
Micro–computed Tomography Study of Oval-shaped Canals Prepared with the Self-adjusting File, Reciproc, WaveOne, and ProTaper Universal Systems
Abstract
Introduction: The newly developed single-file systems claimed to be able to prepare the root canal space with only 1 instrument. The present study was designed to test the null hypothesis that there is no significant difference in the preparation of oval-shaped root canals using single- or multiple-file systems.
Methods: Seventy-two single-rooted mandibular canines were matched based on similar morphologic dimensions of the root canal achieved in a micro–computed tomographic evaluation and assigned to 1 of 4 experimental groups (n = 18) according to the preparation technique (ie, Self-Adjusting File [ReDent-Nova, Ra’anana, Israel], WaveOne [Dentsply Maillefer, Ballaigues, Switzerland], Reciproc [VDW, Munich, Germany], and ProTaper Universal [Dentsply Maillefer] systems). Changes in the 2- and 3- dimensional geometric parameters were compared with preoperative values using analysis of variance and the post hoc Tukey test between groups and the paired sample t test within groups (α = 0.05).
Results: Preparation significantly increased the analyzed parameters; the outline of the canals was larger and showed a smooth taper in all groups. Untouched areas occurred mainly on the lingual side of the middle third of the canal. Overall, a comparison between groups revealed that SAF presented the lowest, whereas WaveOne and ProTaper Universal showed the highest mean increase in most of the analyzed parameters (P < .05).
Conclusions: All systems performed similarly in terms of the amount of touched dentin walls. Neither technique was capable of completely preparing the oval-shaped root canals. (J Endod 2013;39:1060–1066)
The development of nickel-titanium (NiTi) rotary file systems has resulted in a progress in the mechanical preparation of the root canal space. However, the current technology for mechanical preparation has failed in debriding oval-shaped canals, leaving untouched fins or recesses on the buccal and/or lingual extensions. These untouched recesses may harbor unaffected residual bacterial biofilms and serve as a potential cause of persistent infection and poor treatment outcome.
The Self-Adjusting File (SAF; ReDent-Nova, Ra’anana, Israel), a hollow file composed of 120-mm-thick NiTi lattice, was introduced with a concept of a single instrument to prepare the entire root canal. During operation, the SAF adapts itself 3 dimensionally to the irregular shape of the root canal and, rather than machining its central portion into a round cross-section, it maintains the original canal shape with slightly larger dimensions. Previous studies have shown that the SAF system was particularly advantageous in promoting cleaning, shaping, and disinfection of oval-shaped canals compared with rotary files. The newly developed reciprocating instruments Reciproc (VDW, Munich, Germany) and WaveOne (Dentsply Maillefer, Ballaigues, Switzerland) are made of a special NiTi alloy (M-Wire) and are also claimed to be able to mechanically prepare the root canal space with only 1 instrument. These files are available in 3 different sizes, which are indicated to be used according to the canal diameter. Initial reports using these instruments in extracted teeth have shown that they can debride the root canal space similarly to conventional rotary systems.
Several methodologies were developed to evaluate the shaping ability of NiTi systems. These methodologies have been successfully used for many years; however, some inherent repeatedly discussed limitations have encouraged the search for new methods that are able to produce improved results. The development of X-ray micro–computed tomography (μCT) has gained increasing significance in the study of dental tissues because it offers a noninvasive technique for 3-dimensional (3D) assessment of the root canal system.
Even though there is accumulating evidence of the safety and shaping effectiveness of the Reciproc R25 and WaveOne Primary (25.08), knowledge of the shaping ability of Reciproc R40 and WaveOne Large (40.08) is still lacking. Therefore, the purpose of this study was to compare single- and multiple-file systems by testing the null hypothesis that there is no difference between them in the preparation of oval-shaped root canals using 3D μCT analysis.
Materials and Methods
Teeth Selection
After ethics committee approval, 100 straight single-rooted human mandibular canine teeth with fully formed apices and a single root canal were randomly selected from a pool of extracted teeth, decoronated slightly above the cementoenamel junction, and stored in labeled individual plastic vials containing 0.1% thymol solution. Each root was radiographed both in buccolingual and mesiodistal projections, and the canal diameter measured 5 mm from the apex. When the buccolingual diameter was 2.5 or more times larger than that of the mesiodistal diameter, the canals were classified as oval shaped.
