
Anatomical and topographical variability of the root canal orifices in maxillary molars
Machine translation
Original article is written in RU language (link to read it) .
Abstract. The application of a navigation-optical approach to determining the orifices of the root canals of maxillary molars is a relevant task at the stages of endodontic treatment. In this regard, retreatment or re-treatment of the tooth's root system is aimed at eliminating pathological defects in the periapical area. The goal is to study the variations in the location of the orifices of the root canals in maxillary molars during endodontic treatment.
Materials and methods. A total of 435 patients aged 18 to 75 years were examined for complicated caries and re-treatment of teeth. Endodontic treatment was performed on 450 teeth in the maxilla, including 301 first molars and 149 second molars. The treatment was conducted using a dental microscope with a digital camera. The orifice of the root canal was considered to be a depression on the surface of the cavity floor or in the location of the fissure connecting the orifices of the root canals of one root, with the possibility of performing instrumental treatment of one root canal for at least 1/3 of its length. The location of the root canals was confirmed by electronic apex locators and targeted radiographic images.
Results. The analysis of photoprotocols showed variability in the configuration of the root canal orifices at the bottom of the tooth cavity. Four navigational-anatomical variants were identified during the formation of the endodontic access: 1) "mesial groove"; 2) "linear anatomy"; 3) "square anatomy"; 4) "T-shaped anatomy".
Conclusion. Determining the maximum number of root canal orifices in upper molars eliminates cases of missed canals. The application of a navigational-optical approach will help prevent the development of complications in the periapical tissues after the obturation of the tooth's root system.
Introduction
Endodontic treatment for pulp inflammation aims to prevent the development of inflammatory processes in the periodontal tissues. In apical periodontitis, treatment involves eliminating the focus of chronic infection and creating conditions for the restoration of the periapical area. One of the important prognostic factors affecting the quality of endodontic treatment is determining the maximum number of root canal orifices, followed by complete passage and obturation of the tooth's root system. According to cone-beam computed tomography (CBCT), research results for determining prognostic factors showed a direct correlation between missed root canals and the development of apical periodontitis.
A study by a group of researchers from the University of Pennsylvania (2016), aimed at a retrospective assessment of the relationship between the prevalence of apical periodontitis and missed root canals, indicates that this problem is most often associated with the first and second molars of the upper jaw. More than 40% of upper jaw molars diagnosed with "apical periodontitis" had missed root canals. Research results showed that in most cases among the missed root canals, the second mesiobuccal canal (MB2) in the mesial root was present. As a reason for this, the authors point to the problem of visualizing the floor of the tooth cavity when searching for the orifices of the root canals.
According to a meta-analysis by J. Martins et al., the presence of MB2 showed high variability and dependence on the region of study. For example, the prevalence of MB2 in first molars is noted in 96% of cases in Belgium and in 30.9% of cases in China. In this regard, the average value of the number of root canals cannot be applied to a specific geographical region.
It should be noted that one of the important factors in evaluating scientific research dedicated to the topography and quantity of root canals is the methodology used. Authors often use different definitions of anatomical elements that they consider to be root canals. Some authors visualize the root canal as a separate entity that topographically begins separately from the other canals at the bottom of the tooth cavity and has its own apical foramen. In other works, the root canal is defined only as a separate opening at the bottom of the tooth cavity or as a canal that can be instrumentally treated to a depth of 3-4 mm separately from other canals.
However, the authors do not take into account that broader sections of a single slit-like canal can be accepted as root canals, which may merge into one during instrumental treatment. At the same time, a root canal that starts with one opening may split into two or more root canals at varying depths. However, studies on the topography of the distobuccal and MB2 canals have been conducted in a CT navigation design without considering the optical visualization of the location of the openings.
When determining the canals on CBCT in the second upper molar, X. Han et al. (2012) considered the number of root canals and the angle formed between the palatal, distally buccal, and mesially buccal canals (PDM angle) [22]. According to their data, 71% of second upper molars have a PMD angle ranging from 110 to 130°, indicating an elongated shape of the tooth cavity and a tendency for the distally buccal canal to approach the line connecting the mesially buccal and palatal canals. As noted by the authors, about 2.5% of distally buccal canals were located almost on this line with a PDM angle ranging from 140 to 180°. The authors associate the reason for such a shift towards a more palatal position of the distally buccal root with processes occurring in the early stages of tooth development.
The effectiveness of determining the location of the root canal orifices is achieved using optical magnification with directed light. For determining the location of the root canal orifices during endodontic treatment, the use of an operating microscope is considered one of the effective tools. Research by S.I. Gajva et al. (2013) showed that the elimination of errors and complications during retreatment using an operating microscope was 1.96 times higher than when treated with standard methods, without the use of a microscope. In particular, the search for root canal orifices was found to be twice as effective and reached 100% in the observation group using the microscope.
