The importance of treatment planning and patient compliance in the clear aligner orthodontic technique
Introduction
Clear aligners have been demonstrated to be a predictable and efficient appliance for orthodontic therapy. Even though there are many commercial brands, Invisalign (Align Technology) has become the most popular among orthodontists worldwide, millions of clinical cases having been treated. With the advance of technology, 3D treatment set-ups are now much more predictable than before, and the fabrication of in-office aligners is more affordable because 3D printers, resins and thermoplastic sheets are available almost everywhere.
Every orthodontic clinical case, regardless of the technique and appliance, requires a comprehensive diagnosis in order to create a treatment plan tailored exclusively for the patient. The aim of the article is to show two different treatment options using clear aligners for malocclusions, both of moderate complexity, one treated with Invisalign and one with in-office aligners.
Patient 1–treated with the Invisalign Lite Package
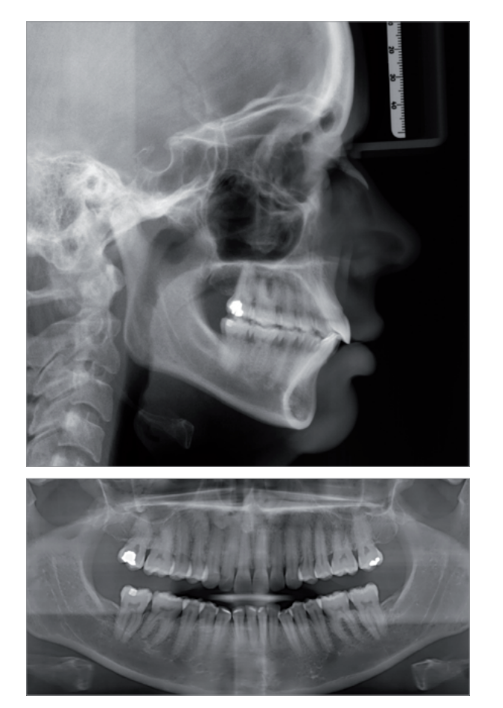
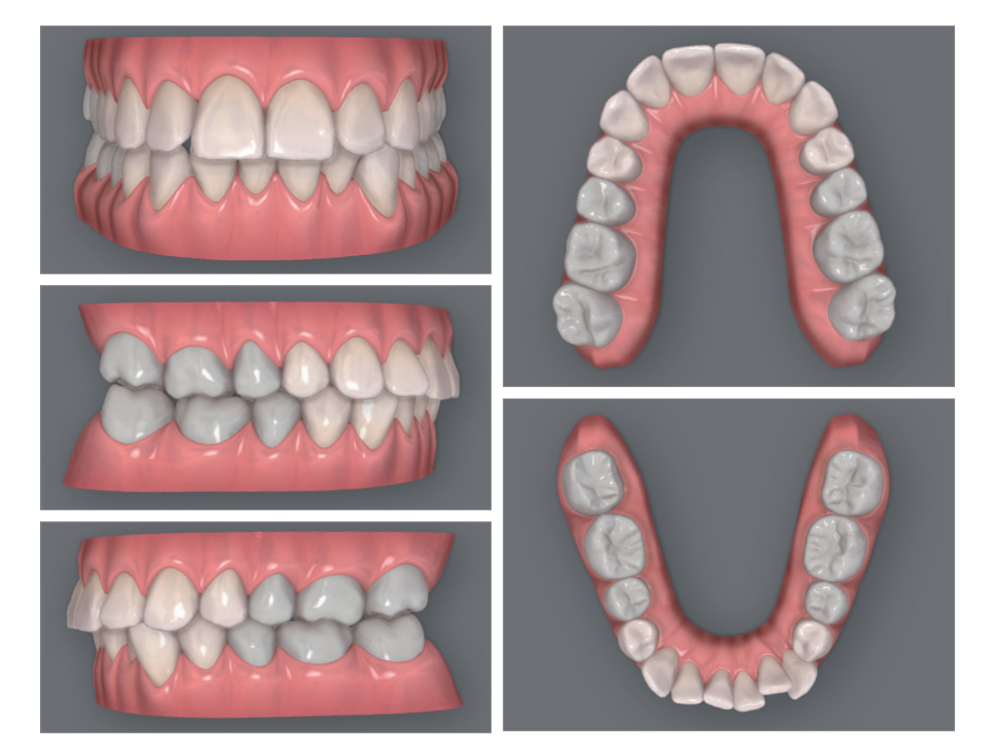
The 35-year-old female patient presented with skeletal Class II, a brachyfacial biotype, molar and canine bilateral Class I, 1.5 mm inferior dental midline left shift, a misaligned tooth #33 with no space in the arch, a buccally inclined tooth #12, external root resorption of teeth #26 and 46, bilateral disc displacement with reduction, nasal breathing and a Class I soft-tissue profile. The main concerns were the inferior crowding and midline shift.
