Original article is written in ES language (link to read it) .
Clinical relevance
The endless discussions regarding the existence of a Centric Relation (CR) that is punctual or individualized, restricted or long, rehabilitating patients with changes in Vertical Dimension of Occlusion (VDO) in CR or MIH (Maximum Intercuspal Habitual), deprogramming methods, and techniques for recording maxillomandibular relationships with the skull are detailed when the patient is seen as the protagonist of the process and the physiological and mechanical mechanisms involved in the loss of stability and functional balance are understood, as well as the mechanisms to be achieved in the Rehabilitation of the functional system so that it operates with maximum stability and balance, offering longevity to what is executed. Aware of the various ideological paths and respectful of the numerous philosophies advocated, we are absolutely convinced of the steps recommended to propose the 2and2 Concept as a rational method of biomechanical Rehabilitation for patients with changes in VDO, with or without the associated presence of Parafunction. The use of ceramics in sectors 01 and 02 (anterior-inferior and anterior-superior, respectively) is based on the better mechanical performance of the material for the biomechanical forces exerted by sliding and/or rolling, maintaining its dimensional and aesthetic stability, consequently promoting the longevity of the disocclusive system responsible for the balance of the Centric Relation as well as the new proposed VDO. Additionally, the indication of composite resins in sectors 03 and 04 (posterior-inferior and posterior-superior, respectively) is also due to the solid understanding in the