
Digital impressions on implants: what do we need to know?
Machine translation
Original article is written in ES language (link to read it) .
Workflows in all specialties of Dentistry have undergone a substantial change due to the introduction of CAD-CAM technology. Specifically, new techniques and methods of planning, printing, and manufacturing have generated the need to define new planning and execution protocols in prosthodontics and implantology.
Conventional impression techniques for recording the position of an osseointegrated implant use transfer copings connected to the implant body, impression trays, and elastomeric materials such as polyvinylsiloxane or polyether. However, with the advent of computer-aided design and computer-aided manufacturing (CAD-CAM), it is possible to use a completely digital workflow based solely on the use of an intraoral scanner and a digital impression coping, commonly referred to in English terminology as a scanbody.

Recent scientific literature shows that through the use of scan bodies, intraoral digital impressions have an accuracy that is not inferior and in certain scenarios such as in cases of single-unit rehabilitations even better, compared to conventional (analog) impression techniques.
Apart from the evidenced improvement in patient comfort, the application of CAD-CAM technology in implant prosthetics has helped to simplify or make more efficient a series of treatment steps.
The use of intraoral scanners eliminates the selection and use of the tray, material waste, setting time of the impression materials, disinfection, and sending impressions to the laboratory. Additionally, there are some advantages over conventional impressions, including less distortion and error during the laboratory phases and greater overall efficiency. By definition, accuracy is a combination of precision and truthfulness. Precision describes how close repeated measurements of the same object are to each other, while truthfulness describes how far the measurement deviates from the actual dimensions of the measured object. Both are important considerations in the workflow of digital implant dentistry and should be optimized not only by the scanners but also by the scanbodies themselves.
Today, intraoral scanners have reached an unprecedented level of accuracy with a truth error of 20 to 48 μm and a precision of between 4 and 16 μm when the impression is partial.
The factors that can affect the accuracy of digital impressions in implant prosthetics are:
- Model of intraoral scanner.
- Software version of the intraoral scanner.
- Scanning strategy and protocol.
- Clinical factors such as saliva, blood, free soft tissue, and moisture.
- Operator experience.
- Scanbody (size, shape, material, associated libraries), as it is the component responsible for transferring the information of the intraosseous implant from the scan to the CAD software to design the prosthesis.
As the trend in dentistry to use more digital technology increases, the market offers many intraoral scanners with comparable scanning quality. Furthermore, updating the software of intraoral scanners allows for improved accuracy of the final result while maintaining the same scanner. Fortunately, for some time now, the main changes occur not in the mechanical components of the scanners (“hardware”), but in the programs and algorithms they use (“software”), which allows for updating the scanners, giving them a long lifespan that greatly facilitates their amortization.