After being washed in running water, each tooth was dried, mounted on a custom attachment, and scanned in a μCT scanner (SkyScan 1174v2; Bruker-microCT, Kontich, Belgium) operated at 50 kV and 800 μA (0.5-mm Al filter). The scanning was performed by 180° rotation around the vertical axis with a rotation step of 1°. The cross-sectional pixel size and intersection distance were 19.6 μm. Images of each specimen were reconstructed (NRecon v.1.6.3, Bruker-microCT) providing axial cross-sections of their inner structure. For each tooth, evaluation was performed for the full canal length in approximately 600–800 slices per specimen. CTAn v.1.12 software (Bruker-microCT) was used for the 2-dimensional (2D) (area, perimeter, roundness, major diameter, and minor diameter) and 3D (volume, surface area, and structure model index) evaluation of the root canal. The structure model index (SMI) involves a measurement of surface convexity in a 3D structure. An ideal plate, cylinder, and sphere have SMI values of 0, 3, and 4, respectively. CTVol v.2.2.1 software (Bruker-microCT) was used for visualization and qualitative evaluation of the specimens.
Each root canal was negotiated with a #10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) and the coronal third flared with a #2 LA Axxess Stainless Steel bur (SybronEndo, Orange, CA) using circumferential motion followed by irrigation with 5 mL 2.5% NaOCl. Subsequently, apical patency was determined by inserting a size 10 K-file into the root canal until its tip was visible at the apical foramen, and the working length (WL) was set 1.0 mm shorter of this measurement. Size 15 and 20 hand files were used at the WL to create a #20/.02 glide path.
From the initial sampling (N = 100), 72 teeth were matched to create 18 foursomes based on the morphologic dimensions of the root canal assessed in the initial μCT evaluation. One tooth from each foursome was randomly assigned to 1 of 4 experimental groups (n = 18). After the groups were established, a flip of a coin was used to define which group of teeth would be treated with each of the following root canal preparation techniques: SAF, WaveOne, Reciproc, or ProTaper Universal systems. After checking the normality assumption (Shapiro-Wilk test), the degree of homogeneity (baseline) of the 4 groups with respect to the previously mentioned parameters of the root canal was assessed using 1-way analysis of variance with a confidence interval of 95%.
Root Canal Preparation
A 1.5-mm diameter SAF instrument was inserted into the root canal and operated to the WL with an in-and-out motion using a vibrating handpiece (GentlePower Lux 20LP; KaVo, Biberach, Germany) combined with a RDT3 head (ReDent-Nova). Continuous irrigation with 2.5% NaOCl was applied throughout the procedure at a flow rate of 5 mL/min using a special irrigation apparatus (VATEA, ReDent-Nova). WaveOne Large (40.08) and Reciproc R40 (40.06) instruments were introduced into the canal until resistance was felt and then activated in reciprocating motion generated by a 6:1 contra-angle handpiece (Sirona, Bensheim, Germany) powered by an electric motor (VDW Silver; VDW GmbH, Munich, Germany). The instruments were moved in the apical direction using an in-and-out pecking motion of about 3 mm in amplitude with a light apical pressure. After 3 pecking motions, the instruments were removed from the canal and cleaned. ProTaper Universal instruments were used in continuous clockwise rotation (VDW Silver) using a gentle in-and-out motion in a modified crown-down manner. SX was used at two thirds of the WL, S1 and S2 at WL 1 mm; and then F1, F2, F3, and F4 at the WL. Each set of instruments was used to enlarge 2 canals only.