Literature for presenting the best mechanical performance under the compressive forces exerted in this sector; thus, the supportive consolidation of the new VDO is present without interference in the disocclusion processes, considering it presents the necessary characteristics for the concept of resilience and self-adjustment capacity during the functional adaptation stage of the system over the following years.
It does not matter the chosen path or the materials selected, as the history of literature presents us with numerous rehabilitative possibilities. The 2and2 Concept is just another path, with a logical and rational systematization of the process, facilitating understanding and execution and, above all, horizontalizing Oral Rehabilitation, making it possible for everyone.
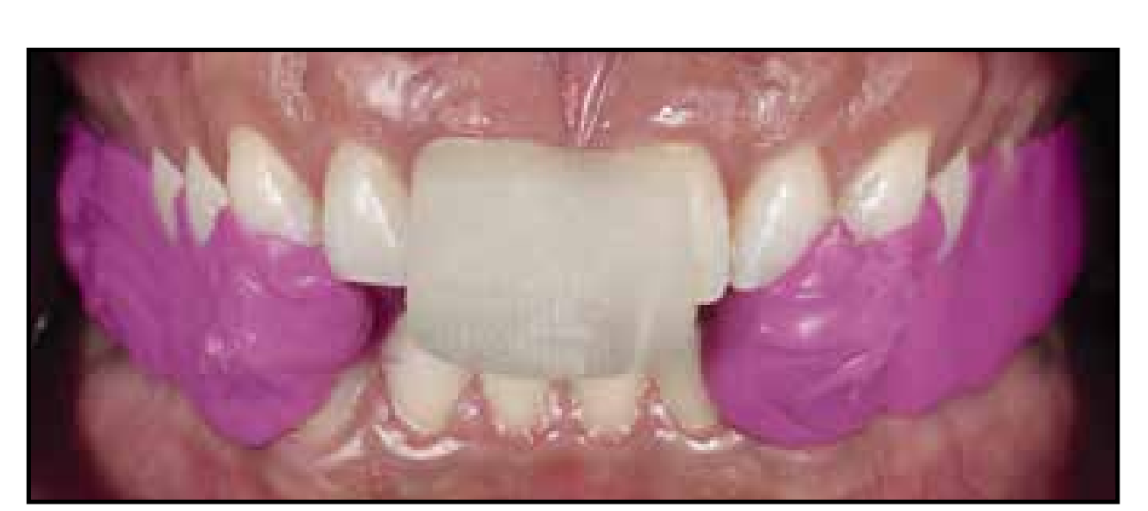
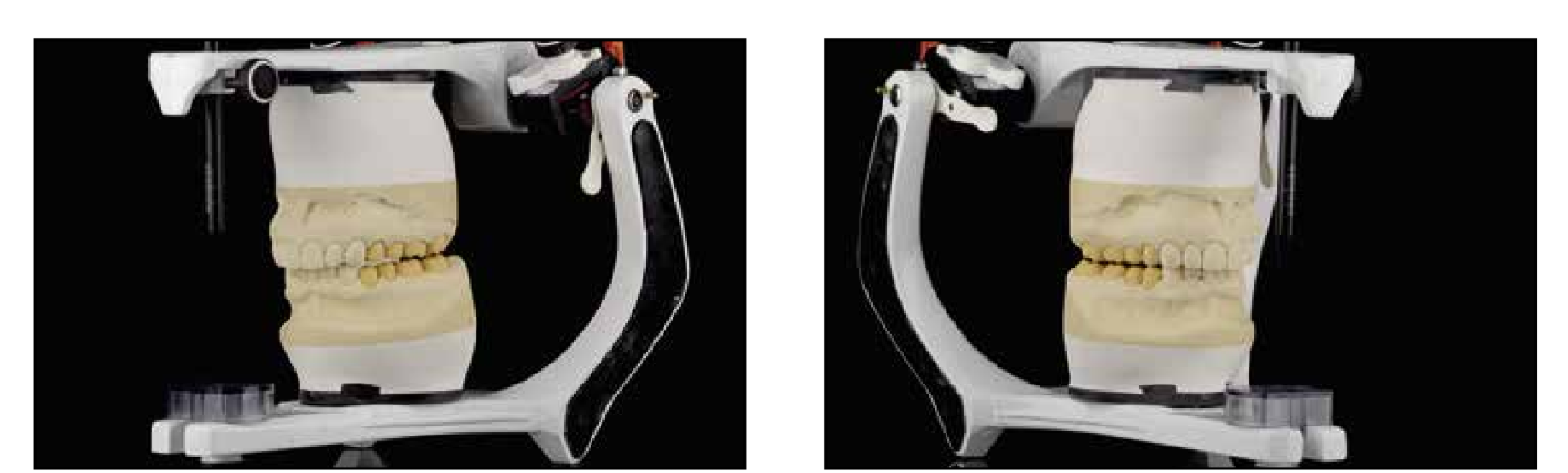
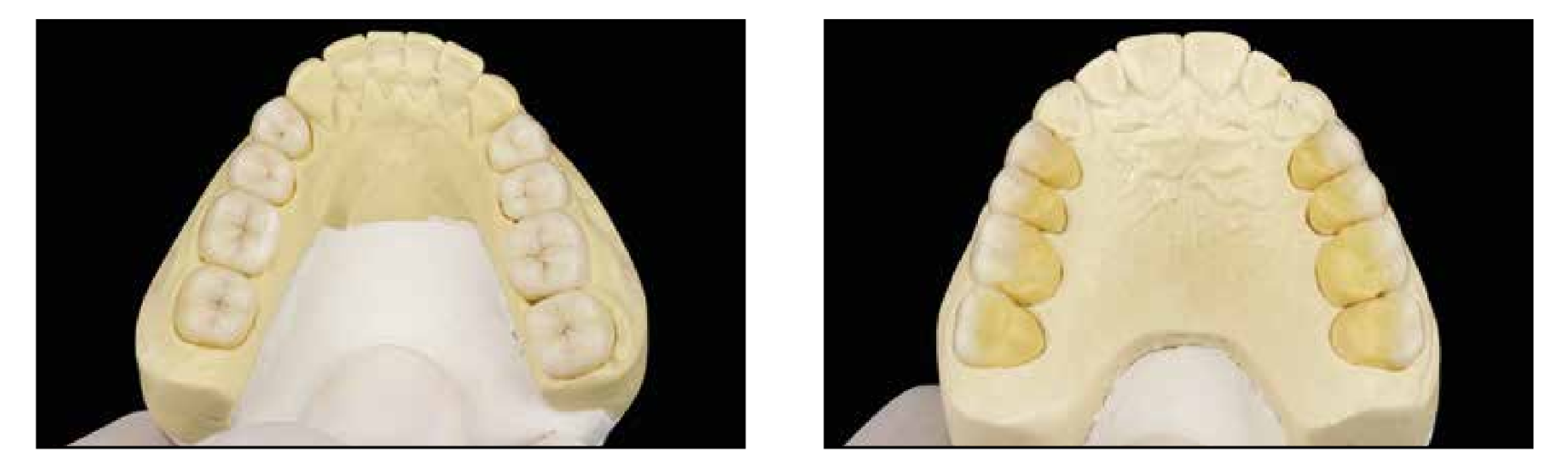
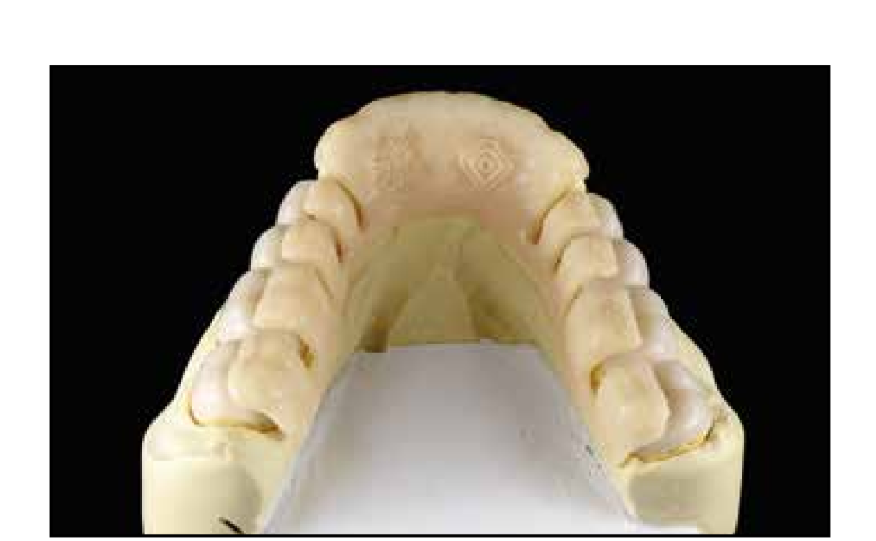
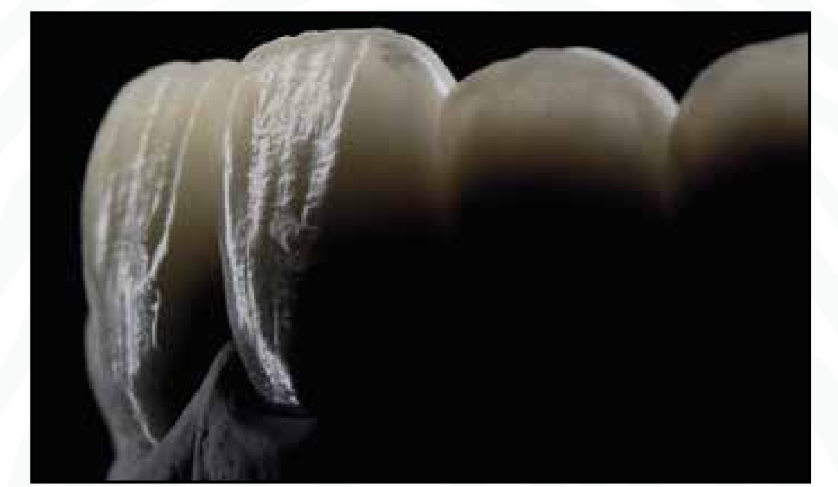
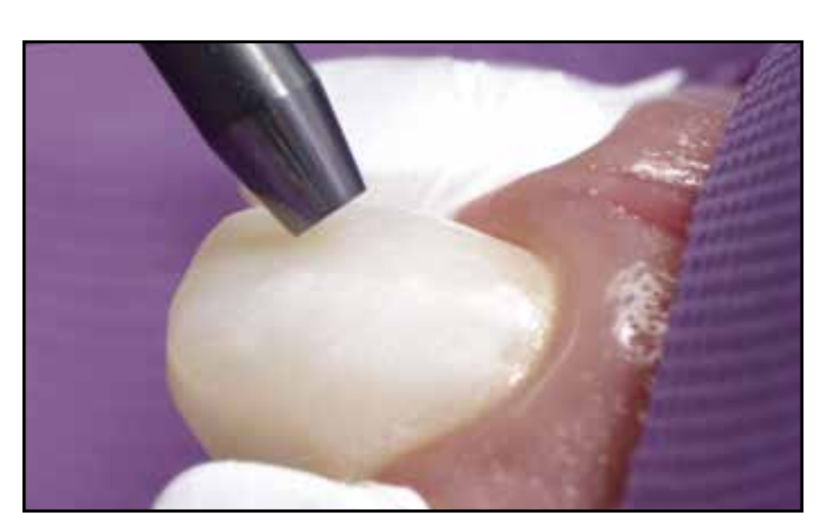
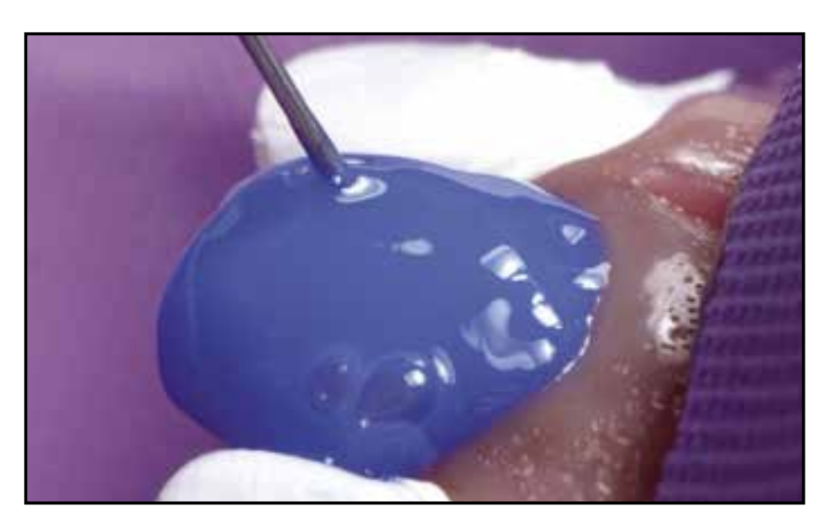
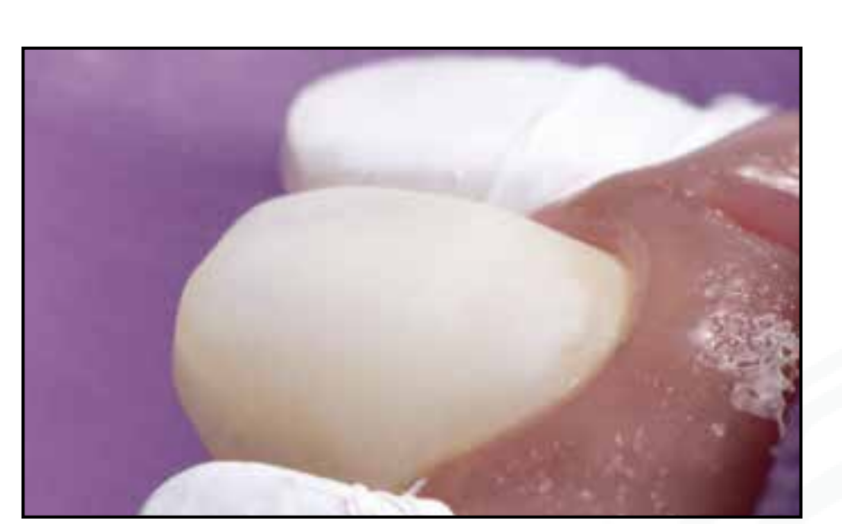
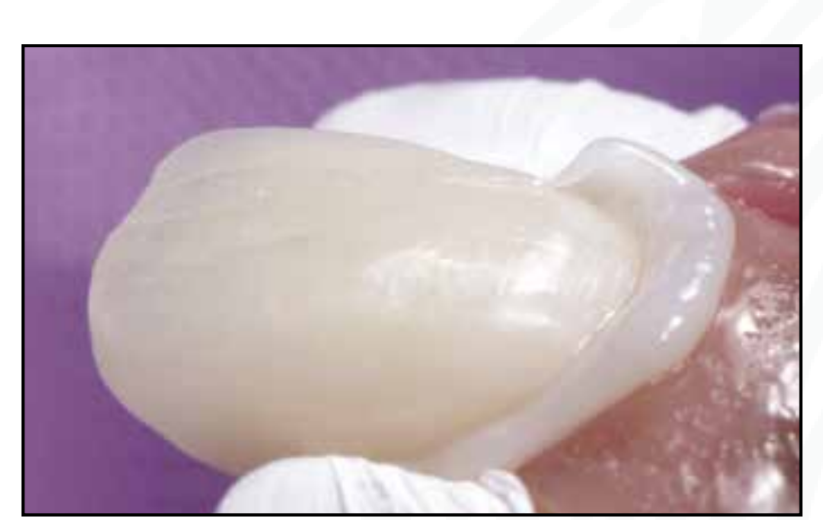
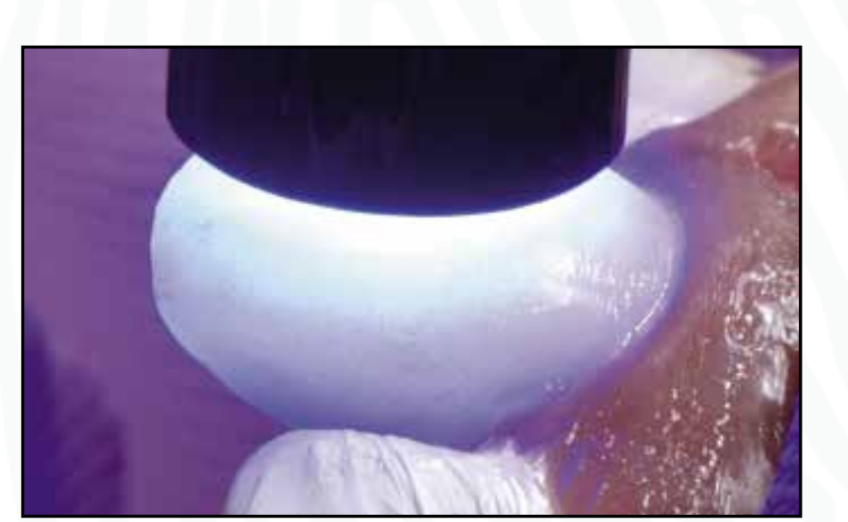
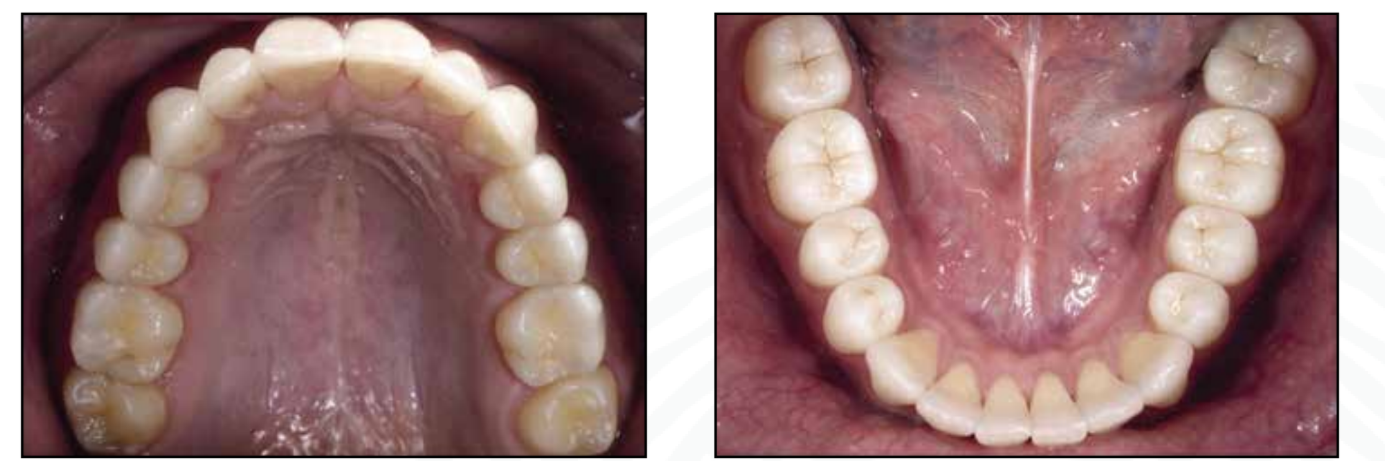
Figure 1: Aesthetic-Functional Rehabilitative Planning based on the analysis of facial references. In this case, the patient presents a significant discrepancy in the teeth, especially during the dynamics of the smile, also due to a scar present on the upper lip on the right side, which can be better observed in the lip-dental photos.Figure 2: Absence of dental exposure in static analysis of the lip-dental relationship, demonstrating a discrepancy with the ideal aesthetic parameters for