
Orthodontics and botulinum toxin: Integrated care of a patient with bruxism and occlusal alteration
Introduction
Hypertrophy of the masseter muscle is defined as the excessive growth of muscle mass in the transverse direction and is more common between the second and fourth decades of life. Even though its aetiology is multifactorial, bruxism is the main cause. There are many treatment alternatives, among which injection of botulinum toxin into the masseter muscle has been shown to be a safe and effective option.
Botulinum toxin is a powerful neurotoxin that, when injected into the muscle, generates interference with the neurotransmitter mechanism, inhibiting the release of acetylcholine at motor neuron axon terminals and thereby producing selective paralysis, decreased contraction and consequent muscular atrophy. It is this last effect that is exploited for addressing hypertrophy of the masseter, reducing its size and improving the patient’s aesthetics.
There is extensive literature on the parameters that must be followed for the injection of botulinum toxin to avoid risk areas and to reduce complications. In 2005, Kim et al. delineated a safe zone for the injection of botulinum toxin, demarcated vertically by the anterior and posterior boundaries of the masseter muscle and horizontally by a line drawn along the inferior border of the mandible to the mandibular angle and a line drawn from the base of the earlobe towards the corner of the mouth. In 2010, Kim et al. determined the subdivision of the masseter muscle into six zones, according to which injection into Zones I, II and III would be associated with adverse effects, such as injury to the parotid duct, and injection into Zone VI would not be effective for masseteric hypertrophy, establishing Zones IV and V as safe for botulinum toxin injection.
Case report
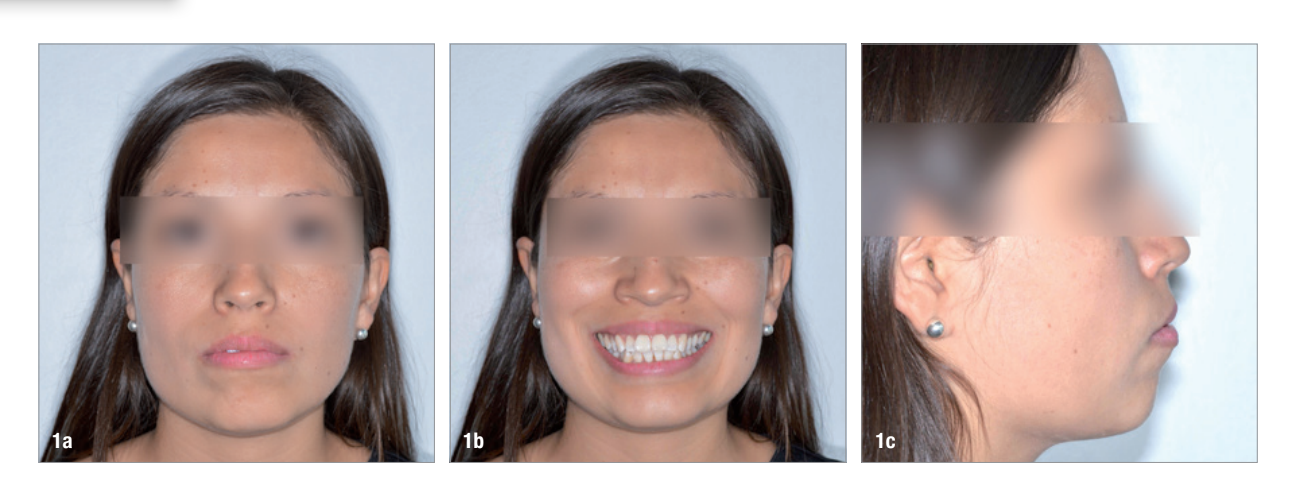
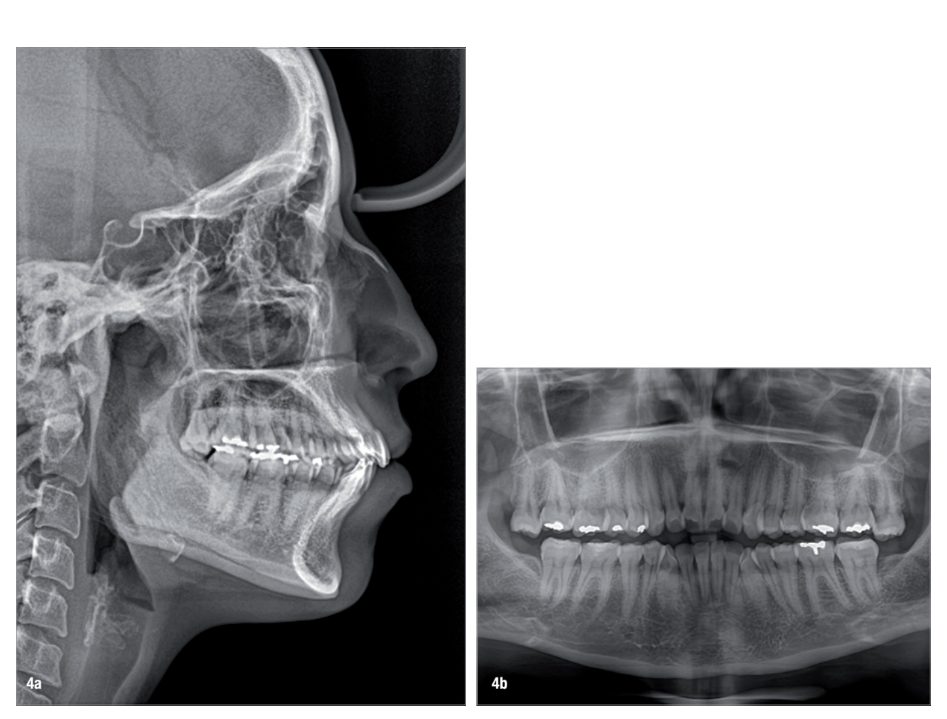
A 35-year-old female patient presented with crowding, muscle and joint pain, and headaches upon awakening. Examination found a skeletal Class I with crowding and bimaxillary protrusion. Facial examination showed a