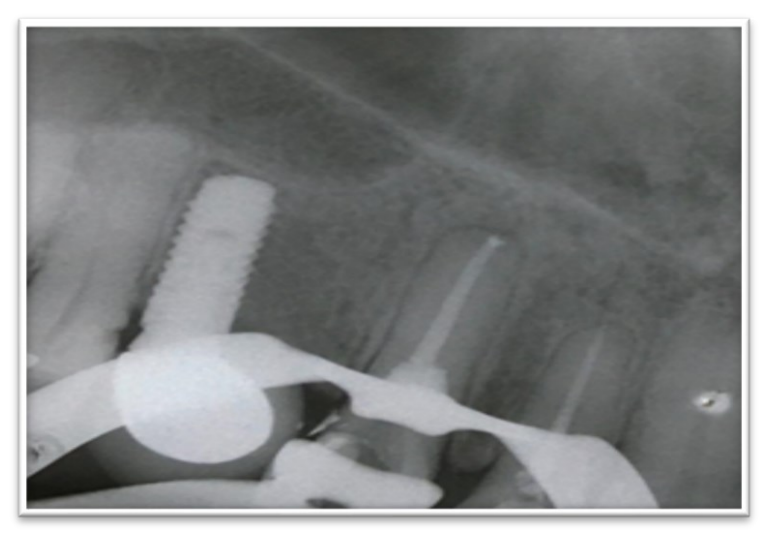
The root canal of tooth 13 was obturated with the Large gutta-percha cone and Ah-Plus sealer (Dentsply) (Figure 7).
The site of internal resorption was entirely filled with Bioceramic (Bio-c Repair - Angelus, Brazil) using a specific condenser and sterile, moistened cotton pellet under electronic microscope guidance (Figure 8). Subsequently, the tooth was restored with glass ionomer cement and composite resin (Figure 9). The patient was instructed to undergo a new cone-beam computed tomography after 6 months for case follow-up.

Discussion
According to Camêlo, internal root resorptions often do not present symptoms. However, during the resorption process, perforation of the dentin wall may occur, making it symptomatic. If the resorption is located in the crown region, it may appear with a pinkish coloration due to the presence of granulation tissue.
For confirmation of the diagnosis, a Cone-Beam Computed Tomography (CBCT) was requested to eliminate possible distortions resulting from conventional radiographs. Similar difficulties were identified by Mehra et al., who also requested this examintion as an aid in the diagnosis.
A 2.5% sodium hypochlorite solution was used for chemical neutralization of the root canal, as it promotes better dissolution of living or necrotic tissues, and it is effective against the microbiota of infected canals. This same solution was used in the works of De Souza et al. and Mehra et al.
The cleaning and shaping were performed using the crown-down technique with reciprocating files from the WaveOne Gold system. Similar preparations for the treatment of internal root resorptions in lower molars were found in the studies of Souza et al.
Calcium hydroxide was the intracanal medication of choice as it allows cauterization of inflamed or granulation tissues. Another factor to consider was the possibility of verifying the extent of the resorption area and observing the complete removal of the pathological tissue through periapical radiographs. This medication was also used in the studies by Dagna and Mehra et al.
The cavity of resorption was filled with Bio-ceramic cement Bio-c Repair (Angelus, Brazil). This material is a ready-to-use repair cement composed of calcium silicate, calcium aluminate, calcium oxide, zirconium oxide, iron oxide, and silicon dioxide as a dispersing agent. Bio-c Repair presents superior characteristics of marginal adaptation, bio-compatibility, excellent radiopacity, and sealing ability in moist environments. Additionally, its great advantage lies in its ease of insertion into resorptive cavities.
Conclusions
Bio-C Repair cement is an excellent option for the treatment of inflammatory internal root resorption due to its characteristics of easy insertion, good marginal adaptation, biocompatibility, and sealing ability in moist environments. However, early diagnosis and appropriate treatment are essential for a favorable prognosis and high rates of clinical success. Bio-C Repair cement is an excellent option for the treatment of inflammatory internal root resorption due to its characteristics of easy insertion, good marginal adaptation, biocompatibility, and sealing ability in moist environments. However, early diagnosis and appropriate treatment are essential for a favorable prognosis and high rates of clinical success.
Roberta de O. Lacerda, Clara I. A. S. e Silva, Alyssa M. Pinheiro2, Irvina C. F. Melo, Ana B. H. R. D. de Sampaio, Eliane M. G. M. de Vasconcelo, Mario F. de P. Leonardi, Cicero L. G. Ramalho
References
- Almeida, D.R.M.F; França, G.M; Lima, J.G.C; Gonçalves, G.C; Silva, G.G; Silva, L.F.B; Pinheiro, J.C. Aspectos clínicos, radiográficos e terapêuticos de reabsorções radiculares internas na endodontia. Revista de Odontologia da Braz Cubas, v. 10, n. 1, p. 82-93, Jan-Jun 2020.
- Consolaro A. Reabsorções dentárias nas especialidades clínicas. 3. ed. ampliada e revisada. Dental Press, 2012. 816 p.
- Umashetty, G.; Hoshing, U.; Patil, S.; Ajgaonkar, N. Manejo da reabsorção radicular interna inflamatória com Biodentina e gutta-percha termoplastificada. Hindawi publishing Corporation, Case Reports in Dentistry. v. 01, 2016.
- Abdullah, D.; Hussein, F.E.; Ghani, H.A. Management of Perforating Idiopathic Internal Root Resorption. Iran Endod J, Tehran, v. 12, n. 2, p. 257 – 260, 2017.
- Braitt, Antônio Henrique et al. Selamento de perfuração com técnica de inserção modificada do MTA: relato de caso clínico. Rev. Odontol. Araçatuba (Online), p. 18-23, 2022.
- Camêlo, F.A.L., Silva, M.S., Argolo, N.M. da R., Monezi, L.L. de L., Neto, D.F.L. e Oliveira, A.P. de 2019. Retratamento endodôntico em dente anterior acometido por reabsorção radicular interna: relato de caso. Revista Eletrônica Acervo Saúde. 21 Apr. 2019.
- Mehra, N. et al. Clinical Management of Root Resorption: A Report of Three Cases. Cureus, California, v. 10, n. 1, p. e3215, Aug. 2018.
- De Souza, et al. Technological advances in endodontics: treatment of a mandibular molar with internal root resorption using a reciprocating single-file system. Gen Dent, Europe, v. 65, n. 3, p. 5 – 8, Jun. 2017.
- Dagna, A. Maxillary Incisor with Internal Resorption: Endodontic and Restorative Management. Restor Dent Endod, South Korea, v. 39, n. 2, p. 137 – 142, May 2016.