A non-surgical orthodontic approach using clear aligners in a Class III adult patient
Introduction
Over the past decade, there has been a notable surge in the use of clear aligners, and their benefits and advantages have been extensively documented. Nowadays, aligners can address a wide range of malocclusions, and the complexity of cases that can be effectively treated with aligners has increased remarkably.
Orthodontists face a challenging task when it comes to treating skeletal Class III malocclusion. This condition can lead to functional and aesthetic issues for patients. According to the severity of the malocclusion, treatment options vary from orthognathic surgery combined with orthodontics for the most severe cases to compensatory strategies involving dental extractions and employment of elastics in camouflage orthodontic treatment. When determining the most appropriate treatment approach, it is crucial to take into consideration not only the severity of the malocclusion but also factors such as facial profile, growth potential, the patient’s wishes and the reason for seeking medical advice.
When asymmetries are present in addition to skeletal Class III malocclusion, the management of the case becomes more complex. Asymmetric movements like distalisation may be necessary to compensate. While distalisation with fixed appliances can be challenging, clear aligners offer a reliable solution for achieving this movement. This article aims to present a case of a patient with a vertical skeletal Class III malocclusion treated successfully through asymmetric distalisation using clear aligners and Class III elastics.
Case report
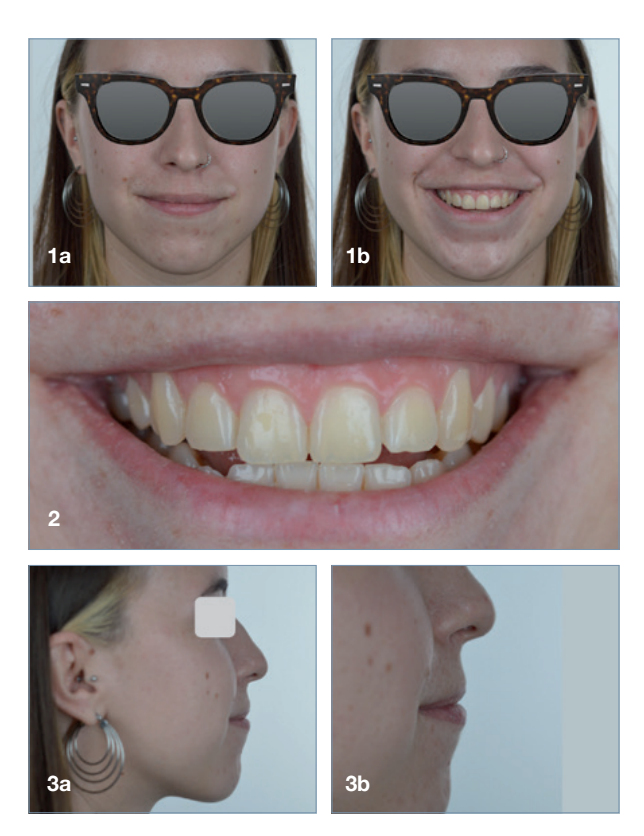
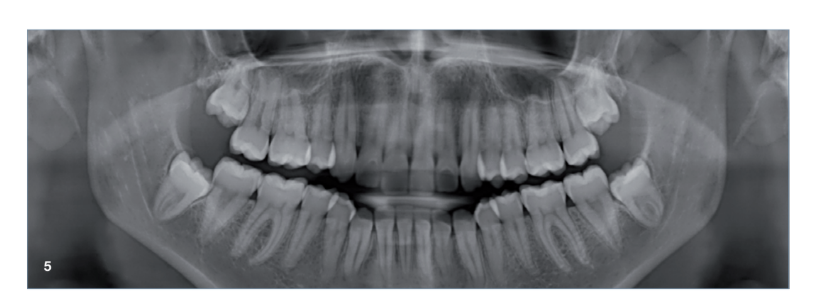
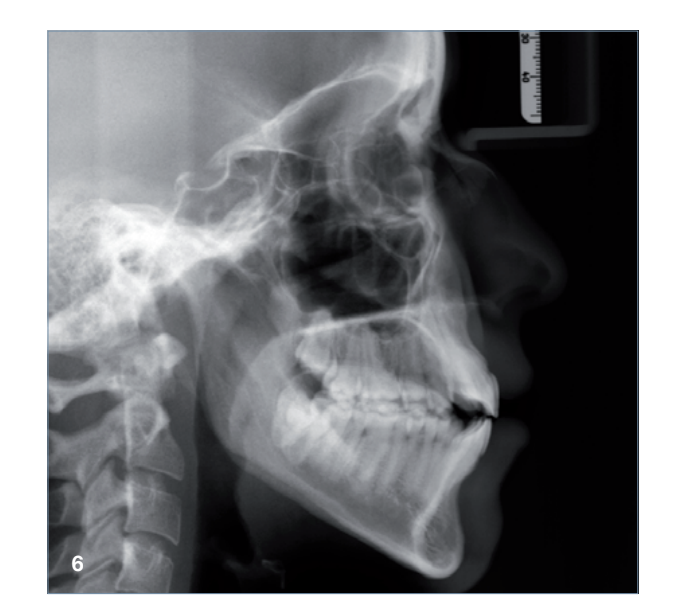
The 23-year-old dolichofacial female patient complained of not being able to chew properly. Facial examination showed a convex profile, an enlarged lower facial height, and a skeletal Class III malocclusion (Figs. 1–3). Intra-oral examination revealed an Angle Class III right subdivision malocclusion, anterior open bite, no overjet and a maxillary dental midline deviated about 3 mm to the right