Orthodontics and Orthognathic Surgery in the Upper Jaw
Machine translation
Original article is written in ES language (link to read it) .
The 19-year-old patient attended a maxillofacial surgery consultation for evaluation and treatment of dentofacial deformity with malocclusion.
During her first consultation, the patient was questioned about her knowledge of her problem, her expectations, and treatment possibilities. Considering these, a combined treatment of orthodontics and orthognathic surgery was evaluated as the most satisfactory and highest quality treatment.
The patient was then referred to the orthodontics consultation to begin the pre-surgery treatment phase.
Diagnosis
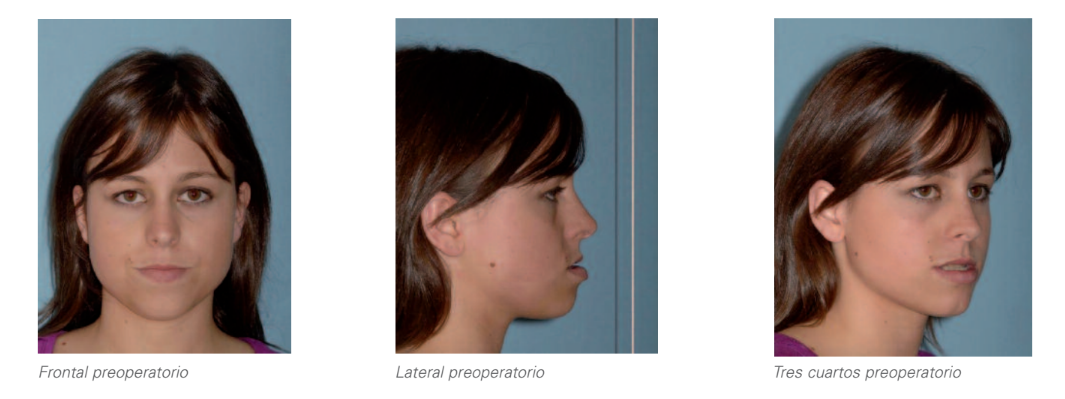
1. Extraoral analysis:
- Wide face.
- Lower third slightly larger than the middle third.
- Adequate exposure of incisors at rest and smile.
- Deviation of the upper midline to the right.
- Negative vector.
- Straight profile.
- Maxillary hypoplasia.
- Lower protrusion.
- Appropriate mandibular contour.
2. Radiographic analysis:
2.1. Panoramic radiography:
- Permanent dentition.
- Adequate bilateral condylar volume without noticeable morphological alterations.
- Included upper right canine and complete lack of space for its eruption.
- Presence of developing wisdom teeth.
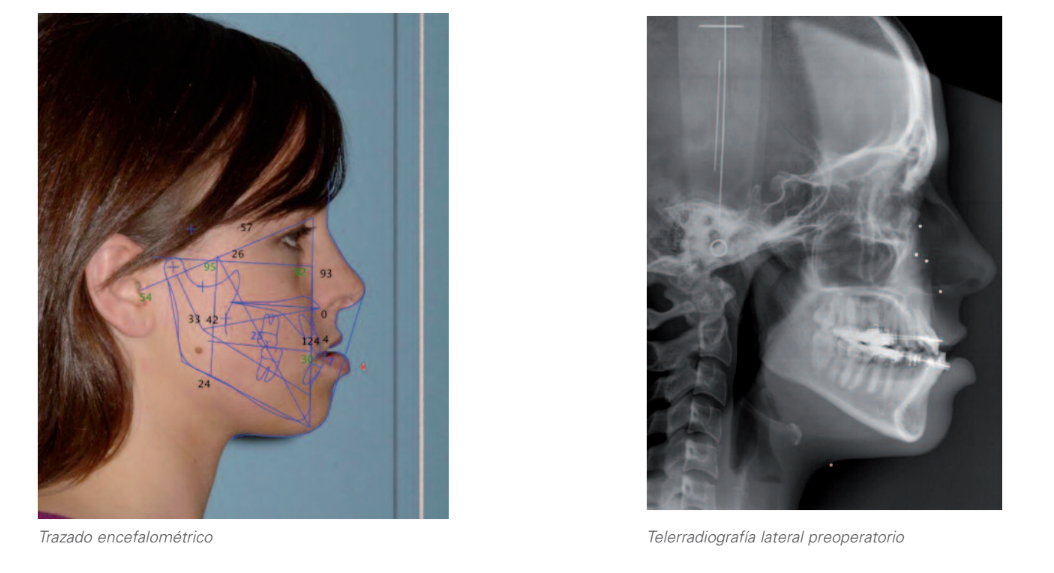
2.2. Lateral cephalometric radiography and cephalometric tracing:
- Brachi facial.