All preparations were performed by 1 operator (MAV) with clinical experience in all systems. In all groups, the total preparation time was 4 minutes and included only active instrumentation. Once each instrument had been negotiated to the end of the canal and had rotated freely, it was used in a light brushing motion. In the rotary and reciprocating groups, passive ultrasonic irrigation was performed every 15 seconds at the WL using a size #15 K file with a total of 20 mL 2.5% NaOCl. At the end of preparation, the canals were flushed with 2 mL 17% EDTA for 5 minutes and 2 mL distilled water for 1 minute; the canals were dried with paper points; and the roots were submitted to a postoperative μCT scan and reconstruction, applying the initial parameter settings.
Evaluation of the Root Canal Preparation
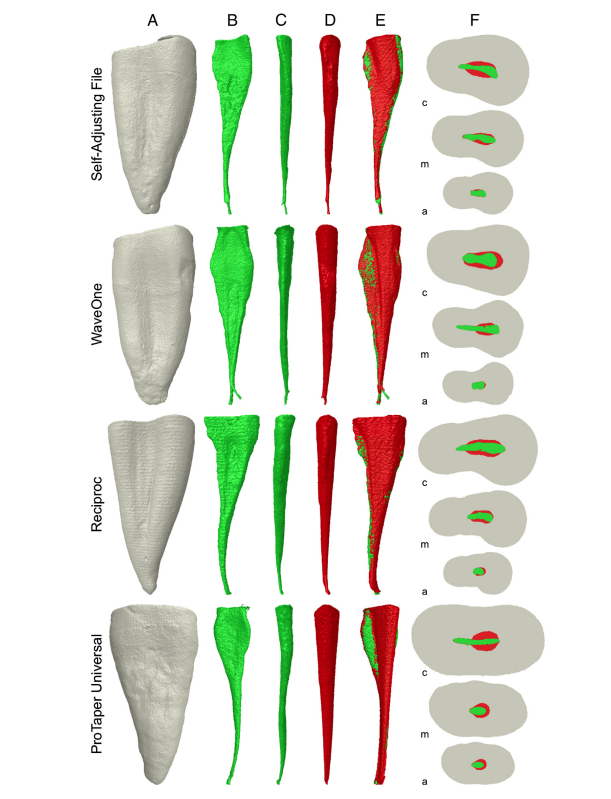
3D root canal models were reconstructed on the basis of μCT scans, and the superimposition of pre- and postpreparation images was ensured by means of a previously validated registration software (Mosaic 0.05; Institute of Communication and Computer Systems, Athens, Greece). Color-coded root canal models (green indicates preoperative and red indicates postoperative canal surfaces) enabled qualitative comparison of the matched root canals before and after shaping using CTVol v.2.2.1 software (Bruker-microCT). CTAn v.1.12 (Bruker-microCT) was used for measuring the area, perimeter, roundness, major diameter, minor diameter, volume, surface area, and SMI. The mean increase (D) of each analyzed parameter was calculated by subtracting the scores for the treated canals from those recorded for the untreated counterparts. 2D evaluations were performed for the full canal length in a total of 14,142 (SAF), 14,145 (WaveOne), 14,295 (Reciproc), and 14,325 (ProTaper Universal) cross-sections.
Statistical Analysis
Because normality assumptions could be verified (Shapiro-Wilk test), the mean increase (D) of each parameter was compared by using 1-way analysis of variance with the post hoc Tukey test between groups and the paired sample t test within groups using SPSS v17.0 for Windows (SPSS Inc, Chicago, IL) with the level of statistical significance set at 5%.
Results
Preoperatively (Fig. 1A), canal cross-sections presented significantly flatter and irregularly tapered by both mesiodistal and buccolingual views (Fig. 1B and C). After preparation, the outline of the canals was larger and showed a smooth taper in all experimental groups (Fig. 1D). Changes in the canal shape, shown as superimpositions of unprepared (green) and prepared (red) areas, showed untouched areas mainly on the lingual side of the middle third (Fig. 1E). The SAF resulted in a more uniform dentin removal along the perimeter of the canals than reciprocating or rotary instrumentation (Fig. 1F).