The analysis of the literature dedicated to the problem of locating the orifices of root canals relative to the topography of the floor of the tooth cavity showed that practicing dentists use the recommendations proposed by P. Krasner and H. Rankow (2003). However, the recommended rules for locating the orifices of root canals are not always feasible, possibly due to the deposition of secondary dentin, calcification of the tooth cavity, or age-related changes. Poorly performed treatment of the tooth's root system can also lead to changes in the anatomy of the orifice part of the root canals, transportation, and perforations of the root canals, complicating the search for root canals.
In this regard, the application of a navigational-optical approach to determine the maximum number of orifices of root canals in maxillary molars, to exclude errors and complications in the long term, at the stages of endodontic treatment is a relevant task.
The aim of the study is to investigate the variations in the location of the orifices of root canals in maxillary molars during endodontic treatment.
Materials and Methods
435 patients aged 18 to 75 years were examined for complicated caries and re-treatment of teeth; endodontic treatment was performed on 450 teeth in the upper jaw (301 first molars, 149 second molars).
Endodontic treatment was carried out using a dental microscope with a light splitter and a digital camera to document each stage of treatment.
During the endodontic treatment of permanent molars in the upper jaw, after anesthesia, a rubber dam was placed to isolate the tooth. Then, the carious cavity was prepared, remnants of filling material were removed, followed by the formation of endodontic access. The identification of the root canal orifices was performed according to the rules proposed by P. Krasner and H. Rankow, based on anatomical landmarks, i.e., the orifices were located at the junction of the walls and the floor of the tooth cavity, according to the color rule and the rule of the location of canal orifices (Fig. 1).
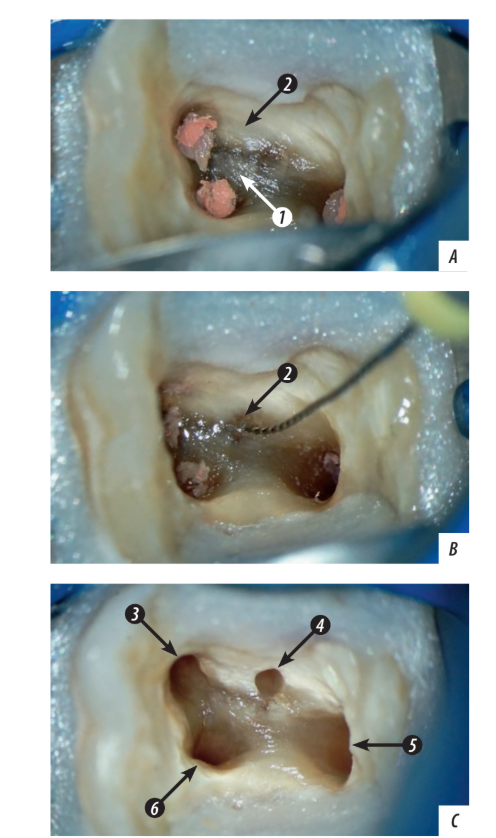
The orifice of the root canal was considered to be a single depression on the surface of the bottom of the tooth cavity or in the location of the fissure connecting the orifices of the root canals of one root, with the possibility of performing instrumental treatment of only one root canal for at least 1/3 of its length. Orifices that merged during instrumental treatment were counted as one slit-like canal. The division of the root canal into two or more canals below the orifice was considered as one orifice (root canal). The location of the root canals was confirmed by electronic apex localization and targeted radiographs to exclude perforation of the tooth cavity and the wall of the root canal. Depending on the clinical situation, treatment was carried out in one or two stages, with instrumental processing, irrigation, and obturation of the root canals under the control of targeted radiography. Subsequently, the coronal part of the tooth was restored according to the treatment plan.