The treatment with the Invisalign Lite Package started with intra- and extra-oral photographs from the patient, taken with the Invisalign Photo Uploader app using an iPhone XS (Apple). Panoramic, bitewing and profile radiographs of the patient were requested, and an addition - cured silicone impression was taken in one step using both light-bodied and putty consistencies to obtain as many details as possible. The impression trays were sent to Invisalign, and all the records were uploaded to the patient archive on the Invisalign Doctor Site, from which a clinical prescription was generated.
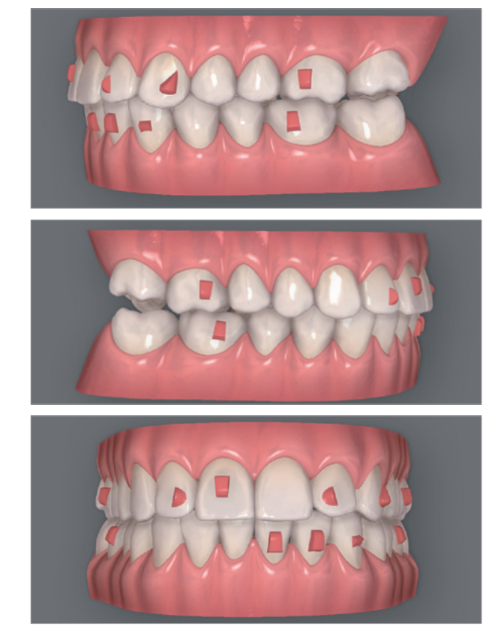
The original ClinCheck treatment plan consisted of eight maxillary active aligners and 14 mandibular active aligners. There were also passive maxillary aligners included. The crown of tooth #33 would move lingually with proclination to solve the crowding of the incisors. The patient was instructed to wear the aligners for 22 hours each day, using the first and second aligners for two weeks each and the rest of the aligners for one week each.
After the first treatment plan had been completed 16 weeks later, there was still buccal inclination of tooth #12 and its root was lingually positioned. In addition to this, the mandibular aligner tracking was far from ideal, owing to insufficient use on the part of the patient.
A new ClinCheck was generated to correct these problems, resulting in 14 new active aligners (seven maxillary and seven mandibular). I also asked the technician for three overcorrection aligners for each arch in order to obtain alignment of the teeth.
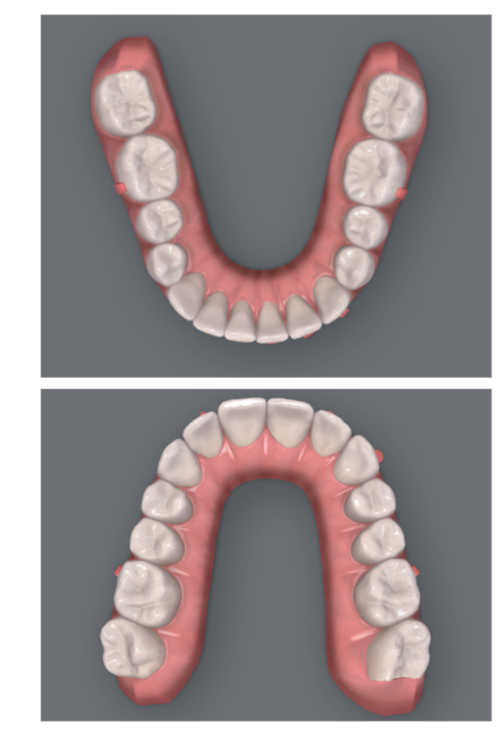
After nine more weeks, the treatment was completed, obtaining good alignment of the teeth and correcting the midline shift. A posterior open bite was generated in the molar region, which began correcting spontaneously after one month of fixed anterior retainers.