the male gender in which the literature presents indications of exposure of 2.0mm of the incisal edge of the upper central incisors.Figure 3: In dynamic analysis of the lip-dental relationship, there is noted hyperactivity of the upper and lower lip on the right side in addition to the flattening of the incisal edges due to wear generated by the diagnosed parafunction.Figure 4: In induced manipulation, the patient shows a clear discrepancy between the positions of Centric Relation and Maximum Habitual Intercuspidation. A situation of considerable severity when summing up signs and symptoms leading to the diagnosis of Parafunction which generates instability and imbalance of the functional process.Figures 5-6: In deocclusion, a functional imbalance is observed with corresponding posterior wear bilaterally characterizing the implosion of the functional system.Figures 7-9: In the foreground, the wear of functional structures in sectors 01 and 02 and loss of plus of the canines is observed, characterizing the loss of anterior guides and consequent loss of functional system protection.Figure 10: Elite® Facial Arch, Bioart registered for the proper transfer to the Semi-Adjustable Articulator of the horizontal and vertical relationships of the maxilla in relation to the skull.Figure 11.Figures 11-13: Lucia jig made and installed for recording the maxillo-mandibular relationship for assembling the Semi-Adjustable Articulator, deprogramming the neuromuscular system, and consequently recording the Centric Relation as the starting point for diagnosis and Aesthetic-Functional Rehabilitation Planning.Figure 13.Figure 14: Aesthetic-Functional Rehabilitative Planning based on the CAS concept and Sectorization, establishes