Results
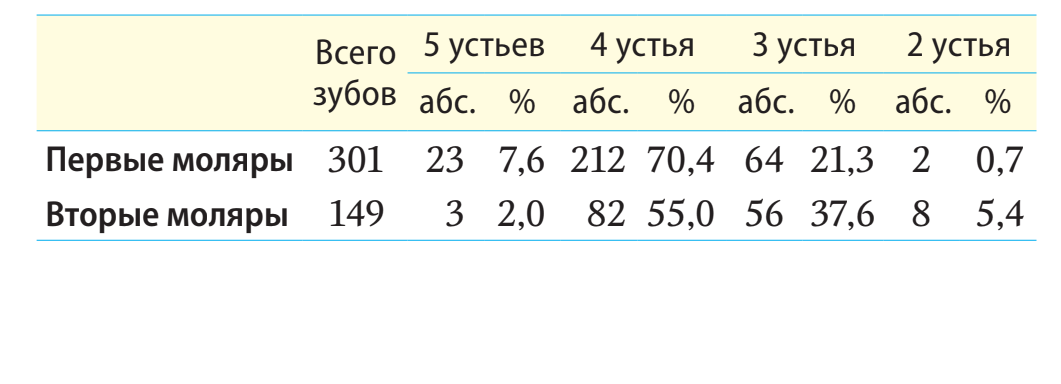
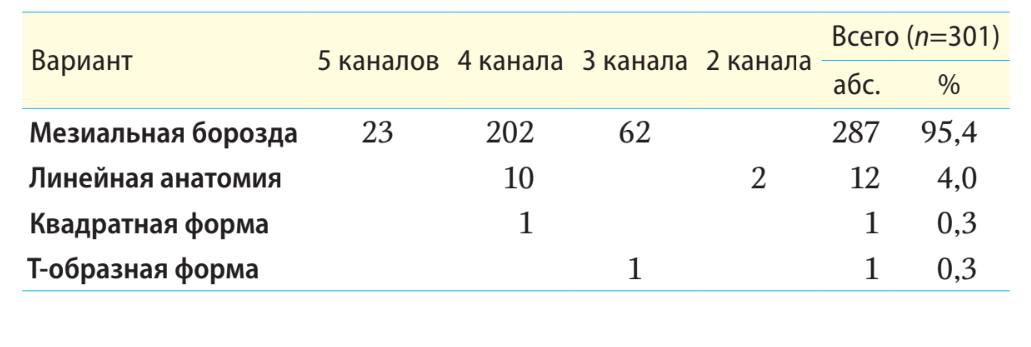
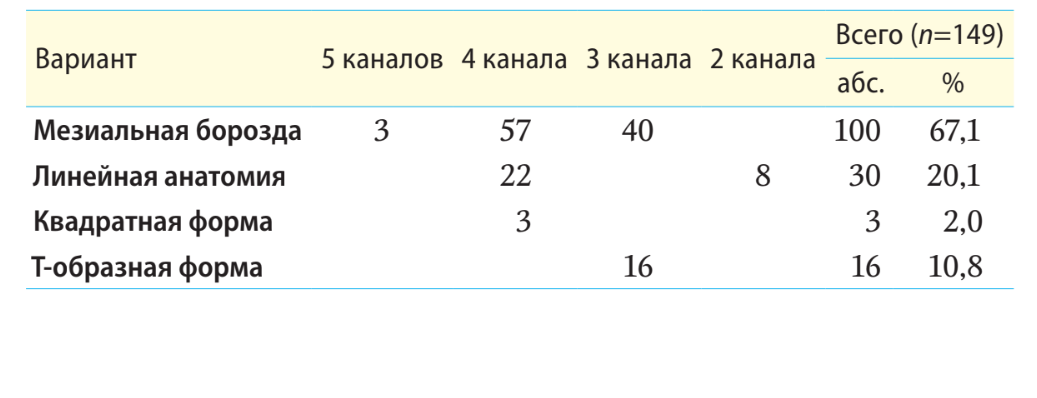
The analysis of the identification of the root canal orifices at the bottom of the cavity of 301 first molars of the upper jaw revealed that in 70.4% of cases, 4 root canal orifices were identified, in 21.3% of cases — 3 orifices, in 7.6% of cases — 5 root canal orifices, and 0.7% of cases had 2 root canal orifices. The second molars of the upper jaw (n=149) had 4 root canal orifices in 55% of cases, 2% had 5 orifices, 37.6% had 3 orifices, and in 5.4% of cases, there were 2 root canal orifices (Table 1).