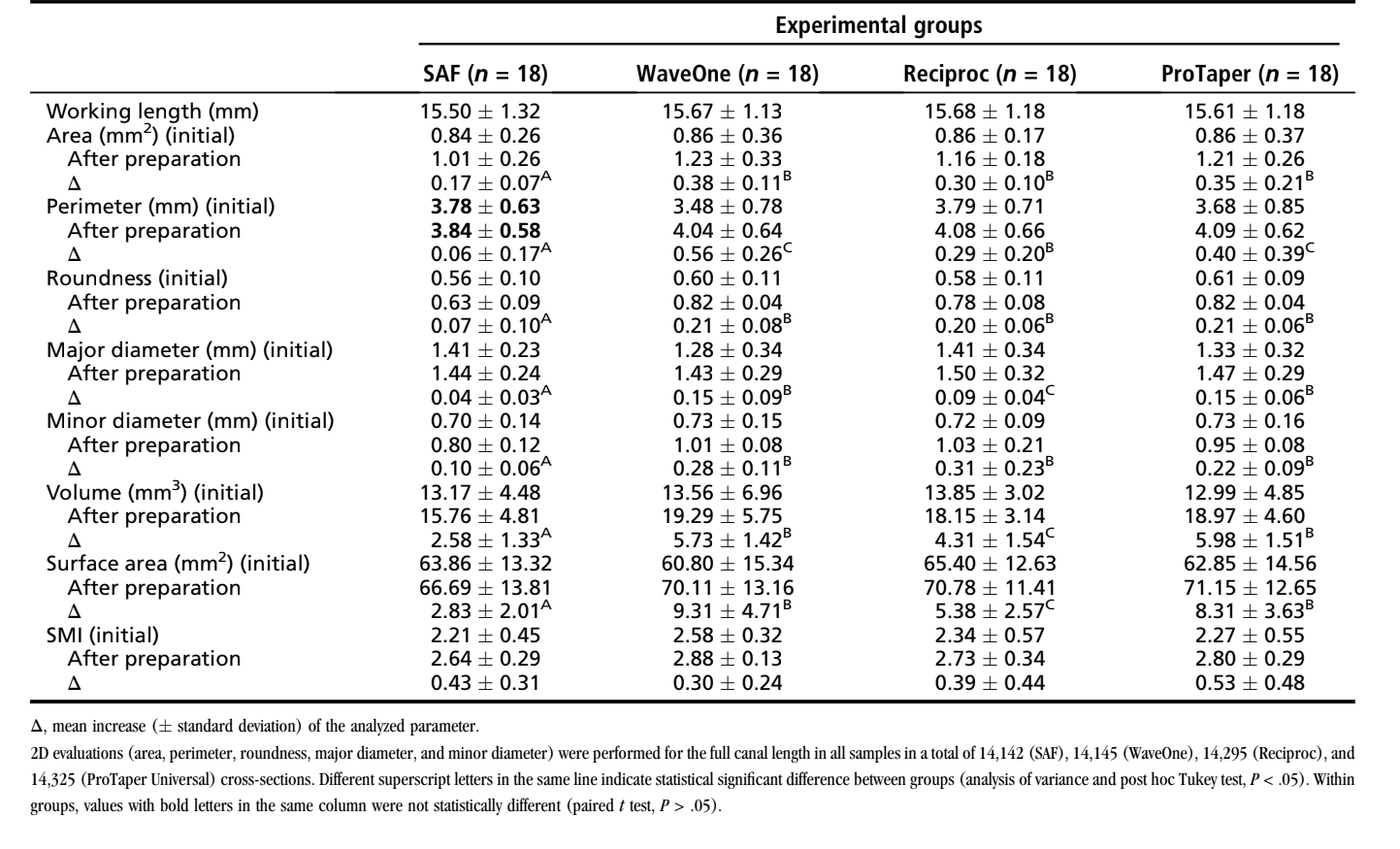
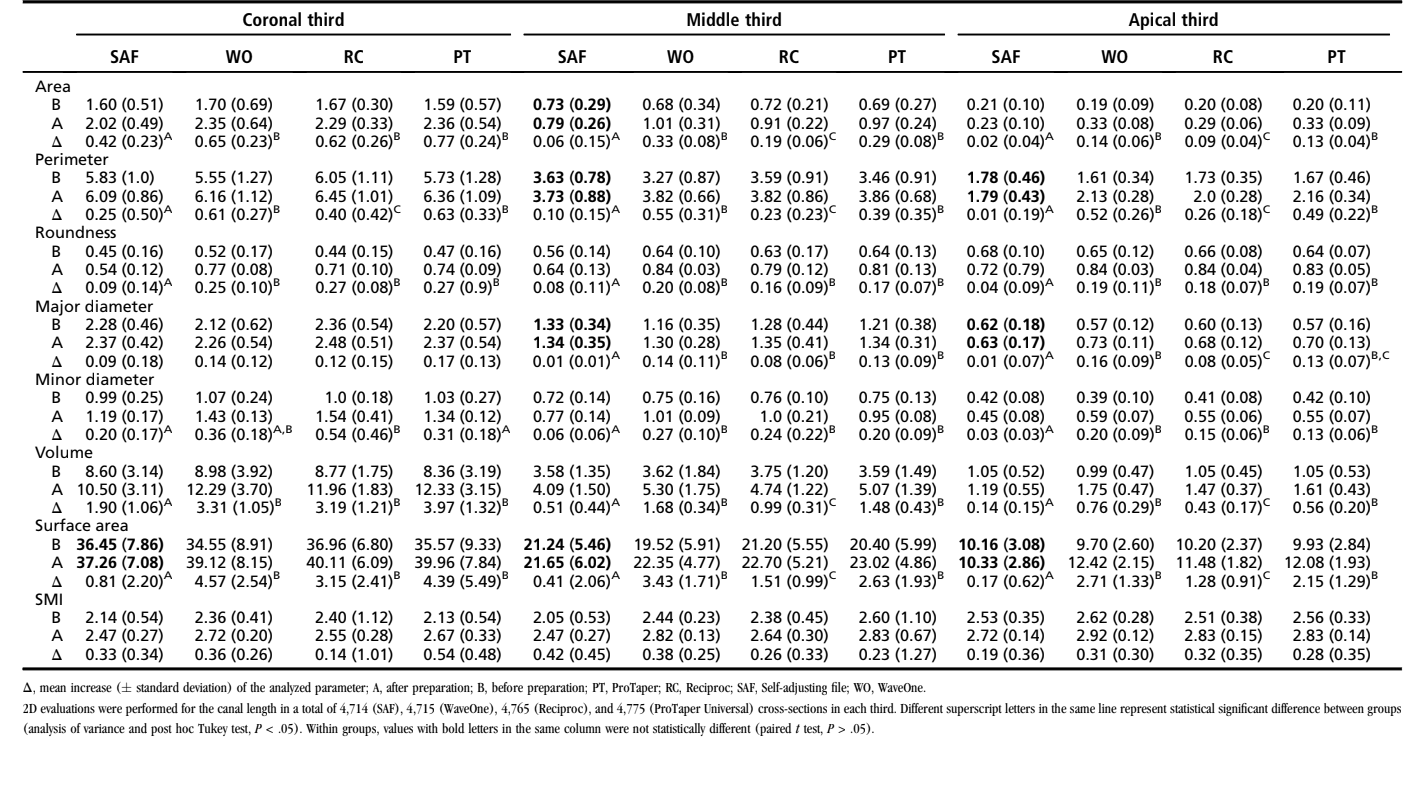
The results of 2D and 3D analysis are detailed in Tables 1 and 2. The paired samples t test revealed that preparation significantly increased all parameters in all groups (P < .05). After preparation, the SAF system presented no significant difference considering some parameters in the coronal (perimeter), middle (area, perimeter, major diameter, surface area), and apical (perimeter, major diameter, surface area) thirds (P > .05). Overall, a comparison between groups revealed that SAF presented the lowest whereas WaveOne and ProTaper Universal showed the highest mean increase in most of the analyzed parameters (P < .05). Reciproc showed intermediate results in some parameters in the coronal (perimeter), middle (area, perimeter, volume and surface area), and apical (area, perimeter, major diameter, volume, and surface area) thirds. SMI analysis revealed no statistical significant difference between groups (P > .05). In light of the present results, the null hypothesis tested was rejected.