with the waxing exclusively of sectors 01 and 02 (anterior-inferior and anterior-superior) the bilateral and simultaneous contact of canines and coupling of incisors. This is one of the rational and easily applicable clinical steps that is part of the 2and2Concept method.Figure 15.Figure 16.Figures 15-17: Installation of a functional mock-up highlighting bilateral and simultaneous contact on canines, coupling of incisors, uniform posterior prosthetic space, and reestablishment of canine disocclusion guides.Figure 18: Confirming the new Vertical Dimension of Occlusion, canine disocclusion guides, and maintaining the Centric Relation as a starting point for the new Rehabilitation, the maxillomandibular relationship is recorded.Figures 19-20: Molds obtained with Express XT® addition silicone, 3M ESPE.Figures 21-22: Plaster models mounted on A7 Plus® Semi-Adjustable Articulator, Bioart from the molds and records obtained after the functional mock-up checked in the mouth.Figures 23-24: Composite resin restorations made by Prof. Dr. Luis Gustavo Barrotte Albino, applying the NEDS technique - Natural Enamel and Dentin Substitution in accordance with the required functional standards: Spee Curve, Wilson Curve, and Three-Dimensional Alignment.Figures 25-26: In a Semi-Adjustable Articulator, the occlusal patterns of gear engagement and functional disillusion of composite resin restorations are checked, maintaining the 2and2Concept technique as a rational method for rehabilitating patients with loss of OVD associated with Parafunction.Figure 27: The Adhesive Cementation Guide, created collaboratively by the authors, is presented in a novel way as a tool to facilitate the cementation process, maintaining the