The analysis of 450 first and second molars of the upper jaw based on photoprotocols in patients at the stage of forming endodontic access showed variability in the configuration of the locations of the root canal orifices at the bottom of the tooth cavity and allowed us to document the following navigational-anatomical variants of the location of the root canal orifices:
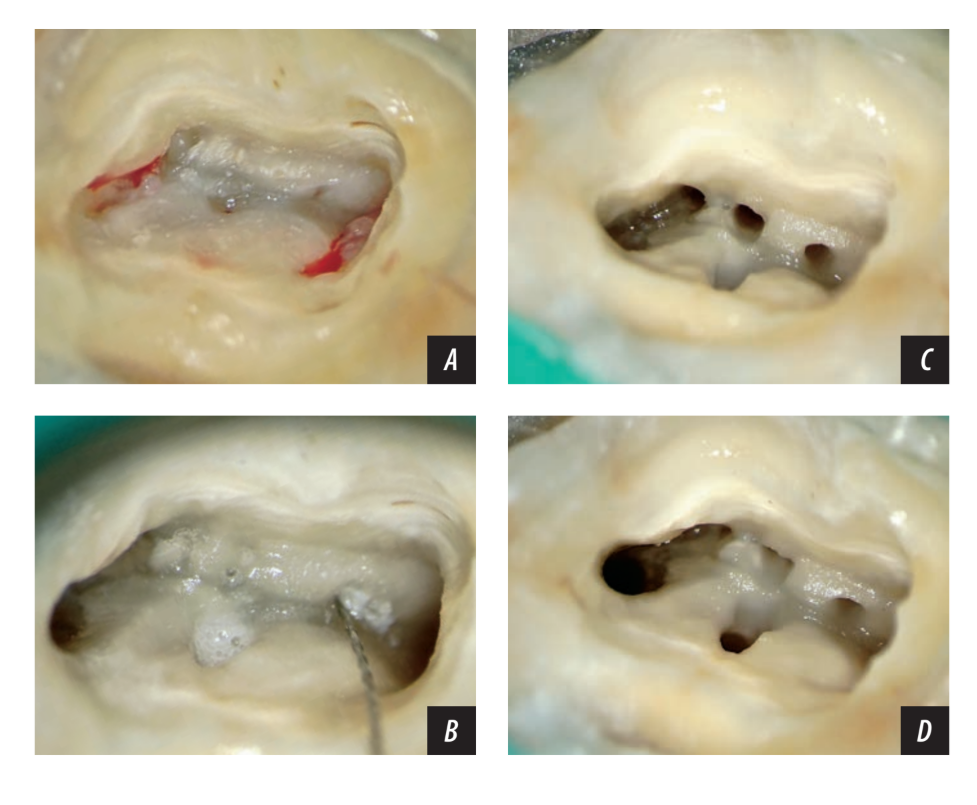
- “Mesial groove” — mesial buccal groove (where one to three root canal orifices may be located), distobuccal and palatal canals are located separately (Fig. 2).
- “Linear anatomy” — the location of two to four root canal orifices along a line connecting the mesial buccal and palatal canals (Fig. 3).
- “Square anatomy” — 4 root canal orifices located at the corners at the bottom of the tooth cavity in a rectangular shape, i.e., 2 buccal and 2 palatal root canals (Fig. 4).
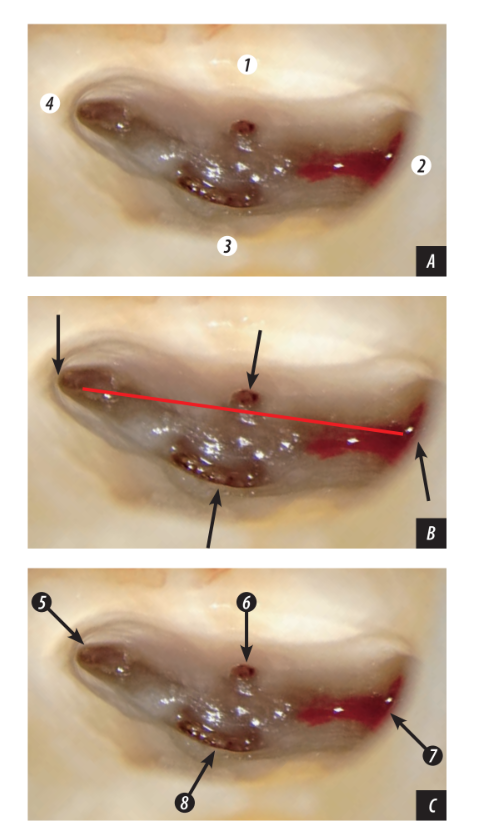
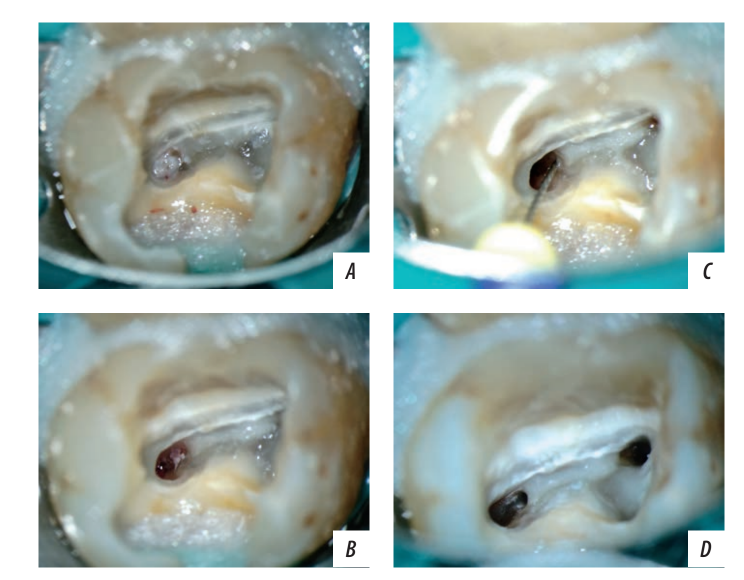
- “T-shaped anatomy” — the orifices of the mesial buccal and distobuccal root canals are located on a single line, perpendicular to the line drawn to the center of the palatal canal (Fig. 5).