- Slight class III skeletal.
- Incisors...
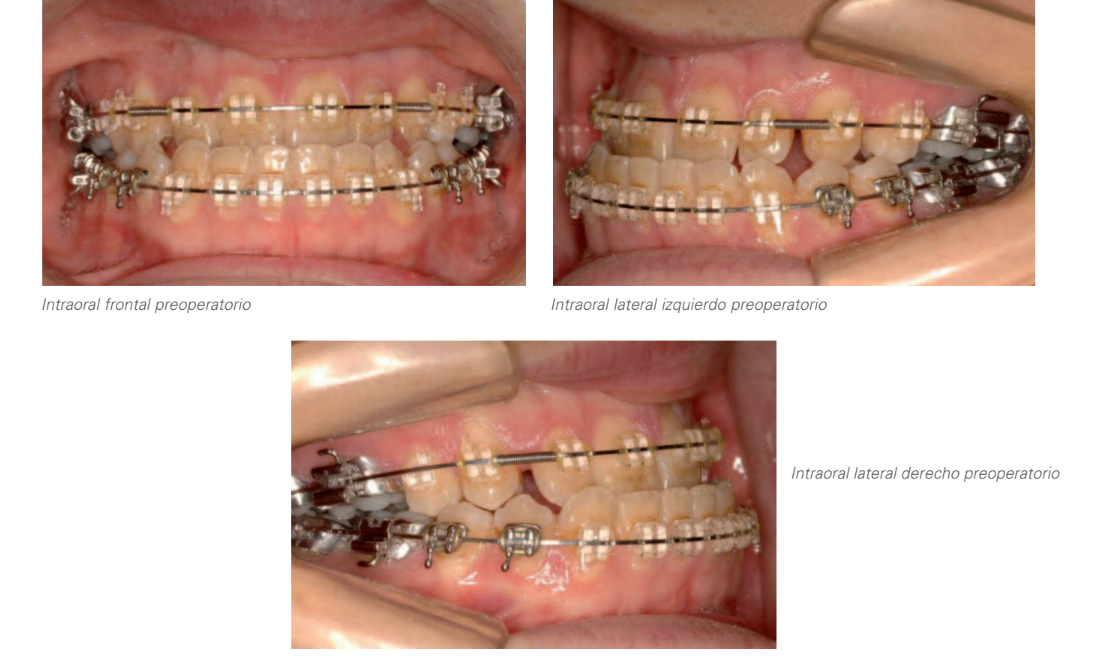
3. Intraoral analysis:
- Deviation of the upper midline to the right by 3.5 mm due to upper dental cause (asymmetric upper arch as a result of the complete lack of space for the eruption of the upper right canine).
- Crossbite of the four upper incisors.
- Overjet: -1 mm.
- Right side: class I molar and canine class not assessable.
- Left side: class I molar and canine.
- Overbite: 0 mm.
Iconography Study: Initial Study




Treatment Plan
In any case, when proposing a treatment plan after a thorough diagnosis, it is necessary to establish treatment objectives for the different areas that will be affected, which serve as a framework for communication with the patient and among different professionals, as well as a critical element for evaluating the results obtained. These objectives are:
- Facial aesthetics.
- Dental aesthetics.
- Functional occlusion.
- Periodontal health.
- Stability.
- Patient satisfaction.
Based on this and aiming to achieve the highest possible degree of compliance in each of the mentioned areas, two treatment options were presented to the patient:
A) Option A:
- Extraction of the upper right first premolar and subsequent traction of the included canine to bring it to its position in the arch, followed by extraction of the upper left first premolar to achieve symmetry in the upper arch, centering the upper dental midline with the facial and lower dental midline and correcting the skeletal class III.
- Subsequently, orthognathic surgery for maxillary advancement would be performed to harmonize the patient's facial aesthetics and achieve an adequate degree of overjet and overbite, as well as a class I canine and complete bilateral class II molar.
- Ultimately, the settling and finishing phase would follow to meet all treatment objectives at the occlusal level.
B) Option B:
- Extraction of the included upper canine and the left upper first premolar in order to achieve symmetry in the upper arch, centering the upper dental midline with the facial and lower dental midline and decompensating the skeletal class III. In this case, the right upper first premolar would remain as a canine for the benefit of a more predictable approach as well as a significantly shorter treatment time.
- Subsequently, orthognathic surgery for maxillary advancement would be performed to harmonize the patient's facial aesthetics and achieve an adequate degree of overjet and overbite, as well as a class I canine and complete bilateral class II molar.