Discussion
The present study compared the effects of 3 recently developed single-file systems on root canal geometry by using μCT. One standard rotary system (ProTaper Universal) was used as a reference technique for comparison. The SAF group presented the lowest mean increase in all analyzed parameters, and, in some cases, no significance difference in the mean values before and after preparation was observed. It may be explained because the mean minor diameter at the apical third of the root canal before preparation (0.42 mm) exceeded the maximum enlargement that a 1.5-mm file is able to achieve (similar to a size 40 instrument), which may have interfered with its cutting efficiency. It was shown that the SAF expands into the canal and circumferentially removes a layer of dentin with a back-and-forth grinding motion. Despite the SAF resulting in a more uniform dentin removal than reciprocating or rotary instrumentation, in the present study all systems performed similarly in terms of the amount of touched dentin walls. The brushing motion used in the other groups may explain this similarity.
In the reciprocating and rotary groups, root canal instrumentation resulted in significant gains in canal volumes and surface areas. Overall, the highest mean increase of the parameters was observed in WaveOne and ProTaper groups in comparison with Reciproc. Despite some similarities between WaveOne and Reciproc instruments (driven under reciprocation movement, same alloy, and tip size), differences in their cross-sectional designs and tapers may explain these results. Reciproc has a double-cutting edge S-shaped geometry, whereas WaveOne has a modified convex triangular cross-section with radial lands at the tip and a convex triangular cross-section in the middle and coronal portion of the instrument analogous to the ProTaper instruments. The design of Reciproc (sharp cutting edges and smaller cross-sectional area) also influences its flexibility and cutting efficiency in brushing motion, which may explain similar results to WaveOne and ProTaper in some parameters. On the other hand, the bigger metal mass of ProTaper F4 and WaveOne Large compared with Reciproc R40 might explain the lowest mean increased of other parameters in the latter. The increase in SMI observed in all groups indicated that the canals became more round in shape after the instrumentation. Despite the fact that no statistical difference could be observed between groups, the highest SMI values in the ProTaper and WaveOne groups also reflect their larger taper and stiffness of the tip in comparison with the Reciproc and SAF systems.
The qualitative evaluation showed that all groups presented untouched areas mainly on the lingual side of the middle third of the canal. In mandibular canines, the canal is narrow mesiodistally but usually very extensive buccolingually. The lingual wall is almost slit-like compared with the larger buccal wall, which makes the canal a challenge to shape and clean and may explain this result.
Unfortunately, the present results cannot be directly compared with earlier reports on the evaluation of root canal preparation with reciprocating systems because of differences in the methodological approach. However, the results of these studies showed that the shaping ability of the single-file technique is in accordance with that of the continuous rotation preparation technique, as shown in the present study.
The accuracy and reproducibility of the μCT system have been verified previously, and it is accepted as an important scientific tool for the analysis of different shaping techniques. Because oval-shaped canals represent a challenge to any preparation system, this was the type of canal selected for the present study. Considering that variations in canal geometry before shaping procedures seem to have more influence on the changes that occurred during preparation than the instrumentation techniques themselves, in the present study several attempts have been made to create a reliable baseline, thus ensuring the comparability of the groups.
During canal preparation with the SAF, a special irrigation device is connected to a silicon tube in the instrument providing a continuous flow of 20 mL 2.5% NaOCl solution. The additional activation of the irrigant by its vibrating motion creates turbulence in the root canal, allowing continuous fresh solution and favoring a higher reduction of debris than rotary instruments. Considering this particular feature of the SAF system, in the present study an attempt was made to ensure a similar type, amount, and activation of the irrigant solution in the reciprocating and rotary groups.
Preparation time is dependent on the technique, the numbers of instruments used, and the operator experience. Previous studies showed that reciprocating systems required significantly less time for preparation than rotary instruments. Hence, considering that the time in which an instrument is used within the root canal may influence the amount of dentin removal, in the present study the preparation time included only active instrumentation and was established in 4 minutes on either the reciprocating or rotary groups to allow comparison with SAF group.