The first variant "Mesial groove" was the most common — 95% of cases in the first molars and 67% of cases in the second molars of the upper jaw. The mesial-buccal groove is an anatomical formation in the form of a narrow fissure running along the mesial boundary of the tooth cavity floor and the mesial wall in the palatal direction. The mesial groove starts from the angle formed by the buccal boundary of the floor and the vestibular wall with the mesial boundary of the floor and the mesial wall. At this point, the orifice of the mesial-buccal canal is usually located, according to the rules of orifice localization.
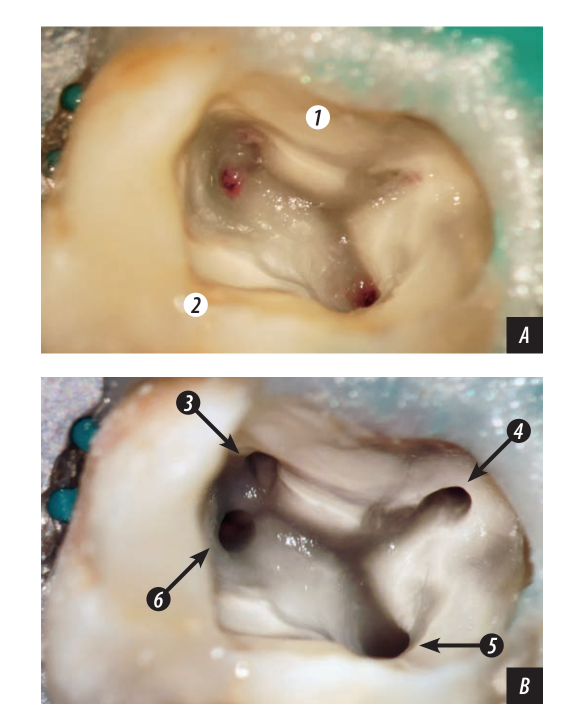
At the depth of the buccal groove, orifices of one or several canals may be located. Often, the groove itself represents a narrow long fissure, transforming into one oval slit-like canal (Fig. 6).
in the lumen of the mesial groove after instrumental processing
The second variant "Linear anatomy" consists of 4 separate orifices of the root canals: buccal-distal, buccal-mesial, second mesial-buccal, and palatal canals. The orifices of the mesial-buccal and palatal canals are anatomically located at the ends of a straight line, while the orifices of the buccal-distal and second mesial-buccal (MB2) canals are near this line, sometimes opposite each other in the central part of this line. In the presence of three root canal orifices, the orifice of the buccal-distal canal is located as close as possible to the mesial-palatal line, with a PMD angle of 140°. The "Linear anatomy" variant occurs in 20% of cases of second molars and in 4% of cases of first molars of the maxilla. It should be noted that this is the most dangerous anatomical form in terms of missed canals. It is often mistaken for a two-canal variant with one mesial-buccal and one palatal canal, or the search for the orifice of the distal-buccal canal is conducted more vestibularly, in the distal-buccal direction, which leads to transportation and perforation of the floor of the tooth cavity.
The third variant "Square shape" is represented by four openings of the root canals: buccal, mesial, and distal, and two palatal — mesial and distal. The openings of the root canals form a quadrilateral shape. In this navigational-anatomical form, the second mesio-buccal canal (MB2) was not identified.
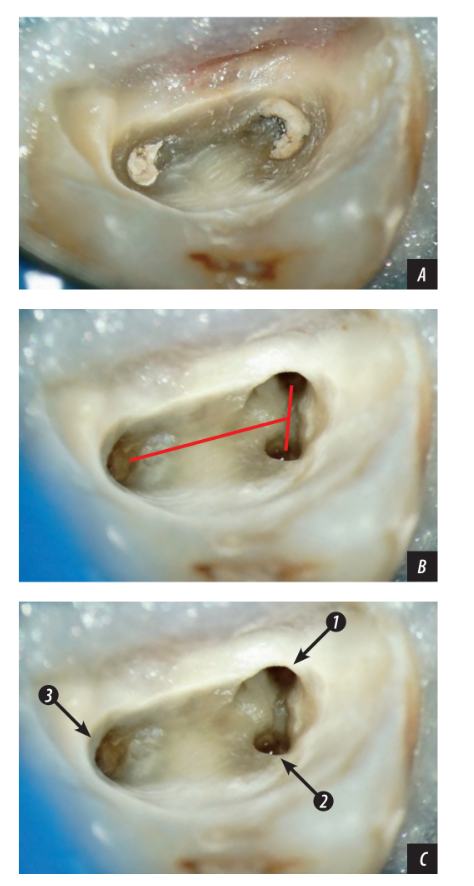
The fourth variant "T-shaped form" is represented by three canals — two buccal (MB and DB) and one palatal (P). The two buccal canals are located on one line, from the midpoint of which a perpendicular line leads to the opening of the palatal canal. When the openings of the buccal canals are closely located, this form is often mistaken for a two-canal linear form, which can lead to the omission of the distal-buccal canal.