functional standard of restorations while minimizing positioning errors of the pieces and subsequent adjustments.Figure 28: In frontal view, highlighting the cemented pieces in sectors 03 (posterior-inferior) and 04 (posterior-superior) characterizing the application of the ideally designed three-dimensional alignment without adjustments of the pieces post-cementation due to the use of the Adhesive Cementation Guide.Figure 29: Adjustments to the substrates of sector 02 for correct insertion and adaptation of the ceramic pieces to be made.Figure 30.Figure 31. Occlusal records of maxillomandibular relationships and molds obtained with Express XT® silicone, 3M ESPE.Figure 32: Highlight of the surface texture of the ceramics made by the Ceramist Leonardo Bocabella.Figures 33-44: After completing the trial stage with Try-In pastes from the RelyX Veneer® system, 3M ESPE, the sequence of the adhesive cementation process is carried out, finishing with the appropriate photopolymerization with Elipar Deep Cure®, 3M ESPE and meticulous removal of excess with Eccesso® Spatula, LM Dental to avoid interference with the adaptation of adjacent pieces.Figure 35.Figure 36.Figure 37.Figure 38.Figure 39.Figure 40.Figure 41.Figure 42.Figure 43.Figure 44.Figure 45: Immediate intraoral result after cementation, achieving desired aesthetic standards with integration between substrate and ceramic pieces.Figure 46: With rotational movement without interference, the system presents total engagement of the rehabilitated dental elements in the 2and2Concept method, rehabilitating the patient in Maximum Intercuspidation with Joint Comfort.Figures 47-48.Figure 49. Anterior and Canine disocclusion guides provided, offering balance to