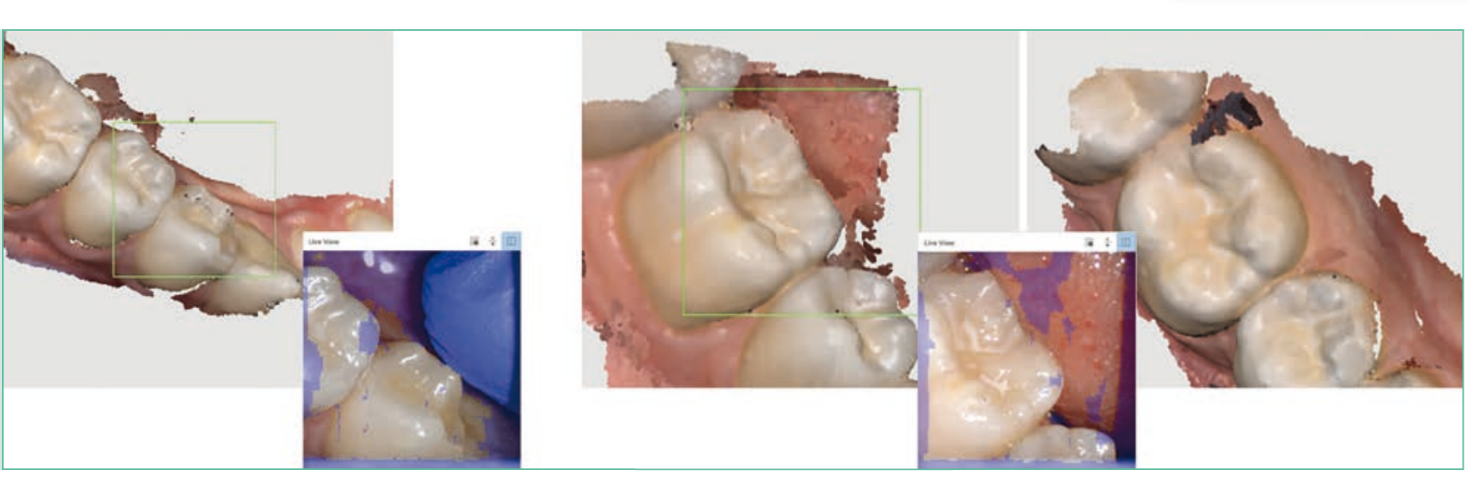
Obtaining an intraoral scan of maximum accuracy is an operator-dependent outcome. It is necessary to understand the strategy of each intraoral scanner we use to reduce the factors that negatively influence precision and accuracy, for example, moving soft tissues (tongue and cheek) using mirrors and intraoral separators, reducing intraoral moisture with continuous suction to eliminate blood and saliva, and avoiding direct light sources to the area being scanned.
The development of artificial intelligence can assist in the scanning process, informing the clinician of every detail and sometimes eliminating clinical risk factors to obtain a quality intraoral scan, through alerts for excess brightness, automatic removal of movable soft tissue, and reliability maps, among others.

Scanbody
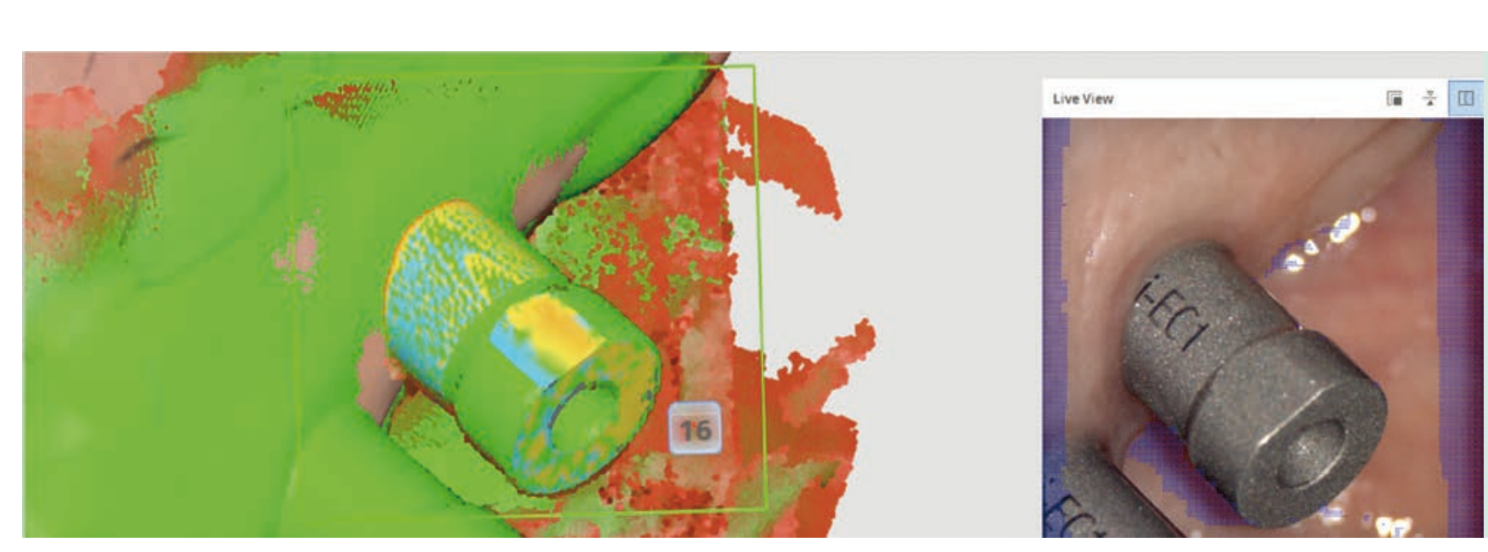
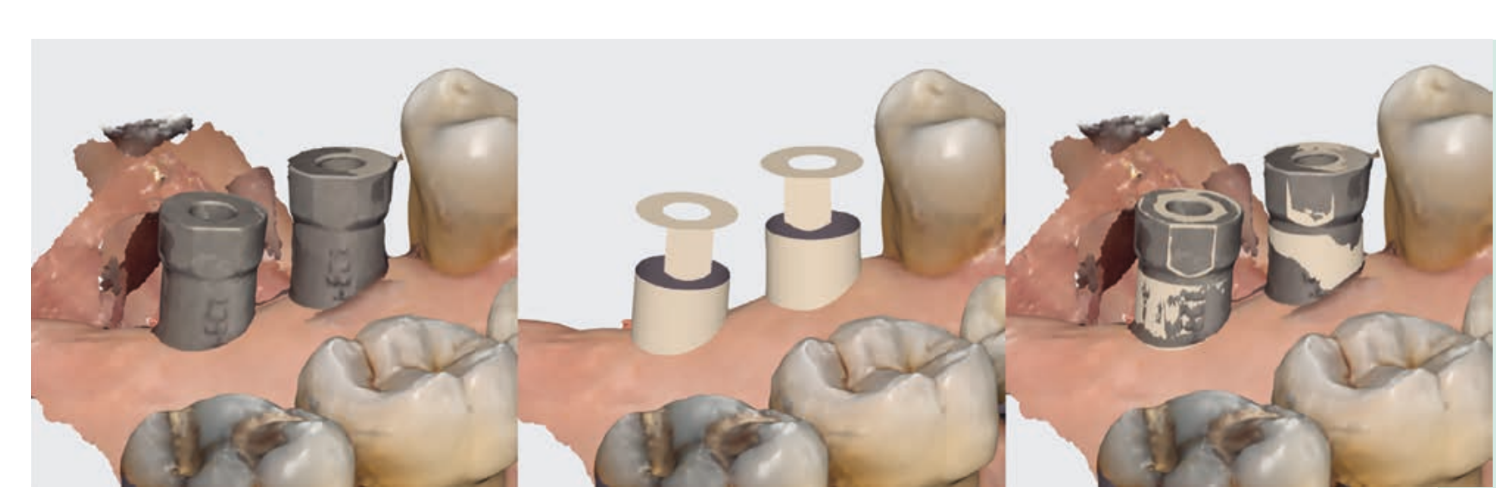
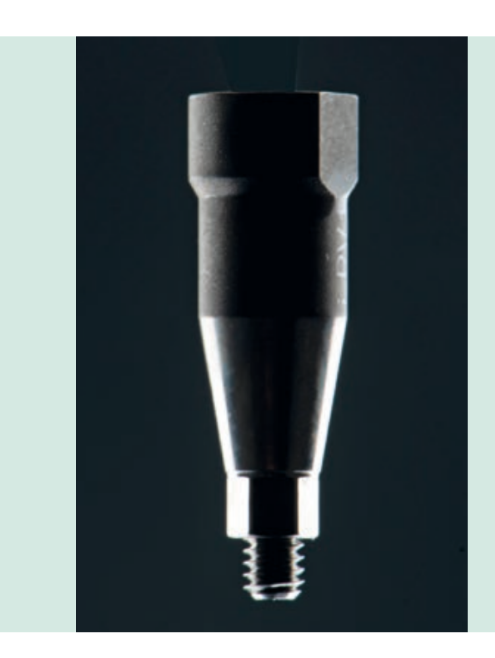
Another factor that also influences the accuracy of the digital impression on implants is the scanbody. Scanbodies are components that are screwed onto the implant and are responsible for transferring the position of the implant in space; they have characteristics that vary greatly from one manufacturer to another, such as: material, shape, size, surface, connection, reusability, software/scanner compatibility, cost, and geometry. It is generally composed of three regions: the base or connection to the implant, the body, and the recognition surface.