The first molars of the maxilla have a rectangular shape of the tooth cavity, which is wider in the mesiodistal direction than that of the second molars, represented by the anatomical navigational form "Mesial groove." The length of the mesial groove can be either short or long and may extend for 2/3 of the length of the floor in the vestibulopalatine direction. In the lumen of the mesial groove, there can be from one to three openings of the root canals, which are represented by wider sections of a single fissure. Therefore, when searching for root canals in this groove, it is advisable to conduct scouting (revision, development) deep into the groove with a thin ultrasonic or rotary instrument. Sometimes, due to deposits of replacement dentin, the mesial groove is covered by a dentin cap, which needs to be removed to improve access to the root canals. In cases where one opening was observed in the mesial groove, the tooth was classified as three-canal; if three openings of the mesial canals were observed, the total number of canals increased to five. Other variants of navigational-anatomical forms in the first molars were extremely rare. The linear form of the location of the openings of the root canals is observed in 4% of cases (10 cases had 4 canals, and 2 cases were two-canal), square anatomy — 1 tooth, T-shaped form — 1 tooth (table 2).
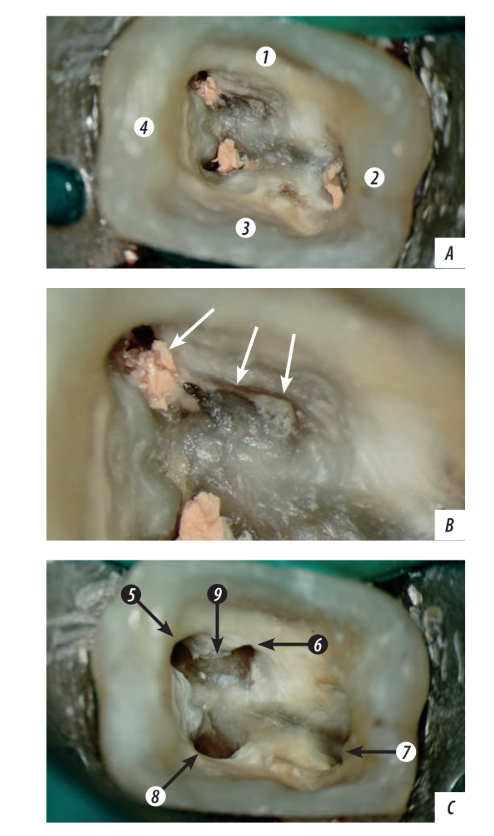
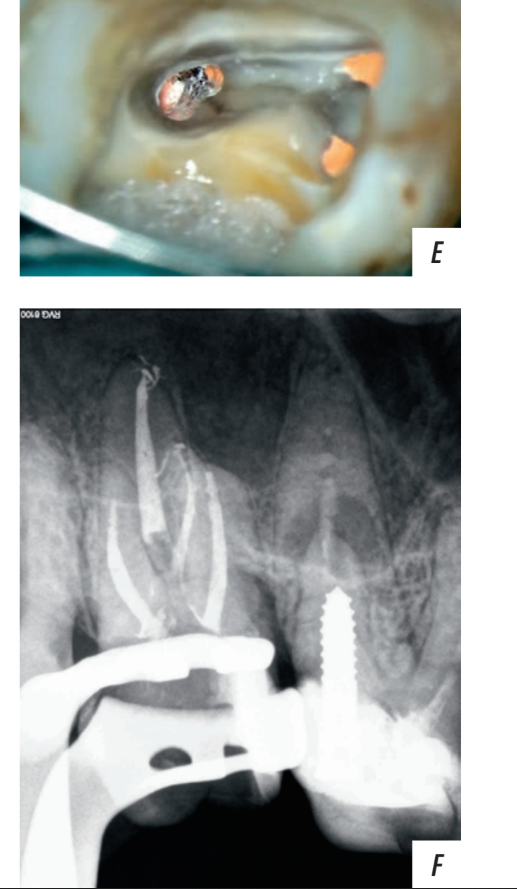
The second molars of the upper jaw have various anatomical forms. The cavity of these teeth has a narrower shape and is more elongated in the buccolingual direction, resembling a triangle with a long base located mesially. At the corners, vestibular and palatal, of this base are the orifices of the mesiobuccal and palatal canals. Observations have shown that the location of the orifices of the distobuccal and second mesiobuccal canals had the greatest variability. The orifice of the second mesiobuccal canal was most often located on the line between the mesiobuccal and palatal canals. The mesial groove in the second molars, unlike in the first molars, has a shorter length, often no more than 1/4 of the distance from the orifice of the mesial canal to the palatal one. In the second molars of the upper jaw, as in the first molars, there are from one (3-canal tooth) to three orifices of root canals within the mesial groove in a tooth with 5 canals. The orifice of the second mesiobuccal canal can significantly shift towards the palatal canal, sometimes located in the palatal canal below its orifice (Fig. 7). A total of 4 such clinical cases have been noted. The location of the orifice of the distobuccal canal in the second molars of the upper jaw is more variable than in the first upper molars, often shifting towards the mesiopalatal line at different angles of PDM. Probably for this reason, a linear shape with a PDM angle of more than 140° is more often found in the second upper molar (Table 3).