convex profile with protruded lips and a square face shape, intensified on smiling (Figs. 1–4). She reported bruxism, and bilateral masseteric hypertrophy was observed, but there was no alteration of the temporomandibular joints.


The objectives of the treatment included correcting the crowding, establishing a Class I occlusion, correcting the patient’s profile and reducing bruxism, along with its associated signs and symptoms. Orthodontic treatment using aligners was planned, together with the administration of botulinum toxin for the bruxism signs and symptoms and to improve the facial aesthetics.
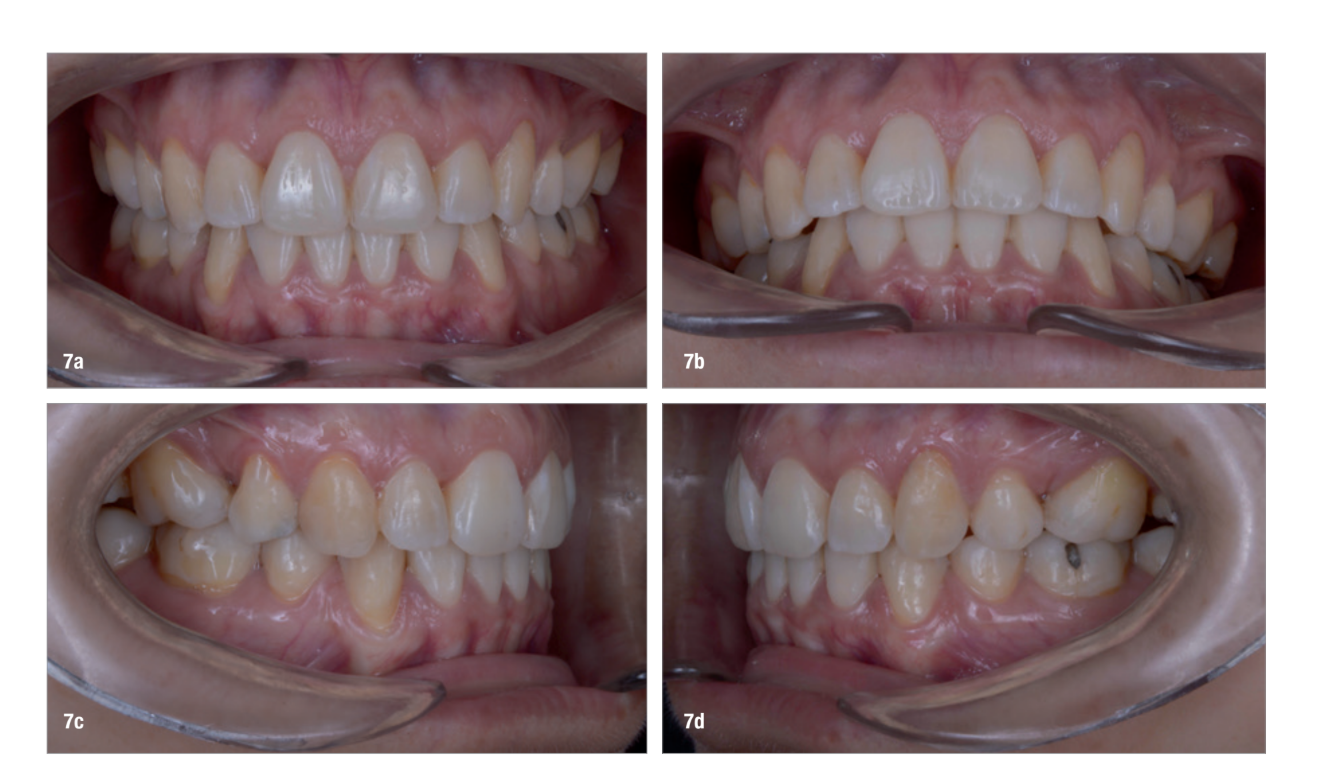
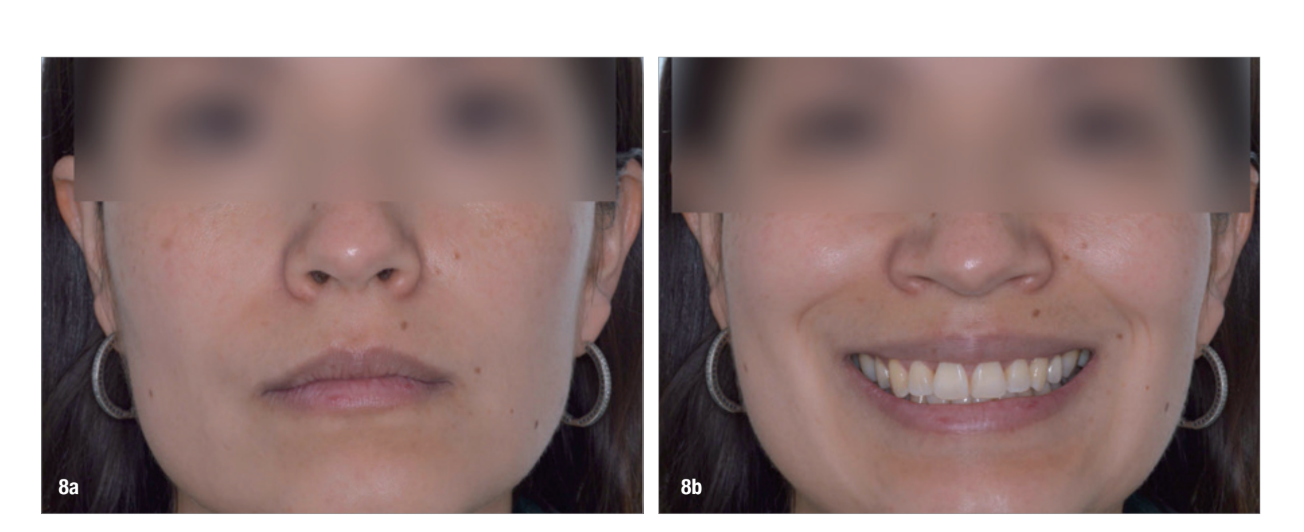
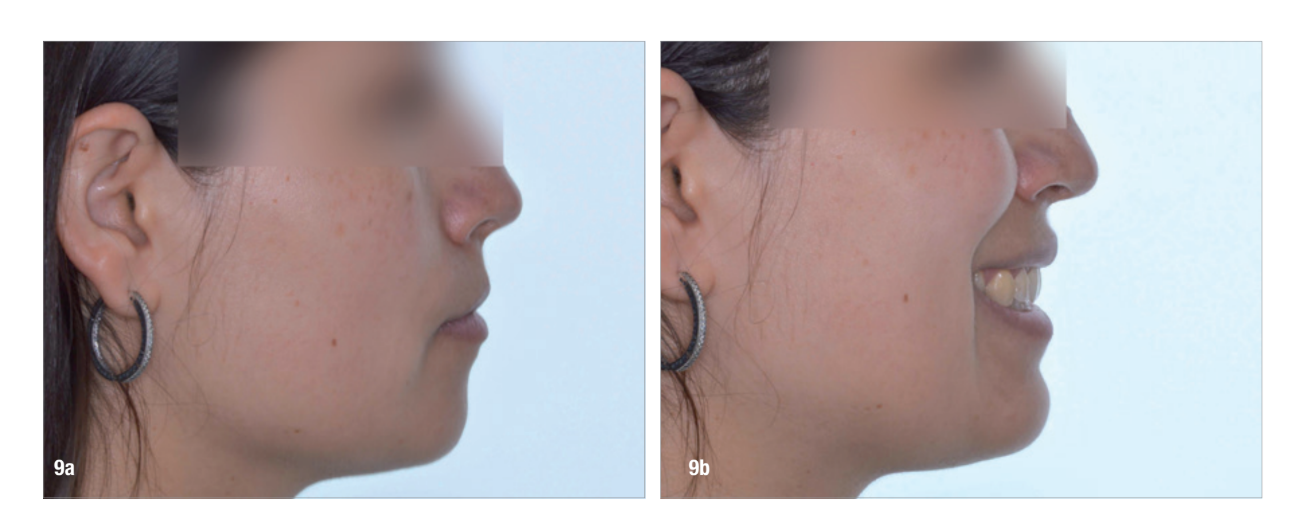
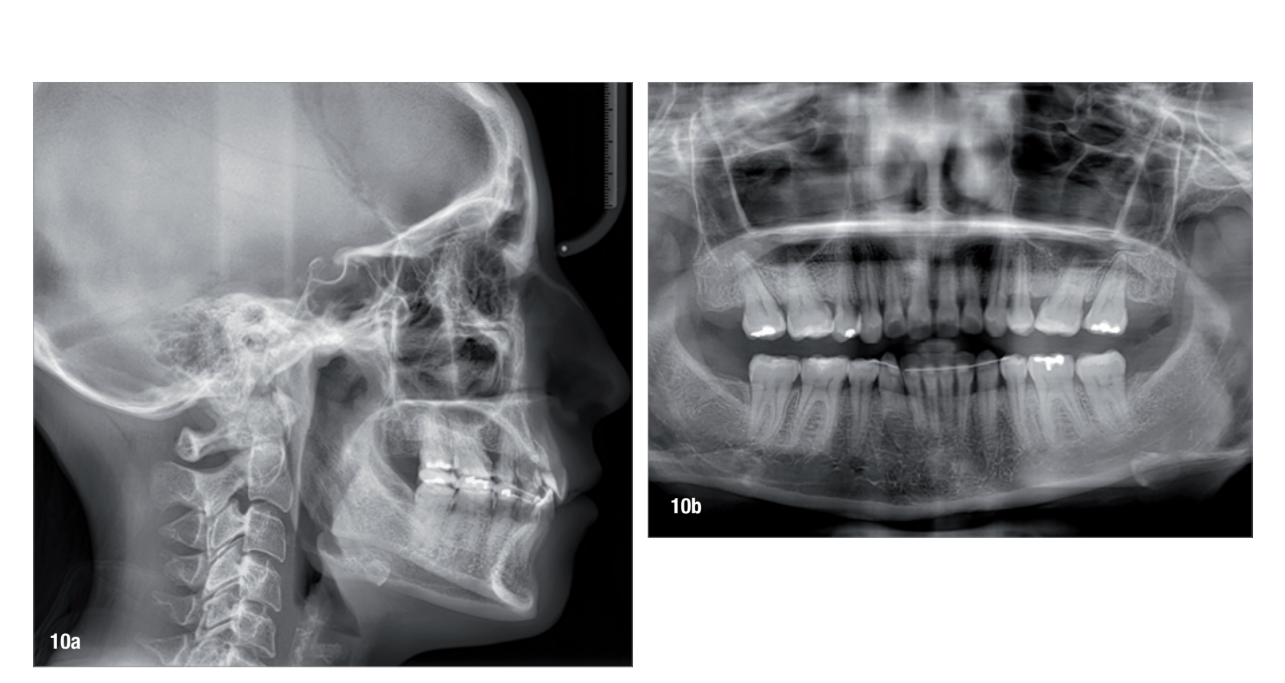
Before the aligner treatment began, the maxillary and mandibular second premolars were extracted to create space. With orthodontic treatment, distalisation of the anterior teeth was achieved by employing maximum mandibular anchorage and moderate maxillary anchorage (Figs. 5–7). At the end of the