compared with the mandibular dental midline (Fig. 4). The panoramic radiograph confirmed previous extraction of the maxillary right first premolar and the presence of all four third molars (Figs. 5 & 6).

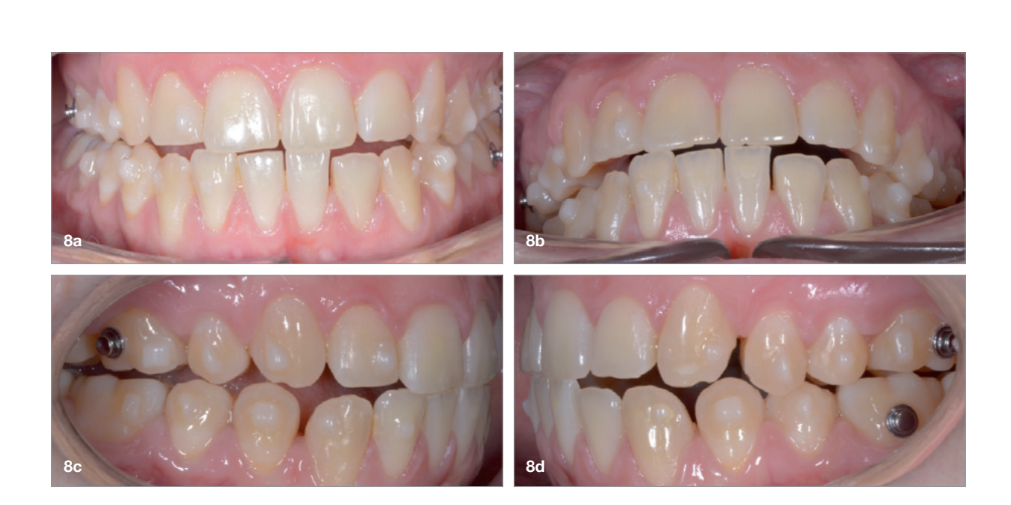
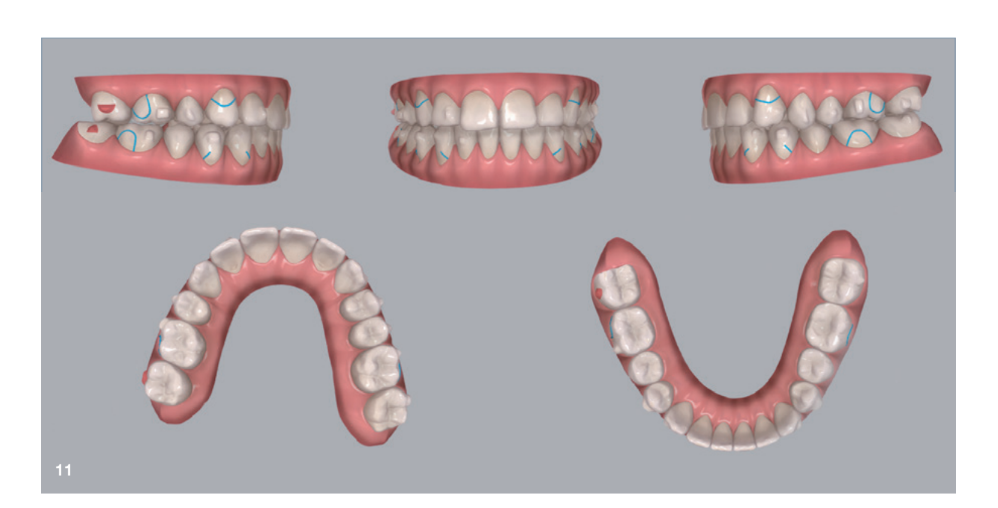
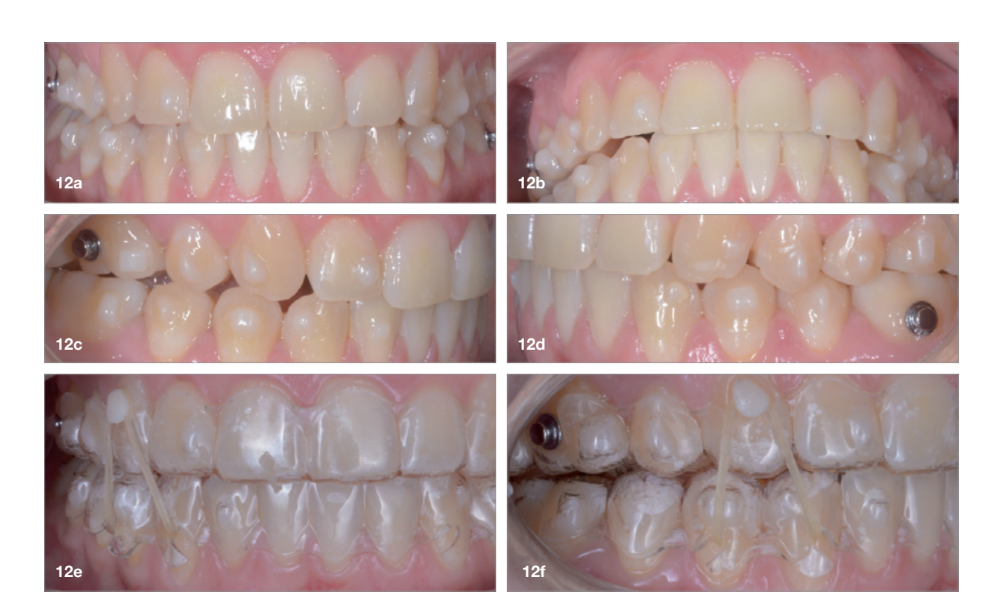
The treatment objectives included closing the anterior open bite, achieving a bilateral Angle Class I relation- ship and a proper overjet and overbite, correcting the midline discrepancies, and achieving a profile harmonisation. The treatment plan consisted of orthodontic camouflage treatment with asymmetric distalisation in three of the four quadrants using Invisalign aligners (Align Technology) and third molar extraction. The Invisalign Comprehensive package was chosen, and 63 pairs of aligners were used (Figs. 7–10). Each aligner was worn for 20 hours a day for one week each. The use of Class III elastics on both sides was indicated. Afterwards, ten refinement aligners were needed to improve the interdigitation on the right side (Figs. 11 & 12).