It should be noted that individual anatomical variations were observed in the upper jaw molars, which may have a combination of several anatomical variants simultaneously, for example, the first upper molar with six root canal orifices, the arrangement of which resembles a T-shaped navigation form, while the orifices of the MB2, and DB2 and DB3 canals are arranged as in "linear anatomy" (Fig. 8).
Conclusion
Knowledge of the rules for the location of root canal orifices and analysis of the shape of their arrangement, based on a navigational-optical approach, will allow practicing specialists to determine the maximum number of root canal orifices in upper molars, followed by the development of canal pathways for obturation, preventing complications in the periapical tissues in the long term after endodontic treatment.
References:
- Duncan H.F., Nagendrababu V., El-Karim I.A., Dummer P.M.H. Outcome measures to assess the effectiveness of endodontic treatment for pulpitis and apical periodontitis for use in the development of European Society of Endodontology (ESE) S3 level clinical practice guidelines: a protocol. — Int Endod J. — 2021; 54 (5): 646—654. PMID: 33630330
- Setzer F., Chogle S., Torabinedjad M. Endodontic treatment outcomes. — In: Torabinejad M., Fouad A.F., Shabahang S. Endodontics. Principles and practice. — Elsevier, 2021. — Pp. 453—455.
- Abbott P.V. Pulp, root canal, and periradicular conditions. — In: Ahmed H.M.A., Dummer P.M.H. Endodontic advances and evidence‐based clinical guidelines. — Hoboken, NJ: John Wiley & Sons, 2022. — Pp. 85-86, 93. DOI: 10.1002/9781119553939.ch4
- Restrepo-Restrepo F.A., Cañas-Jiménez S.J., Romero-Albar- racín R.D., Villa-Machado P.A., Pérez-Cano M.I., Tobón-Arroyave S.I. Prognosis of root canal treatment in teeth with preoperative apical periodontitis: a study with cone-beam computed tomography and digital periapical radiography. — Int Endod J. — 2019; 52 (11): 1533—1546. PMID: 31211862
- Ng Y.L., Mann V., Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. — Int Endod J. — 2011; 44 (7): 583—609. PMID: 21366626
- Baruwa A.O., Martins J.N.R., Meirinhos J., Pereira B., Gouveia J., Quaresma S.A., Monroe A., Ginjeira A. The Influence of missed canals on the prevalence of periapical lesions in endodontically treated teeth: a cross-sectional study. — J Endod. — 2020; 46 (1): 34—39.e1. PMID: 31733814
- Costa F.F.N.P., Pacheco-Yanes J., Siqueira J.F. Jr, Oliveira A.C.S., Gazzaneo I., Amorim C.A., Santos P.H.B., Alves F.R.F. Association between missed canals and apical periodontitis. — Int Endod J. — 2019; 52 (4): 400—406. PMID: 30284719
- Meirinhos J., Martins J.N.R., Pereira B., Baruwa A., Gouveia J., Quaresma S.A., Monroe A., Ginjeira A. Prevalence of apical periodontitis and its association with previous root canal treatment, root canal filling length and type of coronal restoration — a cross-sectional study. — Int Endod J. — 2020; 53 (4): 573—584. PMID: 31749154
- Alnowailaty Y., Alghamdi F. Prevalence of endodontically treated premolars and molars with untreated canals and their association with apical periodontitis using cone-beam computed tomography. — Cureus. — 2022; 14 (6): e25619. PMID: 35795507
- Karabucak B., Bunes A., Chehoud C., Kohli M.R., Setzer F. Prevalence of apical periodontitis in endodontically treated premolars and molars with untreated canal: a cone-beam computed tomography study. — J Endod. — 2016; 42 (4): 538—41. PMID: 26873567
- Martins J.N.R., Marques D., Silva E.J.N.L., Caramês J., Mata A., Versiani M.A. Second mesiobuccal root canal in maxillary molars- A systematic review and meta-analysis of prevalence studies using cone beam computed tomography. — Arch Oral Biol. — 2020; 113: 104589. PMID: 31735252