Patient 2–treated with in-office aligners
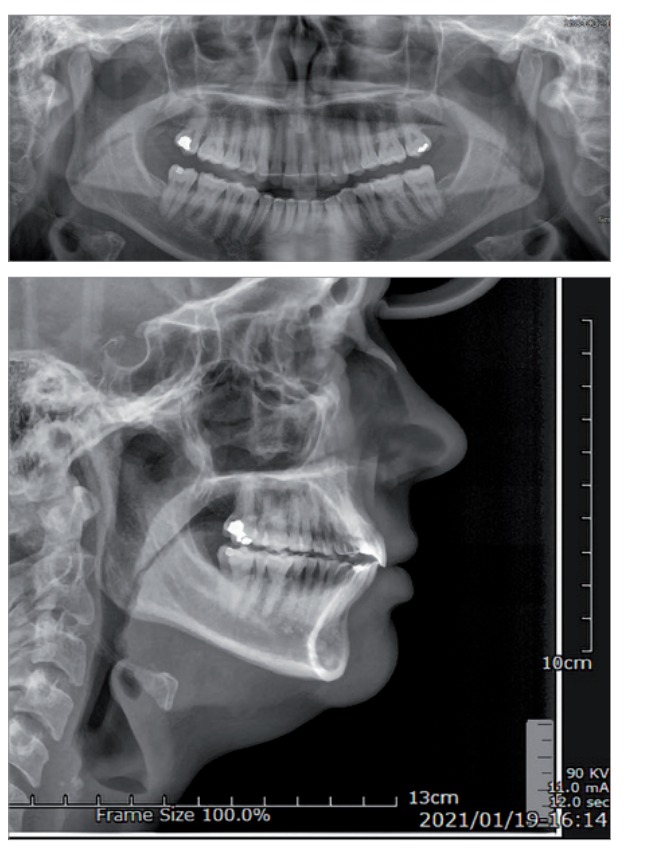
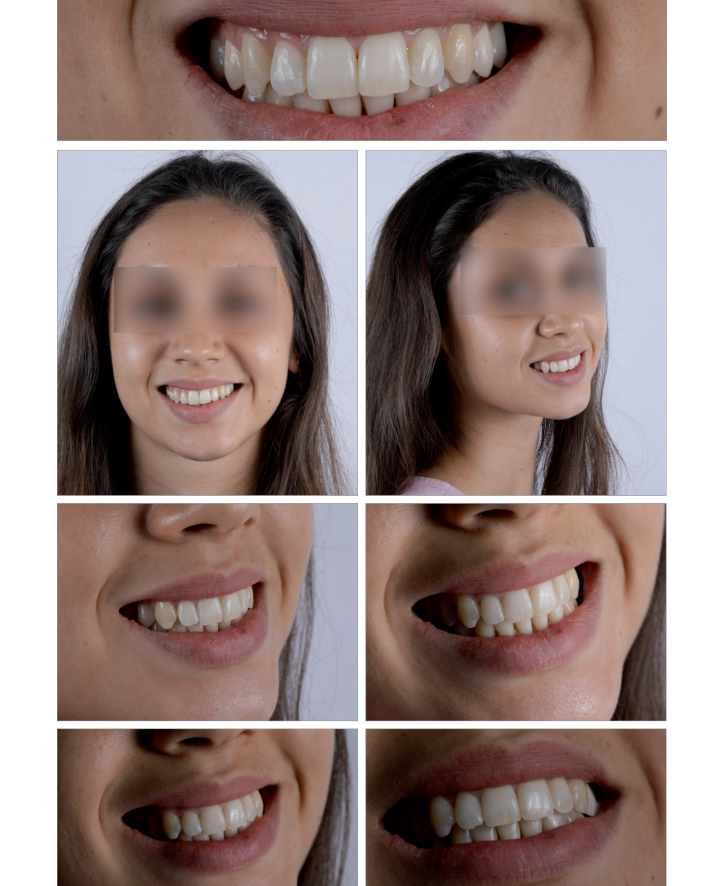
The 29-year-old female patient presented with skeletal Class II, a brachyfacial biotype, maxillary plane canting, molar and canine bilateral Class I, a light deep bite, palatal inclination of the maxillary incisors, moderate maxillary and mandibular crowding, a thin mandibular anterior gingival biotype, nasal breathing and a Class II soft-tissue profile. The main concern was the lingually inclined maxillary teeth.
Both intra- and extra-oral photographs were taken with a D3200 reflex camera (Nikon) using a twin flash. Panoramic, bitewing and profile radiographs of the patient were requested, and an addition-cured silicone impression was taken in one step using both light-bodied and putty consistencies. A cast model was obtained and then scanned. The STL file obtained from this model was uploaded to the Ortho Analyzer software (3Shape).
Essix 0.5 mm thermoplastic sheets and a BIOSTAR vacuum (SCHEU-DENTAL) were used to fabricate the aligners. This process, together with the trimming and polishing of the margins, was performed by a trained technician. The patient was instructed to use each aligner for two weeks, totalling a treatment time of 24 weeks.
After the treatment, the overbite and overjet values had improved with the alignment of the anterior teeth. Both the molar and canine Class I had been maintained, and no posterior open bite was generated by the bite block effect of the aligners.






Discussion
Both clinical cases had many characteristics in common, the most important for me being the patients’ biotypes. A brachyfacial biotype is known for having short muscle fibres with the capacity of generating much greater masticatory force than a mesofacial or dolichofacial biotype, and this could result in a posterior open bite after the use of clear aligners.
In addition, both patients presented with nasal breathing, which would assure biomechanical behaviour characteristic of their biotype rather than that of a dolichofacial biotype, which could have been the case if one of them was a mouth-breather.
Conclusion
Clear aligners have been shown to be as effective, and in some cases more efficient, than fixed appliances, and they constitute a completely different area of knowledge regarding biomechanics and treatment planning than what we have known before. The decision to use different commercial brands of aligners should be determined nowadays by the complexity of the case, Invisalign being the gold standard at the moment. Nevertheless, patient compliance regarding the number of hours of use per day remains one of the most important factors for achieving optimal results.
In the case of other brands, the thermoplastic material used is vital, because it will determine the way the force is applied to the teeth. In combination with excellent orthodontic software, the appropriate thermoplastic material can produce a predictable appliance for treatments that can accomplish the goals of both clinician and patient.