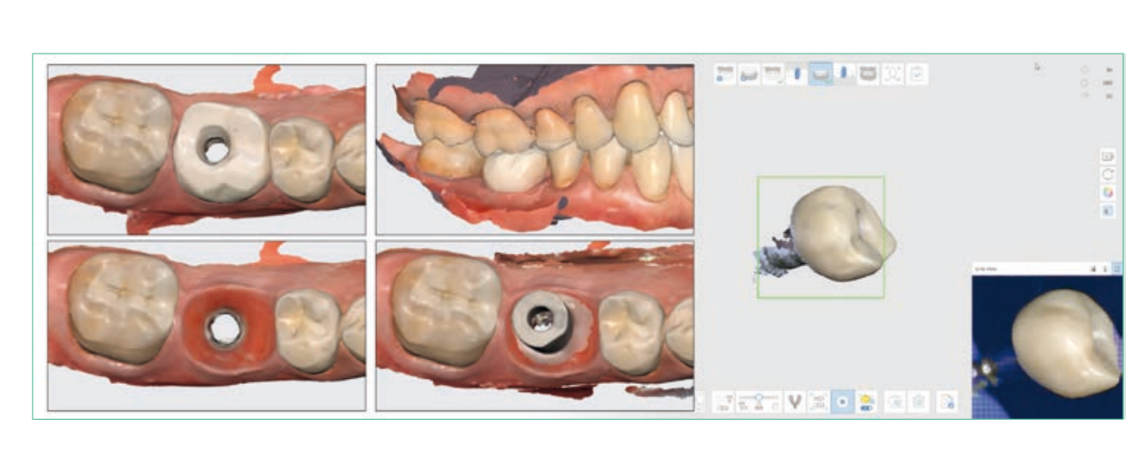
Once the intraoral scanning is completed, a digital file in Standard Tessellation Language (STL) containing the scanbody is generated. This file will be introduced into a specific CAD design software that contains different libraries of scanbodies (Clouds); through specific algorithms, the CAD software will identify the scanbody and align it with its belonging library, thus accurately transferring the position of the implant in space.
Recent studies show that geometries of lower complexity are more reliable in the data acquisition phase when scanning intraorally and in alignment with the libraries when performing the overlay in CAD software. In general, objects with deep, undercut, sharp, angled, or crowded surfaces are more difficult to scan, resulting in a less accurate point cloud. Therefore, the geometry of the scanned body plays a very important role in the accuracy of the digital transfer of the implant position, a fact that has been overlooked in Dentistry in recent years.
Another point to consider when selecting a scanbody is the material it is made of, and we mainly find two types: Polyetheretherketone (PEEK) and titanium. The importance of material selection lies not so much in the body of the scanbody but in the base or connection to the implant. A radiopaque base, such as that offered by titanium, allows us to perform a radiographic verification of the scanbody's seating prior to scanning. Therefore, it is common to find abutments that have a metal base and a PEEK body, as this facilitates scanning by avoiding the reflections typical of metal, although with appropriate surface treatment, it is also possible to achieve abutments with a titanium body that are perfectly scannable.

Unlike titanium scan bodies, PEEK scan bodies will require additional care with sterilization, as they are prone to greater wear and deterioration over time, which can affect their geometric shape and, therefore, the recognition and alignment of the file. In the case of using scan bodies that combine PEEK and titanium, it is necessary to pay attention to a good fit between both materials, as successive uses can compromise the union, causing inaccuracies.
It is important to remember that in the digital environment, not only the factors related to the scanbody matter, but also the availability and characteristics of libraries that will influence the selection of the scanbody. To rehabilitate an implant, there are different brands of scanbody, manufactured by the implant company itself, by milling centers, or by "clone" companies. In this scenario, efficient communication with the laboratory is recommended, which will indicate and facilitate the selection of the scanbody to be used for the subsequent fabrication of the definitive prosthesis based on the prosthetic solutions needed for each case.
The protocol to follow for a correct definitive digital impression is:
- Intraoral scanning (I.S.) of the arch to be treated with the provisional in place (or in the absence of a provisional prosthesis, scan with a healing abutment).