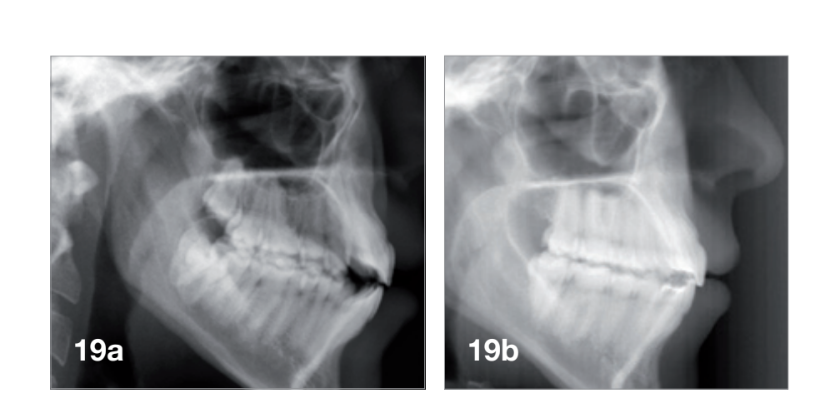
Although Class III elastics tend to extrude the maxillary molars and generate clockwise mandibular rotation, aligners allow us to prevent these complications, since we have better control over tooth movement, enabling us to counteract unwanted dental movements. In this case, an intrusion of the posterior teeth was planned, which would generate anticlockwise rotation of the mandible in an anticlockwise direction. This vertical control led to the closure of the anterior open bite and the reduction of the lower facial height, thereby improving the facial profile.