the functional system.Figure 50: Image of the static lip-dental relationship highlighting the exposure of the incisal edge with lips at rest in convergence with ideal patterns.Figure 51: Image of the dynamic lip-dental relationship highlighting the aesthetic prominence of the Central Incisors and the formation of an ascending curve towards the posterior of the incisal edges.Figures 52-53: Upper and lower occlusal images, highlighting the aesthetic-functional rehabilitation in the 2and2Concept method where we advocate the use of composite resins in sectors 03 and 04 (lower and upper posterior) and ceramic materials in sectors 01 and 02 (lower and upper anterior) as a way to restore the best performance of the mechanical systems involved in the functional process. Obviously, this is only possible when the basic principles of functional rehabilitation are followed, restoring the Curves of Spee, Wilson, Three-Dimensional Alignment, and Morphology Applied to Function.Figure 54: Highlight of the ceramic pieces made by the ceramist Leonardo Bocabella installed performing the aesthetic function and, above all, the functional sliding of the anterior and canine guides.Figure 55: Comparative images highlighting the naturalness of the result.Figure 56: When the patient is the protagonist in the development of techniques and concepts, it always promotes natural results, aesthetically satisfying, and the promotion of health with the rehabilitation of parafunctional patients, with losses of dental structure and clinical signs of chronic suffering. From this point, the rehabilitation of functional structures must be maintained and preserved with the continuous use of rigid occlusal plates, thus controlling the severity of the consequences of Parafunction.