- I.S. of the opposing arch.
- I.S. of occlusal relationship as a bite record.
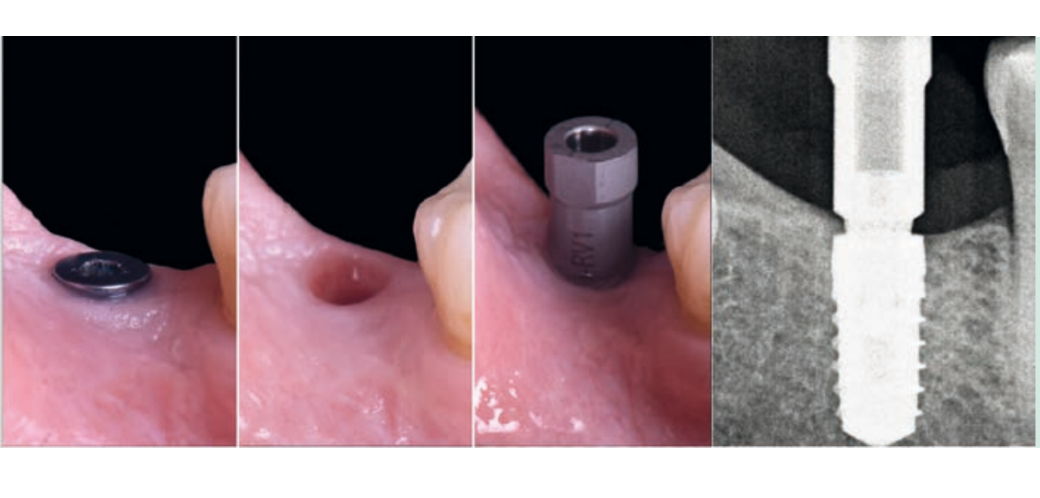
- Unscrew the provisional prosthesis and I.S. of the emergence profile.
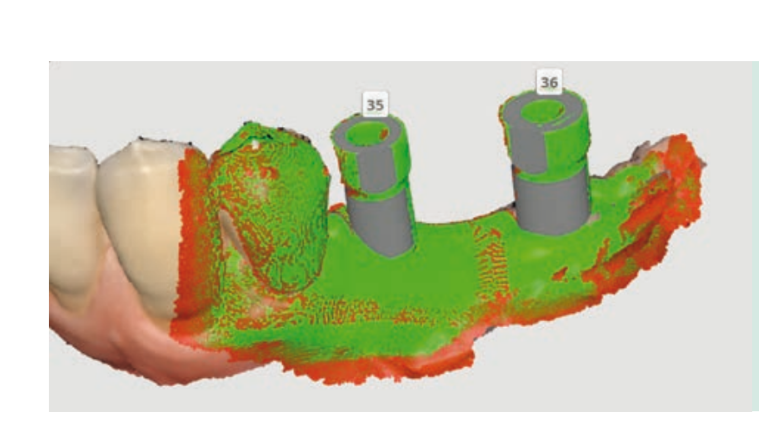
- Screw in the scanbody and position the flat reference face towards the palatal in the upper jaw due to the presence of the lip and towards the buccal in the lower jaw due to the presence of the tongue.
