
Micro-CT assessment of the shaping ability of four root canal instrumentation systems in oval-shaped canals
Abstract
Aim: To compare the shaping ability of four root canal instrumentation systems in oval-shaped canals using micro-computed tomographic analysis.
Methodology: Forty anatomically matched mandibular incisors were scanned and assigned to four groups (n = 10), according to the canal preparation protocol: BioRace, Reciproc, Self-Adjusting File (SAF) and TRUShape systems. After canal instrumentation, the specimens were rescanned, and the registered pre- and postoperative datasets were examined to evaluate the percentages of accumulated hard-tissue debris, untouched canal walls and dentine removed. Kruskal–Wallis and Mann–Whitney U-tests with Bonferroni correction were used to compare the variables in the groups (α = 5%).
Results: The preparation techniques did not affect the percentage of accumulated hard-tissue debris (P = 0.126). The percentage of untouched canal areas was significantly higher for BioRace (32.38%) compared to Reciproc (18.95%) and SAF (16.08%) systems (P < 0.05). Reciproc removed significantly more dentine (4.18%) than BioRace (2.21%) and SAF (2.56%) (P < 0.05). The TRUShape system had intermediate results for both untouched canal walls (19.20%) and dentine removed (3.77%), with no significant difference compared to BioRace, Reciproc and SAF systems.
Conclusions: The preparation techniques resulted in the same level of accumulated hard-tissue debris. Compared to the other tested systems, BioRace was associated with more untouched canal walls and Reciproc produced the greatest amount of removed dentine. Although it touched more of the root canal walls, the SAF system removed less dentine, whereas TRUShape had intermediate results for these same parameters. None of the systems tested were able to provide optimal shaping ability in oval-shaped canals.
Introduction
The development of a new generation of nickel–titanium (NiTi) systems for canal preparation relies on changes in instrument design, alloy and kinematics, aiming to optimize the mechanical instrumentation of root canals (Peters 2004, Hu€lsmann et al. 2005). Most of the available rotary and reciprocating systems have failed to improve debridement of oval-shaped canals (Versiani et al. 2013), leaving large areas of untouched canal walls (Peters et al. 2001, Versiani et al. 2013, De-Deus et al. 2015a) and accumulated hard-tissue debris in fins, isthmuses and irregularities within the root canal space (Paqu´e et al. 2009, De-Deus et al. 2015b, Versiani et al. 2016). Bacteria located in these areas have the potential to remain and might be responsible for persistent periapical inflammation (Versiani et al. 2016).
Recently, a novel heat-treated NiTi rotary system, the TRUShape 3D Conforming Files system (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA), was introduced. It is advertised by the manufacturer as a set of instruments that enable greater dentinal preservation than conventional files, whilst making contact with nearly 75% of the canal walls (TRUShape® 3D Conforming Files. Dentsply Tulsa Dental Specialties website) due to the triangular crosssection, a noncutting tip, and a sweeping S-shape along its long axis, resulting in a .06 taper in the apical 2 mm and an increasing variable taper from this level denoted as a .06v taper. A recent study showed that root canal preparation with TRUShape instruments removed significantly more bacteria from oval-shaped root canals than the Twisted File rotary system (SybronEndo, Orange, CA, USA) (Bortoluzzi et al. 2015); however, no study has attempted to challenge the shaping ability of this novel system regarding the accumulation of hard-tissue debris, untouched root canal walls and the amount of dentine removed from oval-shaped root canals compared to other preparation systems.
Therefore, the aim of this study was to compare the percentages of accumulated hard-tissue debris, untouched canal areas and dentine removed after root canal preparation with BioRace (FKG Dentaire, La-Chaux-de-Fonds, Switzerland), Reciproc (VDW, Munich, Germany), Self-Adjusting File (SAF; ReDent- Nova, Ra’anana, Israel) and TRUShape systems through micro-computed tomographic (micro-CT) analysis. The null hypothesis tested was that there would be no significant difference in shaping outcomes amongst these four preparation systems.
Materials and methods
Sample size estimation
Based on the results of a previous study (De-Deus et al. 2015b), an effect size of 0.9 was estimated and input, together with the parameter alpha-type error of 0.05 and power beta of 0.95, into a one-way ANOVA procedure (G*Power 3.1 for Macintosh; Heinrich Heine, Universität Düsseldorf, Düsseldorf, Germany). A sample size of 28 teeth (seven per group) was indicated as the minimum to reveal statistical significance amongst groups.