- Razumova S.N., Brago A.S., Barakat Kh.B., Khaskhanova L.M., Huaizi A., Nadtochiy A.G. Features of the anatomy of the first upper molars according to cone beam computed tomography data among residents of the Moscow region. — Medical alphabet. — 2018; 2 (339): 27—28 [Razumova S.N., Brago A.S., Barakat Kh.B., Khaskhanova L.M., Huaizi A., Nadtochiy A.G. Anatomy of first upper molar according to cone beam computed tomography among residents of Moscow Region. — Medical alphabet. — 2018; 2 (339): 27—28 (In Russian)]. eLibrary ID: 35040301
- Cantatore G., Berutti E., Castellucci A. Missed anatomy: frequency and clinical impact. — In: Endodontic Topics, vol. 15, issue 1. — Wiley & Sons, 2009. — Pp. 3—31. DOI: 10.1111/j.1601-1546.2009.00240.x
- Alyamovsky V.V., Levenets O.A., Levenets A.A., Narykova S.A. Morphological basis and methodical approaches to treatment of root canals maxillary molars. — Siberian Medical Review. — 2013; 6 (84): 3—8 [Alyamovsky V.V., Levenets O.A., Levenets A.A., Narykova S.A. Morphological basis and methodical approaches to treatment of root canals maxillary molars. — Siberian Medical Review. — 2013; 6 (84): 3—8 (In Russian)]. eLibrary ID: 21082580
- Alyamovsky V.V., Levenets O.A., Levenets A.A. Multiple anatomical variations of structure molars maxilla. — Endodontics Today. — 2014; 4: 22—25 [Alyamovsky V.V., Levenets O.A., Levenets A.A. Multiple anatomical variations of structure molars maxilla. — Endodontics Today. — 2014; 4: 22—25 (In Russian)]. eLibrary ID: 22842164
- Versiani M., Gleghorn B., Christie W. Root canal anatomy. — In: Torabinejad M., Fouad A.F., Shabahang S. Endodontics. Principles and practice. — Elsevier, 2021. — Pp. 225—230.
- Gopikrishna V. Grosman’s enododontic practice, 14th ed. — New Delhi: Wolters Kluwer, 2021. — Pp. 242—244.
- Batukov N.M., Konstantinov A.A., Chibisova M.A. Possibilities of visualizing the tooth structure by means of cone-beam computer tomography and microscope in endodontic treatment. — The Dental Institute. — 2016; 3 (72): 38—41 [Batukov N.M., Konstantinov A.A., Chibisova M.A. Possibilities of visualizing the tooth structure by means of cone-beam computer tomography and microscope in endodontic treatment. — The Dental Institute. — 2016; 3 (72): 38—41 (In Russian)]. eLibrary ID: 26602927
- Patel S., Brown J., Pimentel T., Kelly R.D., Abella F., Durack C. Cone beam computed tomography in Endodontics — a review of the literature. — Int Endod J. — 2019; 52 (8): 1138—1152. PMID: 30868610
- Martins J.N.R., Kishen A., Marques D., Nogueira Leal Silva E.J., Caramês J., Mata A., Versiani M.A. Preferred reporting items for epidemiologic cross-sectional studies on root and root canal anatomy using cone-beam computed tomographic technology: a systematized assessment. — J Endod. — 2020; 46 (7): 915—935. PMID: 32387077
- Abella F., Kanagasingam S. Assessment of root canal anatomy. — In: Patel S., Harvey S., Shemesh H., Durack C. Cone beam computed tomography in endodontics. — Quintessence, 2016. — Pp. 134—135.
- Han X., Yang H., Li G., Yang L., Tian C., Wang Y. A study of the distobuccal root canal orifice of the maxillary second molars in Chinese individuals evaluated by cone-beam computed tomography. — J Appl Oral Sci. — 2012; 20 (5): 563—7. PMID: 23138744
- Batukov N.M., Berkhman M.V. Estimation of Endodontic Treatment Efficacy Using a Microscope. — The Dental Institute. — 2013; 4 (61): 82—83 [Batyukov N.M., Berkhman M.V. Estimation of Endodontic Treatment Efficacy Using a Microscope. — The Dental Institute. — 2013; 4 (61): 82—83 (In Russian)]. eLibrary ID: 22988429
- Zhukova E.S., Chuikova Y.A. Quality assessment of root canal obturation using a dental microscope. — Scientist (Russia). — 2021; 2 (16): 23 [Zhukova E.S., Chuikova Y.A. Quality assessment of root canal obturation using a dental microscope. — Scientist (Russia). — 2021; 2 (16): 23 (In Russian)]. eLibrary ID: 47378335
- Gopikrishna V. Grosman’s enododontic practice, 14th ed. — New Delhi: Wolters Kluwer, 2021. — P. 230.