Coronal enlargement, canal scouting, and preliminary creation of a glide path are fundamental for the safer use of NiTi rotary instrumentation. A recent study has shown that the WaveOne Primary instrument produced less modification in the canal curvature if used after a glide path, suggesting that the presence of a bigger canal hole improves the performance of the instrument. Although the manufacturer of the Reciproc instrument does not strictly recommend creating a glide path, the root canals were scouted and preflared, and a #20 K-file was used for apical sizing in all experimental groups. This was performed because these procedures reflect the conditions under which root canal treatment is performed as recommended by SAF’s manufacturer. It is noteworthy that only in the coronal third no statistical difference was observed in the mean increase of the major diameter between groups and in most of the analyzed parameters between reciprocating and rotary groups. These results should be interpreted with caution because they did not represent the efficacy of the preparation systems themselves but also the additional action of the LA Axxess bur used for coronal flaring.
In the present study, both reciprocating systems as well as the ProTaper F4 as a final instrument were compared because they have a tip diameter equivalent to an ISO size 40. A 1.5-mm SAF instrument was also chosen because the resulting apical size with this instrument is usually at least equivalent to a #40 file. Instruments were used in the apical direction using an in-and-out pecking motion with a light pressure according to the manufacturer’s instructions. However, once the instrument had negotiated to the WL, it was used in a light brushing motion following recommendations for the preparation of oval-shaped canals, enhancing cleaning of the buccal and lingual recesses. Because of the brushing motion, the mean enlargement of the apical region was equivalent to a size #55 to #60 file in the rotary and reciprocating groups. Clinically, it means that if a single-cone technique was chosen for the obturation procedure, the standardized master cone must be prefitted to the WL.
Thus, the concept of using a single NiTi instrument to prepare the entire root canal is interesting because it is cost-effective and can shorten the learning curve for practitioners to adopt the new technique. Further in vivo research studies are highly recommended to verify the clinical efficacy of these instruments for shaping the root canal.
Conclusions
Within the limitations of this ex vivo study, it can be concluded that the null hypothesis that there is no difference between single- and multiple-file systems in the preparation of oval-shaped canals of mandibular canine teeth has to be rejected. ProTaper Universal and WaveOne systems presented the highest changes of the basic geometric analyzed parameters (area, perimeter, roundness, major diameter, minor diameter, volume, surface area, structure model index) in comparison with the Reciproc and SAF systems. However, used in a brushing motion, all systems performed similarly in terms of the amount of touched dentin walls. Neither technique was capable of completely preparing the oval-shaped root canals.
Author: Marco Aurélio Versiani, Graziela Bianchi Leoni, Liviu Steier, Gustavo De-Deus, Simone Tassani, Jesus Djalma Pécora, Manoel Damião de Sousa-Neto
References:
- Peters OA. Current challenges and concepts in the preparation of root canal systems: a review. J Endod 2004;30:559–67.
- Hülsmann M, Peters OA, Dummer PMH. Mechanical preparation of root canals: shaping goals, techniques and means. Endod Topics 2005;10:30–76.
- Versiani MA, Pécora JD, Sousa-Neto MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002–7.
- De-Deus G, Souza EM, Barino B, et al. The self-adjusting file optimizes debridement quality in oval-shaped root canals. J Endod 2011;37:701–5.
- Alves FR, Almeida BM, Neves MA, et al. Disinfecting oval-shaped root canals: effectiveness of different supplementary approaches. J Endod 2011;37:496–501.
- Siqueira JF Jr, Alves FR, Almeida BM, et al. Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. J Endod 2010;36:1860–5.
- De-Deus G, Barino B, Zamolyi RQ, et al. Suboptimal debridement quality produced by the single-file F2 ProTaper technique in oval-shaped canals. J Endod 2010;36: 1897–900.
- Ricucci D, Siqueira JF Jr, Bate AL, et al. Histologic investigation of root canal-treated teeth with apical periodontitis: a retrospective study from twenty-four patients. J Endod 2009;35:493–502.