Sample selection and preparation
After local research ethics committee approval, 127 human mandibular incisors were obtained from a pool of teeth. Each tooth was radiographed in both buccolingual and mesiodistal directions. To prevent the introduction of confounding variables, the inclusion criteria were only teeth with approximately 19 1 mm in length, straight roots (<5°) (Schneider 1971), a canal ratio of long to short diameter more than 2.5 at the 5 mm level from the root apex and an initial apical size equivalent to a size 10 K-file (Dentsply Sirona, Ballaigues, Switzerland). As a result, 63 teeth were selected and scanned in a micro-CT device (SkyScan 1173; Bruker micro-CT, Kontich, Belgium) operated at 70 kV and 114 mA, using a low resolution (70 μm) to obtain an outline of the root canals. The acquired projection images were reconstructed (NRecon v.1.6.10; Bruker micro-CT) providing axial crosssections of their inner structure, and 40 mandibular incisors with similar canal configuration were selected and scanned again at an increased resolution (14.25 μm) with 360° rotation around the vertical axis, a rotation step of 0.5°, a camera exposure time of 7000 ms and frame averaging of 5, using a 1.0 mm-thick aluminium filter. Images of each specimen were reconstructed using standardized parameters for beam hardening (40%), ring artefact correction (10) and similar contrast limits. The volume of interest was selected to extend from the cemento-enamel junction to the apex of the root, resulting in the acquisition of 800–900 transverse crosssections per tooth. The apices of the teeth were then sealed with hot glue and embedded in polyvinyl siloxane to create a closed-end system (Susin et al. 2010).
After access cavity preparation, a glide path was created by scouting a stainless steel size 20 K-file (Dentsply Sirona) up to the working length (WL), which was established by deducting 1 mm from the canal length. Canals were then matched to create ten groups of four teeth based on similar morphological features of the canal (length, volume, surface area, structure model index [SMI] and configuration), and one root from each group was randomly assigned to one of the four experimental groups (n = 10) according to the preparation protocol.
BioRace system
BR0 (25/.08), BR1 (15/.05), BR2 (25/.04) and BR3
(25/.06) NiTi rotary instruments were used at 500– 600 rpm and 1 N cm in a crown-down manner (VDW Silver motor; VDW) up to the WL, using a gentle in-and-out pecking motion. After three steady strokes, the file was removed from the canal and cleaned.
Reciproc system
A R25 instrument (25/.08) was moved in the apical direction using a slow in-and-out pecking motion of about 3 mm in amplitude with a light apical pressure in a reciprocating motion (‘RECIPROC ALL’) powered by an electric motor (VDW Silver) until the WL was reached. After three pecking motions, the instrument was removed from the canal and cleaned. The WL was reached in the third wave of instrumentation for all teeth.
SAF system
A 1.5-mm diameter SAF instrument was operated to the WL with an in-and-out motion using an RDT3 head (ReDent-Nova) adapted to a vibrating handpiece (GentlePower Lux 20LP; KaVo, Biberach, Germany). Continuous irrigation with 5.25% NaOCl was applied throughout the procedure at a flow rate of 5 mL min—1 using a special irrigation apparatus (VATEA; ReDent-Nova).
TRUShape system
Using an electric motor (VDW Silver) pre-set at 300 rpm and 3 N cm, a TRUShape 20/.08v file was used with a gentle 2–5 mm in-and-out motion to shape the middle third. TRUShape 20/.06v and 25/.06v instruments were then used with a further 2– 3 mm amplitude towards the WL. Each tooth was shaped as two canals due to its larger buccal-lingual dimension, as recommended by the manufacturer.
In all groups, the total preparation time was 4 min. Irrigation was performed with a NaviTip needle (Ultradent Products Inc., South Jordan, UT, USA) using 20 mL of 5.25% NaOCl per tooth. In all groups, at the end of the preparation, passive ultrasonic irrigation was performed for 20 s at 2 mm short of the WL using a size 15 K-file (Dentsply Sirona), and canals were then flushed with 3 mL of 17% EDTA for 5 min and 2 mL of bi-distilled water for 1 min. Therefore, each tooth was irrigated with 25 mL of irrigant over 10 min. Aspiration of the irrigant solution was performed at the canal orifice with a Surgi-Tip (Ultradent Products Inc.) attached to a high-speed suction pump. An experienced operator conducted all preparation procedures after substantial training with all systems. Root canals were dried with absorbent paper points (Dentsply Sirona) and the specimens submitted to a postoperative scan and reconstruction, applying the aforementioned parameters.