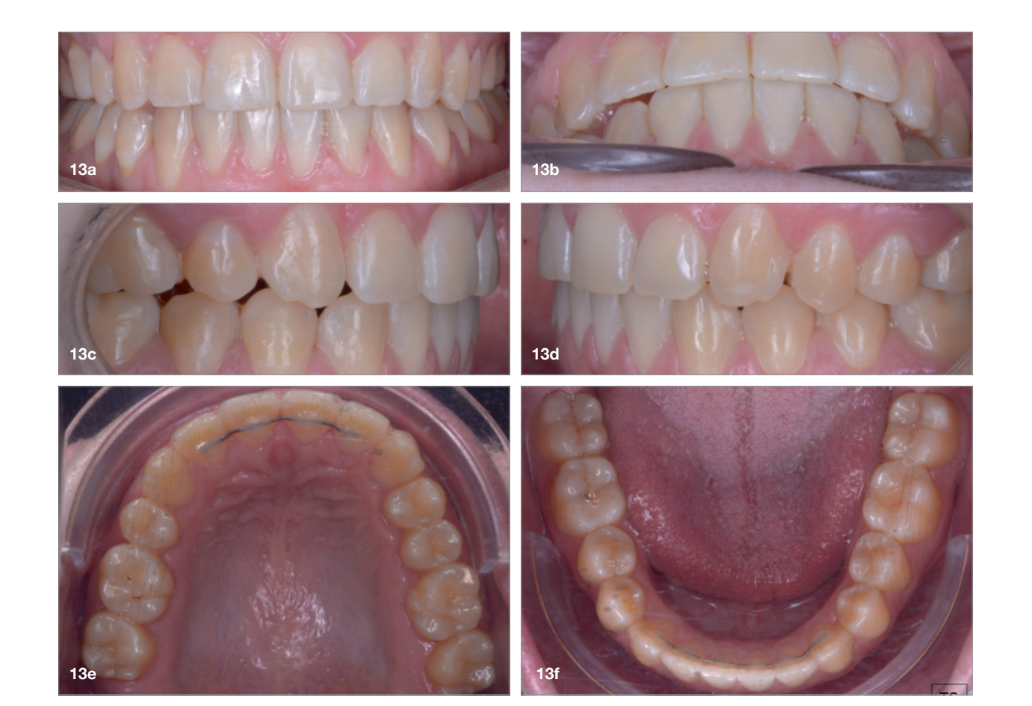
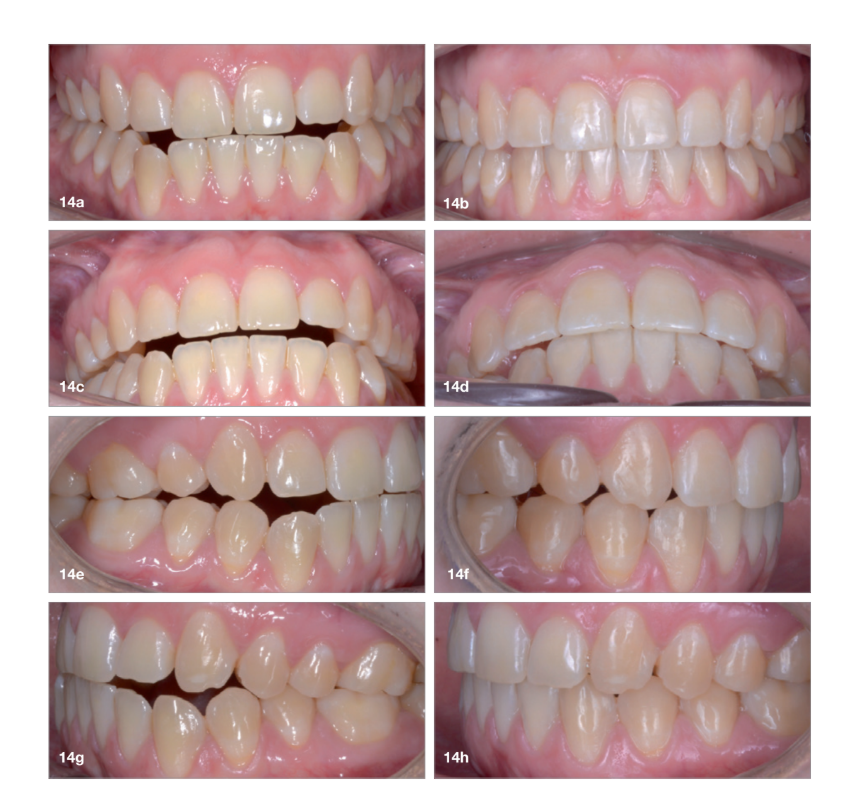
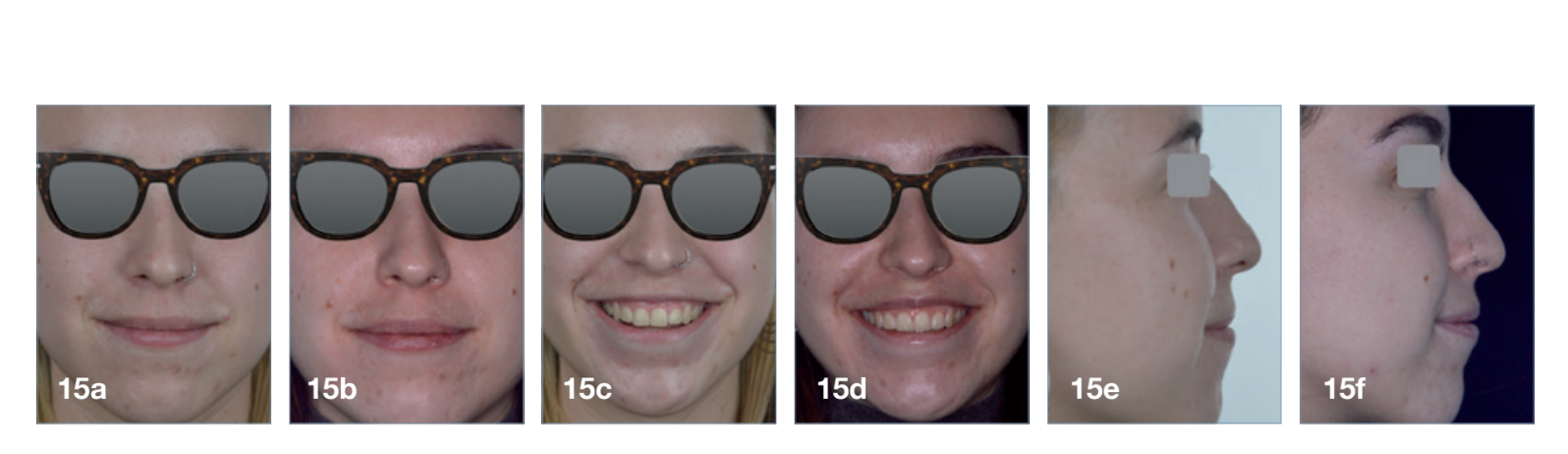
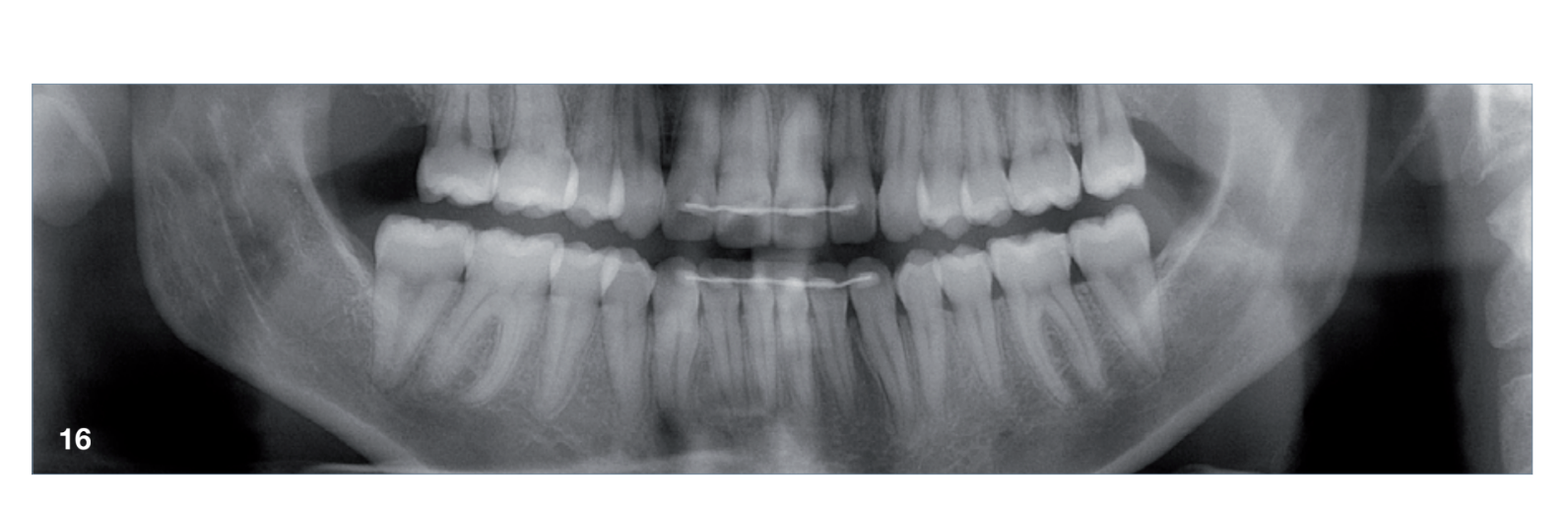
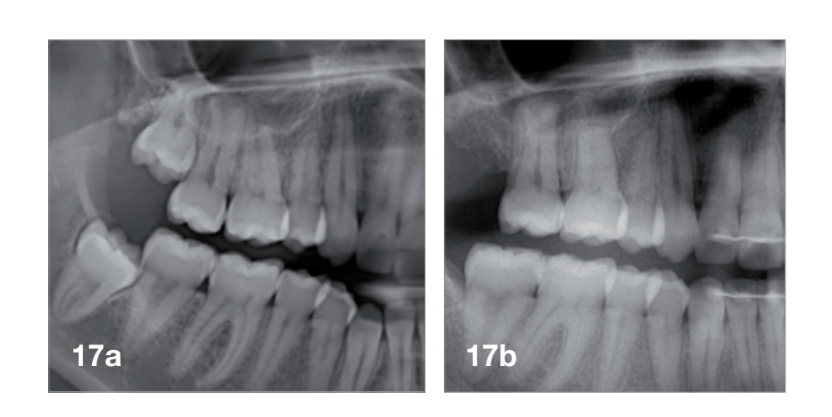
The total treatment time was 15 months. An Angle Class I relationship was established along with adequate anterior and canine guidance, establishing a functional occlusion. This not only ensures optimal masticatory function but also protects the teeth and the temporomandibular joint from excessive force. Maxillary and mandibular fixed retention were installed at the end of the treatment (Figs. 13–19).

Conclusion
This case report has shown that, with a comprehensive diagnosis, proper planning and patient compliance, aligners aided by elastics are an effective and efficient treatment alternative for correcting asymmetric Class III malocclusion. Aligners allow efficient distalisation in patients with anterior open bite or hyper-divergent patterns while minimising the risk of worsening the vertical problems.