treatment, a stable bilateral Class I occlusion had been achieved, as well as normal inclination and retrusion of the anterior teeth, consequently improving the profile (Figs. 8–10). Among the post-treatment recommendations was a mouth guard, which the patient was advised to wear every night to protect the teeth from the excessive occlusal force of bruxism.


Once the orthodontic treatment had been completed, botulinum toxin was injected bilaterally into the masseter muscle and an anterior portion of the temporalis muscle. In the first session, three injections were performed in the masseter muscle, administering 2.5 U in the most superior point and 5.0 U in each of the two lower points, a total of 12.5 U per masseter. Then, 10 U of botulinum toxin was injected into the anterior portion of the temporalis muscle in this same session. After 14 days, a second session was performed. Because the patient presented with slightly greater hypertrophy on the right side compared with the left side, 5.0 U of botulinum toxin was injected into the right masseter and 2.5 U into the left masseter.
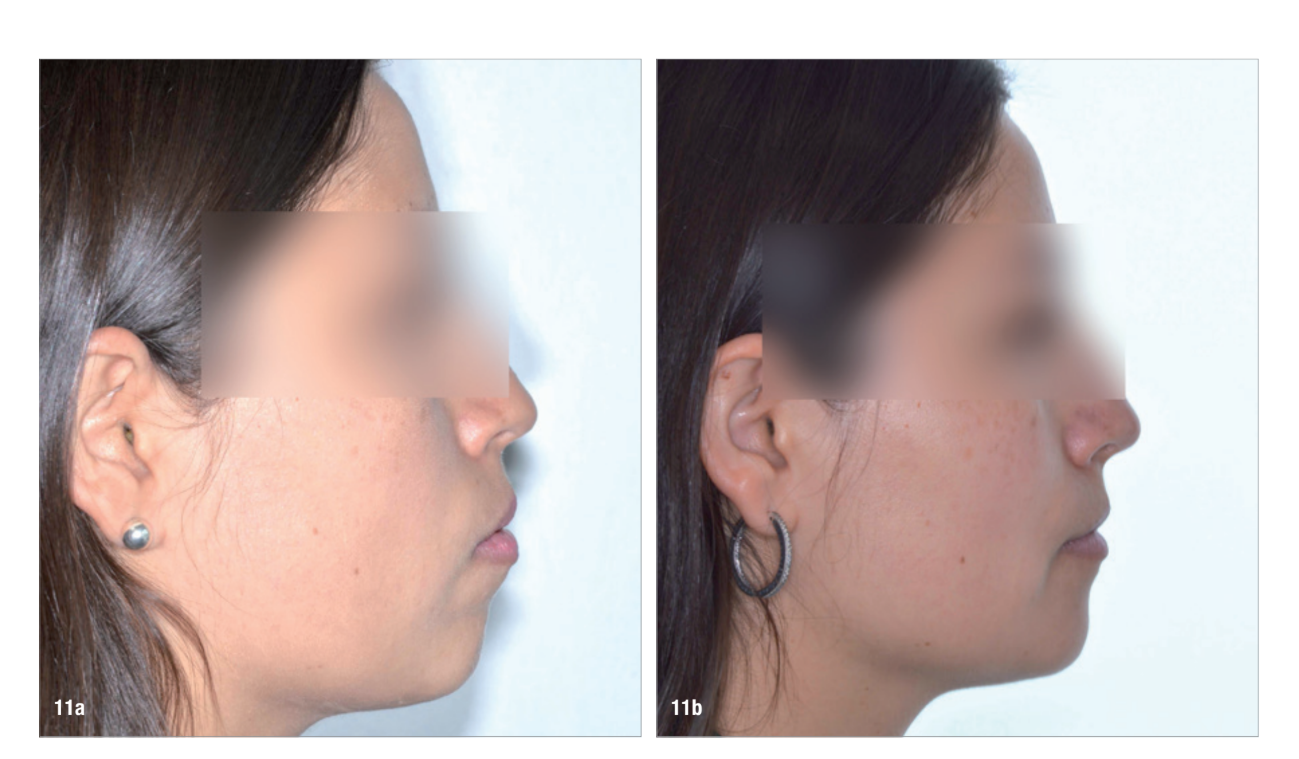
At the end of the treatment, the patient showed a significant improvement in her profile thanks to the orthodontic treatment (Fig. 11) and an improvement in her facial shape thanks to the injection of botulinum toxin into the elevator muscles (Fig. 12). She also had a decrease in bruxism and its symptomatology thanks to the combination of both treatments.

Conclusion
This case report demonstrates that a comprehensive and holistic approach to treatment is essential to achieve the desired outcomes for the patient. Neither of the two treatments alone could have resolved the patient’s complaints at the first consultation, demonstrating the importance of listening carefully to the patient during his or her first appointment to understand his or her concerns and expectations and using all the treatment options available not limiting treatment to one specialty.
Authors: Drs Tomás A. Salazar, Belen M. Perretta, Camila Reino & Kristen Kock, Chile
References:
- Aragón Niño Í, Niño Aragón ML, Pampín Martínez MM, del Castillo Pardo de Vera JL, Cebrián Carretero JL. Tratamiento de la hipertrofia del músculo masetero con toxina botulínica. Consideraciones y manejo [Treatment of masseter muscle hypertrophy with botulinum toxin. Considerations and management]. Med Estética. 2022 Jun 15;71(2):45–50.
- Kim NH, Chung JH, Park RH, Park JB. The use of botulinum toxin type A in aesthetic mandibular contouring. Plast Reconstr Surg. 2005 Mar;115(3):919–30.
- González Magaña F, Miranda LM, Malagón Hidalgo H, González Amesquita V. Uso de toxina botulínica para tratamiento de la hipertrofía del músculo masetero [Use of botulinum toxin for treatment of hypertrophy of the masseter muscle]. Cir Plast Ibero-Latinoam. 2012 Jul–Sep;38(3):297–302.
- Fedorowicz Z, van Zuuren EJ, Schoones J. Botulinum toxin for masseter hypertrophy. Cochrane Database Syst Rev. 2013 Sep 9;2013(9):CD007510.
- Kim DH, Hong HS, Won SY, Kim HJ, Hu KS, Choi JH, Kim HJ. Intramuscular nerve distribution of the masseter muscle as a basis for botulinum toxin injection. J Craniofac Surg. 2010 Mar;21(2):588–91.