Micro-CT evaluation
The image stacks of the specimens after preparation were rendered and co-registered with their respective preoperative datasets using an affine algorithm of the 3D Slicer 4.5.0 software (available from http://www.slicer.org) (Fedorov et al. 2012). The quantification of accumulated hard-tissue debris was expressed as the percentage of the total canal system volume after preparation for each specimen and undertaken as described elsewhere (De-Deus et al. 2014, 2015b, Neves et al. 2015). The volume of the dentine removed after preparation was calculated by subtracting pre- and postoperative segmented root dentine using morphological operations (Fiji v.1.47n; Madison, WI, USA). The area of untouched canal surface was determined by calculating the number of static voxels (voxels present in the same position on the canal surface before and after instrumentation). The untouched area was expressed as a percentage of the total number of voxels present on the canal surface (Paqué & Peters 2011), according to the formula:
(number of static voxels × 100)/ total number of surface voxels
Statistical analysis
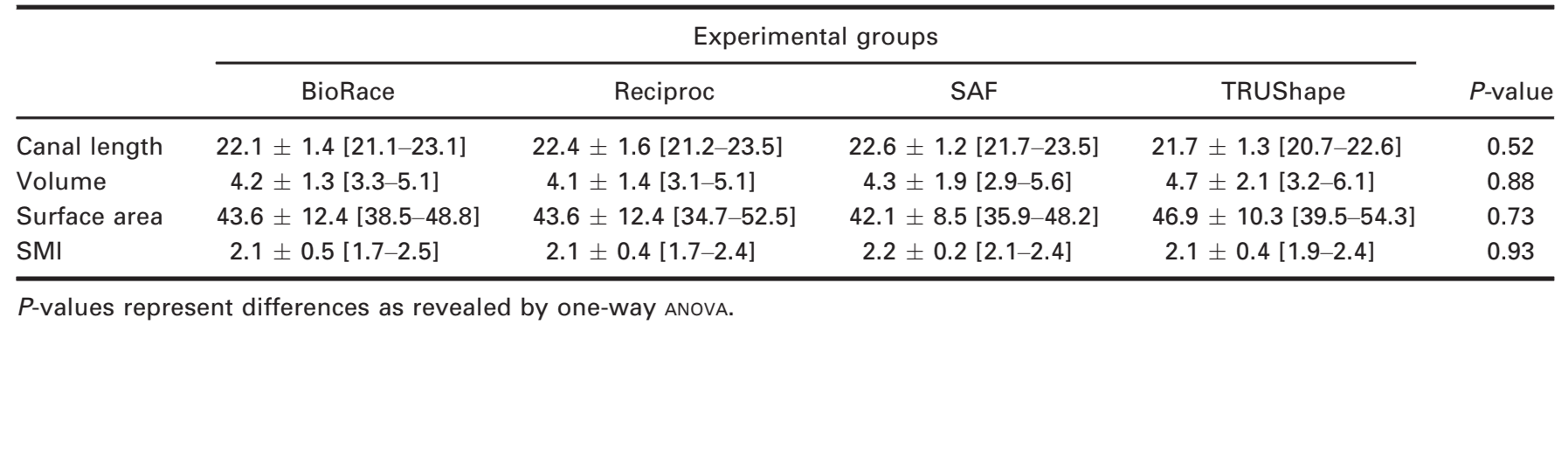
The degree of homogeneity (baseline) of the groups, before root canal preparation, was verified by performing a one-way ANOVA comparison amongst the groups regarding the root canal volume (mm3), unprepared surface area (mm2), length and SMI. SMI involves a measurement of surface convex curvature. In endodontics, the SMI parameter is intended to determine quantitatively the three-dimensional geometry of the root canal. Because normality assumptions of the percentages of accumulated hard-tissue debris, untouched canal area and dentine removed after root canal preparation could not be verified (Shapiro–Wilk test; P < 0.05), the results were expressed as medians and compared between groups by Kruskal–Wallis and Mann–Whitney U-tests with Bonferroni correction (SPSS v.17; SPSS Inc., Chicago, IL, USA). Significance was set at α = 5%.