- Metzger Z, Teperovich E, Zary R, et al. The self-adjusting file (SAF). Part 1: respecting the root canal anatomy—a new concept of endodontic files and its implementation. J Endod 2010;36:679–90.
- Paqué F, Peters OA. Micro-computed tomography evaluation of the preparation of long oval root canals in mandibular molars with the self-adjusting file. J Endod 2011;37:517–21.
- Peters OA, Paqué F. Root canal preparation of maxillary molars with the self-adjusting file: a micro-computed tomography study. J Endod 2011;37:53–7.
- Bürklein S, Hinschitza K, Dammaschke T, et al. Shaping ability and cleaning effectiveness of two single-file systems in severely curved root canals of extracted teeth: Reciproc and WaveOne versus Mtwo and ProTaper. Int Endod J 2012;45:449–61.
- Berutti E, Chiandussi G, Paolino DS, et al. Effect of canal length and curvature on working length alteration with WaveOne reciprocating files. J Endod 2011;37: 1687–90.
- Berutti E, Chiandussi G, Paolino DS, et al. Canal shaping with WaveOne Primary reciprocating files and ProTaper system: a comparative study. J Endod 2012;38: 505–9.
- Berutti E, Paolino DS, Chiandussi G, et al. Root canal anatomy preservation of WaveOne reciprocating files with or without glide path. J Endod 2012;38:101–4.
- Bürklein S, Sch€afer E. Apically extruded debris with reciprocating single-file and full-sequence rotary instrumentation systems. J Endod 2012;38:850–2.
- Dietrich MA, Kirkpatrick TC, Yaccino JM. In vitro canal and isthmus debris removal of the self-adjusting file, K3, and WaveOne files in the mesial root of human mandibular molars. J Endod 2012;38:1140–4.
- Goldberg M, Dahan S, Machtou P. Centering ability and influence of experience when using WaveOne single-file technique in simulated canals. Int J Dent 2012; 2012:206321.
- Plotino G, Grande NM, Testarelli L, et al. Cyclic fatigue of Reciproc and WaveOne reciprocating instruments. Int Endod J 2012;45:614–8.
- Bergmans L, Van Cleynenbreugel J, Wevers M, et al. A methodology for quantitative evaluation of root canal instrumentation using microcomputed tomography. Int Endod J 2001;34:390–8.
- Versiani MA, Pascon EA, de Sousa CJ, et al. Influence of shaft design on the shaping ability of 3 nickel-titanium rotary systems by means of spiral computerized tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:807–13.
- Peters OA, Laib A, Ruegsegger P, et al. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res 2000;79: 1405–9.
- Versiani MA, Pécora JD, Sousa-Neto MD. The anatomy of two-rooted mandibular canines determined using micro-computed tomography. Int Endod J 2011;44: 682–7.
- Versiani MA, Pécora JD, Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars: a micro-computed tomography study. J Endod 2012;38:977–82.
- Versiani MA, Sousa-Neto MD, Pécora JD. Pulp pathosis in inlayed teeth of the ancient Mayas: a microcomputed tomography study. Int Endod J 2011;44:1000–4.
- Paqué F, Zehnder M, De-Deus G. Microtomography-based comparison of reciprocating single-file F2 ProTaper technique versus rotary full sequence. J Endod 2011;37:1394–7.
- Metzger Z, Zary R, Cohen R, et al. The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. J Endod 2010;36:1569–73.
- You SY, Kim HC, Bae KS, et al. Shaping ability of reciprocating motion in curved root canals: a comparative study with micro-computed tomography. J Endod 2011;37: 1296–300.
- Hildebrand T, Rüegsegger P. Quantification of bone micro architecture with the structure model index. Comput Methods Biomech Biomed Engin 1997;1:15–23.
- Tassani S, Matsopoulos GK, Baruffaldi F. 3D identification of trabecular bone fracture zone using an automatic image registration scheme: a validation study. J Biomech 2012;45:2035–40.
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Topics 2005;10:3–29.
- Yared G. Canal preparation using only one Ni-Ti rotary instrument: preliminary observations. Int Endod J 2008;41:339–44.