- Ultimately, the phase of settling and finishing would be carried out until all treatment objectives at the occlusal level are met.
- The patient preferred to opt for option B, primarily motivated by the shortening of the total treatment time.
Evolution
- Prior to orthodontic treatment, surgical extraction of the included upper right canine and included lower third molars was performed.
- The postoperative period was uneventful, starting orthodontic treatment at four weeks, with the objectives being:
- Center midlines.
- Increase and shape congruent arches of the maxillae.
- Treat compensations and adjust the negative overjet to the surgical planning.
- Close spaces.
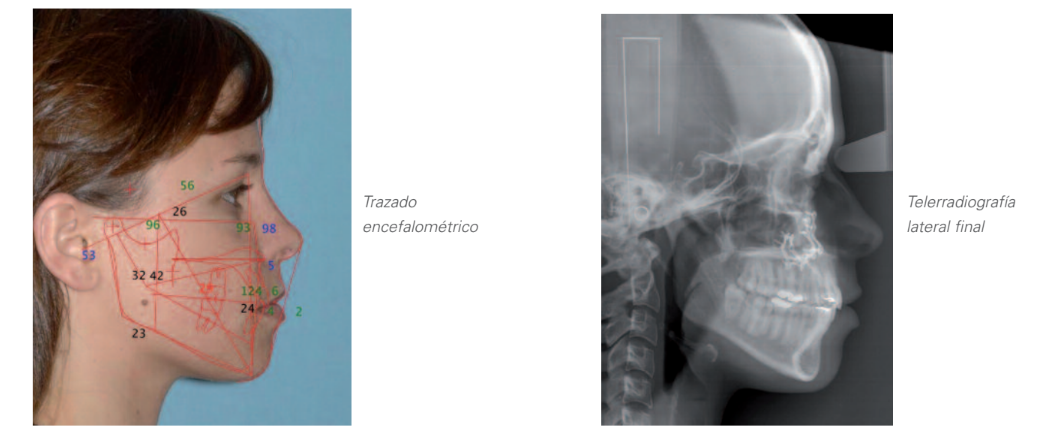
Preoperative state: Final preoperative study after orthodontics

Surgery
The surgery was performed under general anesthesia. A Lefort I osteotomy for advancement and descent was carried out. Of particular importance in this patient was to not alter the lip dynamics and the nasal pedestal, for which the muscular complex around the septum and anterior nasal spine was reconstructed.
The osteotomy was performed without pterygoid dysfunction, advancing and descending the maxilla to the splint without effort.
The osteotomies were rigidly fixed with L plates and once the centric was verified, two class III elastics were placed, with the patient being extubated in the operating room.
The patient was discharged 24 hours later with moderate edema and inflammation and was referred to orthodontics 10 days later for completion of treatment.
Results


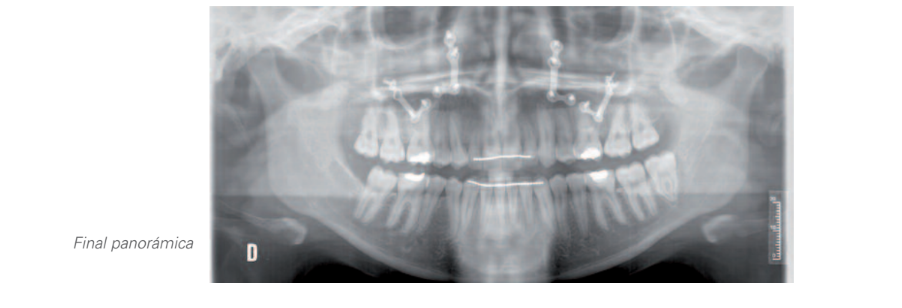
Conclusions
This is probably an easy case of the multiple possibilities offered by the combination of surgery and orthodontics.
The key to the result in this patient lies in the creation of an inverted overbite after the extraction of the included right canine and left first bicuspid, also allowing the maxillary midline to be centered with the face and jaw. The Lefort I osteotomy for advancement and descent is an easy, predictable, and stable surgery with minimal morbidity and rapid recovery. Associated with the occlusal and cosmetic change, the patient requires significant improvement in nasal respiratory dynamics and chewing.
Preoperative - final state comparison


César Colmenero Ruiz, Fe Serrano, Teresa Martínez Iturriaga
Bibliography
- Henry J, Kawamoto, Jr. Simplification of the Le Fort I Osteotomy In Clinics of Plastic Surgery. October 1989, pp. 777-785.
- Harvey M Rosen. Maxillary Hypoplasia: Surgical Treatment with the Lefor I Osteotomy Journal Oral Maxillofacial Surgery 1998. Vol. 62, pp. 114-119.