Results
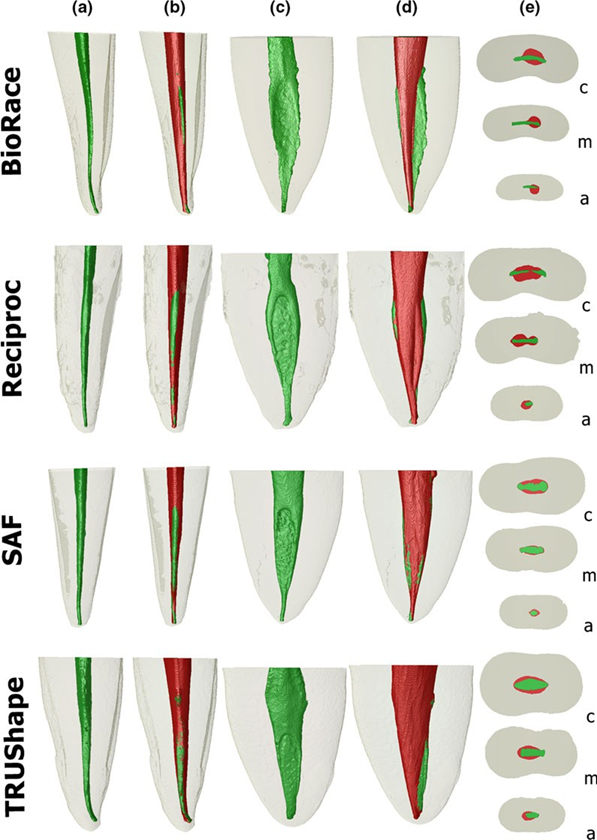
Figure 1 shows representative images of the internal anatomy of four mandibular incisors before and after canal preparation with the systems tested.
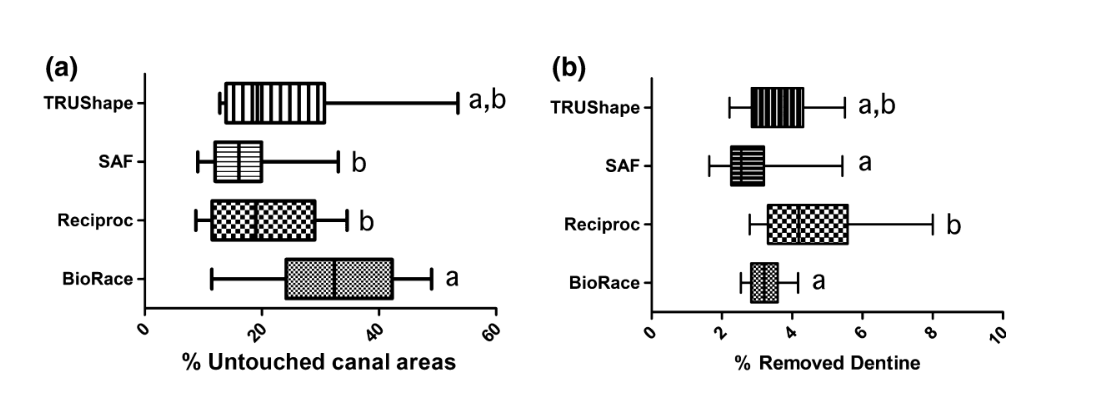
The degree of homogeneity (baseline) of the groups regarding initial canal volume, surface area, length and SMI before and after root canal preparation was confirmed (Table 1, P > 0.05). There was no significant difference in the median and interquartile ranges (IQR) regarding the percentage of accumulated hard-tissue debris amongst TRUShape (0.00%, IQR 0.06), BioRace (0.00%, IQR 0.00), Reciproc (0.01%, IQR 0.22) or SAF (0.00%, IQR 0.00) groups (P > 0.05). A significantly greater percentage of untouched canal area was observed after preparation with the BioRace system (32.38%, IQR 18.10) compared to the Reciproc (18.95%, IQR 17.50) and SAF (16.08%, IQR 7.94) systems (P < 0.05). Reciproc removed significantly more dentine (4.18%, IQR 2.27) than BioRace (2.21%, IQR 0.76) and SAF (2.56%, IQR 0.92) (P < 0.05). The TRUShape system had intermediate results regarding the untouched canal area (19.20%, IQR 16.80) and the amount of dentine removed (3.77%, IQR 1.46) with no significant difference compared to the other systems (P > 0.05) (Fig. 1). Figure 2 shows a boxplot representation of the median percentages and IQR of the parameters tested (untouched canal areas [a] and removed dentine [b]) after root canal preparation with the BioRace, Reciproc, SAF and TRUShape systems.