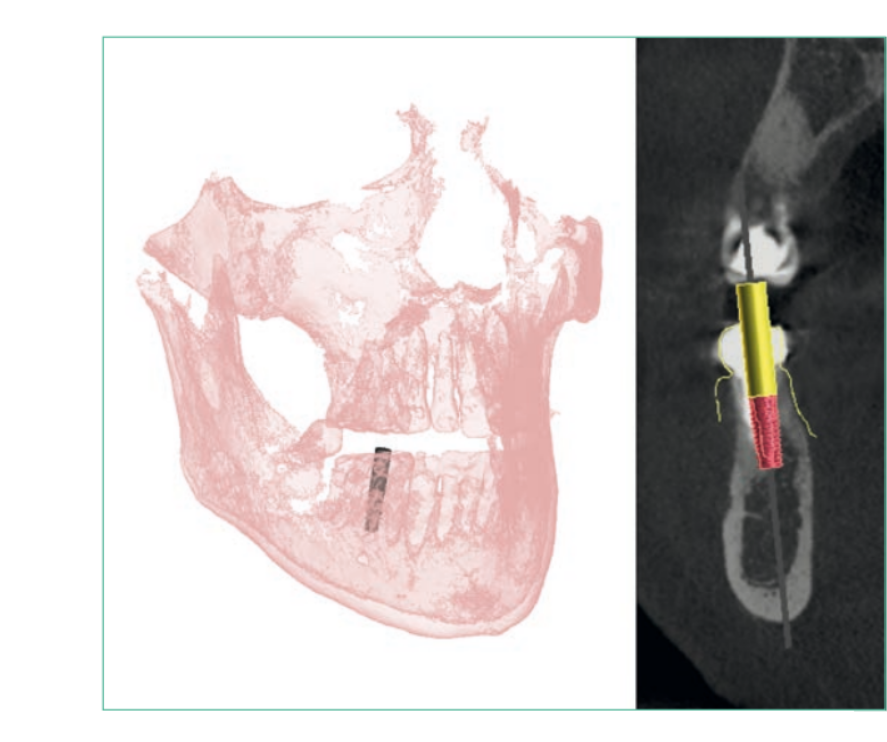
- Radiographically check the seating of the scanbody to the connection.
- I.S. of the problematic arch with the scanbody in the mouth.
- Optionally, an extraoral scan of the provisional prosthesis can be done to have information about the emergence profile.


The methods of manufacturing definitive prostheses with monolithic materials require a digital workflow in the laboratory stages. However, it is not necessary for the clinician to follow a completely digital protocol. An alternative is that, by taking a conventional impression, the laboratory is able to digitize it by placing scanbodies for extraoral scanning, thus allowing for a hybrid digital workflow. Nevertheless, although the desktop scanners used by the laboratory are very accurate (more than intraoral ones), they have the drawback of carrying over the errors from the conventional impression, which is generally less accurate than the digital one.
Ultimately, the advantages of implant-prosthesis treatments through a digital workflow far outweigh those present in the conventional workflow. For this, it is necessary to know and control the factors that influence the accuracy of digital impressions on implants, among which the following are paramount:
- Selection of scanbodies based on their characteristics and libraries.
- Favorable clinical factors.
- Operator experience.

Bibliography
- Mizumoto, Ryan M.; YILMAZ, Burak. Intraoral scan bodies in implant dentistry: A systematic review. The Journal of prosthetic dentistry, 2018, 120.3: 343-352.
- Flügge, Tabea V., et al. Precision of Dental Implant Digitization Using Intraoral Scanners. The International journal of prosthodontics, 2016, 29.3: 277-283.
- Alikhasi, Marzieh; ALSHARBATY, Mohammed Hussein M.; MOHARRAMI, Mohammad. Digital implant impression technique accuracy: a systematic review. Implant dentistry, 2017, 26.6: 929-935.
- Arcuri, Lorenzo, et al. Influence of implant scanbody material, position and operator on the accuracy of digital impression for complete-arch: A randomized in vitro trial. Journal of prosthodontic research, 2020, 64.2: 128-136.
- Chochlidakis, Konstantinos M., et al. Digital versus conventional impressions for fixed prosthodontics: A systematic review and meta-analysis. The Journal of prosthetic dentistry, 2016, 116.2: 184-190. e12.
- Crockett, Russell, et al. Digital custom implant impression technique for capturing the acquired emergence profile. The Journal of prosthetic dentistry, 2019, 122.4: 348-350.
- Lee, Sang J., et al. Accuracy of digital versus conventional implant impressions. Clinical oral implants research, 2015, 26.6: 715-719.
- Rutkünas, Vygandas, et al. Accuracy of digital implant impressions with intraoral scanners. A systematic review. Eur J Oral Implantol, 2017, 10.Suppl 1: 101-120.
- Gintaute, Aiste, et al. Accuracy of computerized and conventional impression-making procedures for multiple straight and tilted dental implants. 2016. PhD Thesis. Department of Prosthodontics, School of Dentistry, University of Freiburg.