References
Abduo J. Safety of increasing vertical dimension of occlusion: A systematic review. QDT. 2012.
Albino LGB, Gradinar O, Cardoso PC, Decurcio RA. A new concept in oral rehabilitation: 2and2 CONCEPT. Clínica - International Journal of Brazilian Dentistry, Florianópolis, v. 15, n. 3, p. 200-215, jul./sep. 2019.
Alonso AA. Deocclusion • Three-Dimensional Alignment and Occlusion. Quintessence Editora. Edition: 1st/2020.
Andrews LF. The six keys to normal occlusion. AJO-DO. 1972.
Baladhandayutham B, Lawson NC, Burgess JO. Fracture load of ceramic restorations after fatigue loading. J Prost Dent. 2015.
Calamita M, Coachman C, Sesma N, Kois J. Occlusal vertical dimension: treatment planning decisions and management considerations. Int J Esthet Dent. 2019.
Da Rosa Rodolpho PA, Donassollo TA, Cenci MS, Loguércio AD, Moraes RR, Bronkhorst EM, Opdam NJ, Demarco FF. 22-Year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent Mater. 2011.
Y Katoh, Y Taira, C Kato, M Suzuki, K Shinkai. A case report of a 20 year clinical follow-up of porcelain laminate veneer restorations. Operative Dentistry. 2009.
Magne P, Schlichting LH, Maia HP, Baratieri LN. In vitro fatigue resistance of CAD/CAM composite resin and ceramic posterior occlusal veneers. J Prost Dent. 2010.
Opdam NJ et al. Longevity of posterior composite restorations: a systematic review and meta-analysis. J Dent Res. 2014.
Schlichting LH, Maia HP, Baratieri LN, Magne P. Novel-Design ultra-thin CAD/CAM composite resin and ceramic occlusal veneers for the treatment of severe dental erosion. J Prost Dent. 2011.
Wiens JP, Goldstein GR, Andrawis M, Choi M, Priebe JW. Defining centric relation. J Prost. Dent. Jul 2018.