Discussion
The current investigation was designed to evaluate the percentages of accumulated hard-tissue debris, untouched canal walls and dentine removed after preparation of oval-shaped canals of mandibular incisors with BioRace, Reciproc, SAF and TRUShape systems using micro-CT analysis. Despite natural variations in the morphology of teeth, attempts were made to ensure comparability of the groups regarding root canal morphology. As oval-shaped canals present a challenge to the clinician (Peters 2004, De-Deus et al. 2010, Versiani et al. 2011), this type of canal configuration was selected. As previous studies (Peters et al. 2001, Versiani et al. 2016), a micro-CT screening of the volume, surface area, length and SMI was performed to provide an overall anatomical mapping of the root canals. Based on these measurements, four similar teeth were grouped and further allocated in one of the four groups. Statistical analysis confirmed the effective balance between the groups with respect to the baseline parameters, thus enhancing the internal validity of the study and potentially eliminating significant anatomical biases that may confound the outcomes.
In the last decade, three-dimensional nondestructive imaging micro-CT technology has been used successfully for quantitative evaluation of hard-tissue debris packed into root canal recesses during preparation procedures (Paqué et al. 2009, 2011, 2012, Robinson et al. 2013, De-Deus et al. 2014, 2015b, Neves et al. 2015, Versiani et al. 2016). Evidences from these studies indicate that dentine particles cut from the canal walls by endodontic instruments can be actively packed into the anatomical complexities of the canal system, becoming more resistant to removal. In the present study, accumulation of hard-tissue debris occurred regardless of system design and kinematics, which is in accordance with De-Deus et al. (2015b). On the other hand, the present findings disagree with other micro-CT studies, in which preparation with the SAF system resulted in less debris accumulation (Paqué et al. 2012), and with a reciprocating system that left significantly more debris within the root canals than a multifile rotary system (Robinson et al. 2013). These contradictory results may be explained by differences in the methodological design. The oval-shaped canals of mandibular incisors were used here, and in those studies (Paqué et al. 2012, Robinson et al. 2013), a more complex preoperative canal configuration (mesial root canal system of mandibular molars) was used. Passive ultrasonic irrigation was also used as a supplementary irrigation protocol in the present study. According to a recent study, the activation of the irrigant solution with an oscillating ultrasonic tip after root canal preparation is more likely to remove hard-tissue debris from root canals with a simple anatomy (Versiani et al. 2016), which may also help to explain the present results.
It is well established that untouched canal walls may be colonized by biofilms and serve as a potential cause of persistent infection, which may compromise the treatment outcome (Alves et al. 2011, Dietrich et al. 2012). In the current study, the percentage of untouched canal walls and dentine removed were significantly affected by the preparation protocols. Consequently, the null hypothesis tested was rejected. The median percentage of untouched canal walls ranged from 16.08% to 32.38%, and none of the tested systems were able to completely debride the dentinal walls, which is in agreement with previous reports (Peters et al. 2001, Paqué & Peters 2011, Versiani et al. 2013, Bortoluzzi et al. 2015, De-Deus et al. 2015a). Amongst the tested systems, the SAF and Reciproc systems had the lowest percentage of untouched canal area. As previously demonstrated (Metzger et al. 2010a, Paqué & Peters 2011, Versiani et al. 2011, 2013), results from the SAF system can be explained because of its hollow NiTi lattice-like form, which adapts itself to the shape of the root canal, enabling a greater percentage of root canal walls to be touched. Besides, the back-and-forth grinding motion of the SAF instrument enables the circumferential removal of only a thin layer of dentine from most of the canal walls (Metzger et al. 2010b), which explains the lowest percentage of dentine removed by the SAF system in this study. On the other hand, the low percentage of untouched canal walls and larger amount of removed dentine observed after canal preparation with the Reciproc system may be explained by the combination of its reciprocating kinematics, larger taper size (.08 in the first 3 mm) and design (sharp cutting edges and smaller cross-sectional area), which effect its flexibility and increase its cutting efficiency in a brushing motion (Plotino et al. 2014). Similarly, the smaller dimensions and cutting efficiency of BioRace instruments compared to Reciproc explain its greater percentage of untouched canal walls and less dentine removal (Lopes et al. 2010).
Root canal preparation with the TRUShape system was associated with intermediate median results regarding untouched canal walls and dentine removed. Peters et al. (2015) reported that TRUShape enables dentine preservation during root canal shaping, and Elnaghy et al. (2017) reported a mean percentage of dentine removed of about 2.77%, which is similar to the 3.77% observed herein. However, in the present study, dentine preservation by TRUShape could not be confirmed. The asymmetric cutting motion of the TRUShape files, which can reach a fluted diameter up to 0.80 mm, might be the basis to explain the lack of significance compared to the other tested systems evaluated here (Fig. 2).
One may argue that the differences in the rotation speed (rpm) alone, used to activate the tested instruments, might influence the results. If this were true, BioRace should have had a lower percentage of untouched canal area and a greater amount of dentine removal when compared to TRUShape files, as the former was used in a higher number of revolutions to shape the root canal when compared to the latter (500–600 rpm and 300 rpm, respectively). Similarly, instruments with different kinematics were also used in the current study (continuous rotation, reciprocating and in-and-out movement). Moreover, it is important to emphasize that all instruments were used according to the specific manufacturer0s instructions. Therefore, shaping outcomes must be considered a result of an interplay amongst different variables such as instrument design, activation kinematics, operator experience, speed and torque used during root canal shaping, amongst others.
Like other studies using the nondestructive micro-CT approach (Peters et al. 2001, Paqué et al. 2012, De-Deus et al. 2015a,b, Versiani et al. 2016), the current results highlight the less than ideal ability of currently available preparation systems to prepare this type of root canal configuration. These findings emphasize the importance of irrigation and intracanal dressing procedures in an attempt to compensate for the suboptimal status of the mechanical preparation (Versiani et al. 2011, 2013, Siqueira et al. 2013).
Conclusions
Under the conditions of the present study, none of the tested systems were able to provide optimal shaping of oval-shaped canals. Root canal preparation with the BioRace, Reciproc, SAF and TRUShape systems resulted in similar amounts of accumulated hard-tissue debris. Greater percentage of untouched canal areas and dentine removal were observed after preparation with BioRace and Reciproc systems, respectively. The SAF system touched more root canal walls and removed less dentine, whilst TRUShape had intermediate results for these same parameters.
Authors: M. L. Zuolo1, A. A. Zaia, F. G. Belladonna, E. J. N. L. Silva, E. M. Souza, M. A. Versiani, R. T. Lopes, G. De-Deus
References
- Alves FR, Almeida BM, Neves MA, Moreno JO, Rôças IN, Siqueira JF Jr (2011) Disinfecting oval-shaped root canals: effectiveness of different supplementary approaches. Journal of Endodontics 37, 496–501.
- Bortoluzzi EA, Carlon D Jr, Meghil MM et al. (2015) Efficacy of 3D conforming nickel titanium rotary instruments in eliminating canal wall bacteria from oval-shaped root canals. Journal of Dentistry 43, 597–604.
- De-Deus G, Barino B, Zamolyi RQ et al. (2010) Suboptimal debridement quality produced by the single-file F2 ProTaper technique in oval-shaped canals. Journal of Endodontics 36, 1897–900.
- De-Deus G, Marins J, Neves Ade A et al. (2014) Assessing accumulated hard-tissue debris using micro-computed tomography and free software for image processing and analysis. Journal of Endodontics 40, 271–6.
- De-Deus G, Belladonna FG, Silva EJ et al. (2015a) Micro-CT evaluation of non-instrumented canal areas with different enlargements performed by NiTi systems. Brazilian Dental Journal 26, 624–9.
- De-Deus G, Marins J, Silva EJ et al. (2015b) Accumulated hard tissue debris produced during reciprocating and rotary nickel-titanium canal preparation. Journal of Endodontics 41, 676–81.
- Dietrich MA, Kirkpatrick TC, Yaccino JM (2012) In vitro canal and isthmus debris removal of the self-adjusting file, K3, and WaveOne files in the mesial root of human mandibular molars. Journal of Endodontics 38, 1140–4.
- Elnaghy AM, Al-Dharrab AA, Abbas HM, Elsaka SE (2017) Evaluation of root canal transportation, centering ratio, and remaining dentin thickness of TRUShape and ProTaper Next systems in curved root canals using micro-computed tomography. Quintessence International 48, 27–32.
- Fedorov A, Beichel R, Kalpathy-Cramer J et al. (2012) 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magnetic Resonance Imaging 30, 1323–41.
- Hülsmann M, Peters OA, Dummer PMH (2005) Mechanical preparation of root canals: shaping goals, techniques and means. Endodontic Topics 10, 30–76.
- Lopes HP, Elias CN, Vieira VT et al. (2010) Effects of electropolishing surface treatment on the cyclic fatigue resistance of BioRace nickel-titanium rotary instruments. Journal of Endodontics 36, 1653–7.
- Metzger Z, Zary R, Cohen R, Teperovich E, Paqué F (2010a) The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. Journal of Endodontics 36, 1569–73.
- Metzger Z, Teperovich E, Zary R, Cohen R, Hof R (2010b) The self-adjusting file (SAF). Part 1: respecting the root canal anatomy-a new concept of endodontic files and its implementation. Journal of Endodontics 36, 679–90.
- Neves AA, Silva EJ, Roter JM et al. (2015) Exploiting the potential of free software to evaluate root canal biomechanical preparation outcomes through micro-CT images. International Endodontic Journal 48, 1033–42.
- Paqué F, Peters OA (2011) Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the self-adjusting file. Journal of Endodontics 37, 517–21.
- Paqué F, Laib A, Gautschi H, Zehnder M (2009) Hard-tissue debris accumulation analysis by high-resolution computed tomography scans. Journal of Endodontics 35, 1044–7.
- Paqué F, Boessler C, Zehnder M (2011) Accumulated hard tissue debris levels in mesial roots of mandibular molars after sequential irrigation steps. International Endodontic Journal 44, 148–53.
- Paqué F, Al-Jadaa A, Kfir A (2012) Hard-tissue debris accumulation created by conventional rotary versus self-adjusting file instrumentation in mesial root canal systems of mandibular molars. International Endodontic Journal 45, 413–8.
- Peters OA (2004) Current challenges and concepts in the preparation of root canal systems: a review. Journal of Endodontics 30, 559–67.
- Peters OA, Schönenberger K, Laib A (2001) Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. International Endodontic Journal 34, 221–30.
- Peters OA, Arias A, Paqué F (2015) A micro-computed tomographic assessment of root canal preparation with a novel instrument, TRUShape, in mesial roots of mandibular molars. Journal of Endodontics 41, 1545–50.
- Plotino G, Giansiracusa Rubini A, Grande NM, Testarelli L, Gambarini G (2014) Cutting efficiency of Reciproc and WaveOne reciprocating instruments. Journal of Endodontics 40, 1228–30.
- Robinson JP, Lumley PJ, Cooper PR, Grover LM, Walmsley AD (2013) Reciprocating root canal technique induces greater debris accumulation than a continuous rotary technique as assessed by 3-dimensional micro-computed tomography. Journal of Endodontics 39, 1067–70.
- Schneider SW (1971) A comparison of canal preparations in straight and curved root canals. Oral Surgery, Oral Medicine, Oral Pathology and Endodontics 32, 271–5.
- Siqueira JF Jr, Alves FRF, Versiani MA et al. (2013) Correlative bacteriologic and micro-computed tomographic analysis of mandibular molar mesial canals prepared by self-adjusting file, reciproc and twisted file systems. Journal of Endodontics 39, 1044–50.
- Susin L, Liu Y, Yoon JC et al. (2010) Canal and isthmus debridement efficacies of two irrigant agitation techniques in a closed system. International Endodontic Journal 43, 1077–90.
- TRUShape® 3D Conforming Files. Dentsply Tulsa Dental Specialties website. Available at: https://www.dentsply.com/content/dam/dentsply/pim/manufacturer/Endodontics/GlidePath Shaping/Rotary Reciprocating_Files/3D Conforming/TRUShape 3D Conforming Files/TRUShape-3D-Conforming-Files-Brochure-2vkhexu-en-1504.pdf. Accessed June 17, 2017.
- Versiani MA, Pécora JD, de Sousa-Neto MD (2011) Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. Journal of Endodon- tics 37, 1002–7.
- Versiani MA, Leoni GB, Steier L et al. (2013) Micro-computed tomography study of oval-shaped canals prepared with the self-adjusting file, Reciproc, WaveOne, and ProTaper universal systems. Journal of Endodontics 39, 1060–6.
- Versiani MA, Alves FR, Andrade-Junior CV et al. (2016) Micro-CT evaluation of the efficacy of hard-tissue removal from the root canal and isthmus area by positive and negative pressure irrigation systems. International Endodontic Journal 49, 1079–87.