
Root and Root Canal Morphology of Four-rooted Maxillary Second Molars: A Micro–Computed Tomography Study
Abstract
Introduction: This study examined the anatomy of 4-rooted maxillary second molars by using micro–computed tomography.
Methods: Twenty-five 4-rooted maxillary second molars were scanned to evaluate the size and curvature of the roots; the distance and spatial configuration between some anatomical landmarks; the number of root canals and the position of apical foramina; the occurrence of fusion of roots and enamel pearls; the configuration of the canal at the apical third; the cross-sectional appearance, the volume, and surface area of the root canals. Data were compared by using analysis of variance post hoc Tukey test (α = 0.05).
Results: The specimens were classified as types I (n = 16), II (n = 7), and III (n = 2). The size of the roots was similar (P > .05), and most of them presented straight with 1 canal, except the mesiobuccal that showed 2 canals in 24% of the samples. The configuration of the pulp chamber was mostly irregular quadrilateral-shaped. The lowest mean distance of the orifices was observed between the buccal roots (P < .05). Accessory canals were present mostly in the apical third. Location of the apical foramina varied considerably. Fusion of roots and enamel pearls occurred in 44% and 8% of the samples, respectively. Mean distance from the pulp chamber floor to the furcation was 2.15 ± 0.57 mm. No statistical differences were found in the bi-dimensional and 3-dimensional analyses (P > .05).
Conclusions: All analyzed parameters showed differences between roots, except for the length of the roots, the configuration of the canals at the apical third, cross-sectional appearance, volume, and surface area of the canals. (J Endod 2012;38:977–982)
It is common knowledge that the goal of endodontic therapy is the thorough cleaning and obturation of the entire root canal system. Therefore, a comprehensive understanding of the root and the root canal morphology is imperative to reduce endodontic failure caused by incomplete root canal preparation and obturation. Despite a wide range of anatomical variations associated with maxillary molars that has been reported, the presence of double palatal roots has been considered as a rare phenomenon most frequently limited to the maxillary second molar teeth. The etiology behind this variation is still unclear, but it is probably related to disturbances of the Hertwig epithelial root sheath by exogenic or endogenic factors during the development of the roots.
Since the first report on endodontic treatment of maxillary molars with 2 palatal roots, similar cases have been published, and some attempt has been made to establish its incidence. In a survey of 1200 maxillary second molars, Libfeld and Rostein found only 0.4% of the sample exhibiting this condition, whereas in a retrospective study of 520 completed endodontic treatments of maxillary second molar teeth, Peikoff et al indicated that the frequency of this variation was nearly 1.4%. Nevertheless, both studies are compromised by lack of methodological accuracy in the detection of these extra roots, considering that the interpretation of these morphologic variations in radiographs is difficult and very often impossible. Thus, neither the inspection nor a 2-dimensional (2D) radiograph could give exact information about the number, location, or morphology of the roots or root canals in an in vivo situation.
In recent years, significant noninvasive technological advances for imaging dental structures have been introduced, including digital radiography, densitometry, magnetic resonance imaging, ultrasound, and computed tomography. The development of X-ray micro–computed tomography (micro-CT) has gained increasing significance in endodontic research because it offers a reproducible technique that can be applied quantitatively as well as qualitatively for the 3-dimensional (3D) assessment of the root canal system.
Although the existence of maxillary second molars with 4 separated roots has been reported by several authors, no study has been undertaken to evaluate its anatomy by using micro-CT. Thus, considering the lack of detailed information on this subject, the aim of this ex vivo study was to investigate the internal and external morphology of this anatomical variation by using micro-CT.
Materials and Methods
After ethics committee approval (protocol 2009.1.972.58.4, CAAE 0072.0.138.000-09), 25 4-rooted human maxillary second molars were selected from a pool of extracted teeth and stored in labeled individual plastic vials containing 0.1% thymol solution until use.
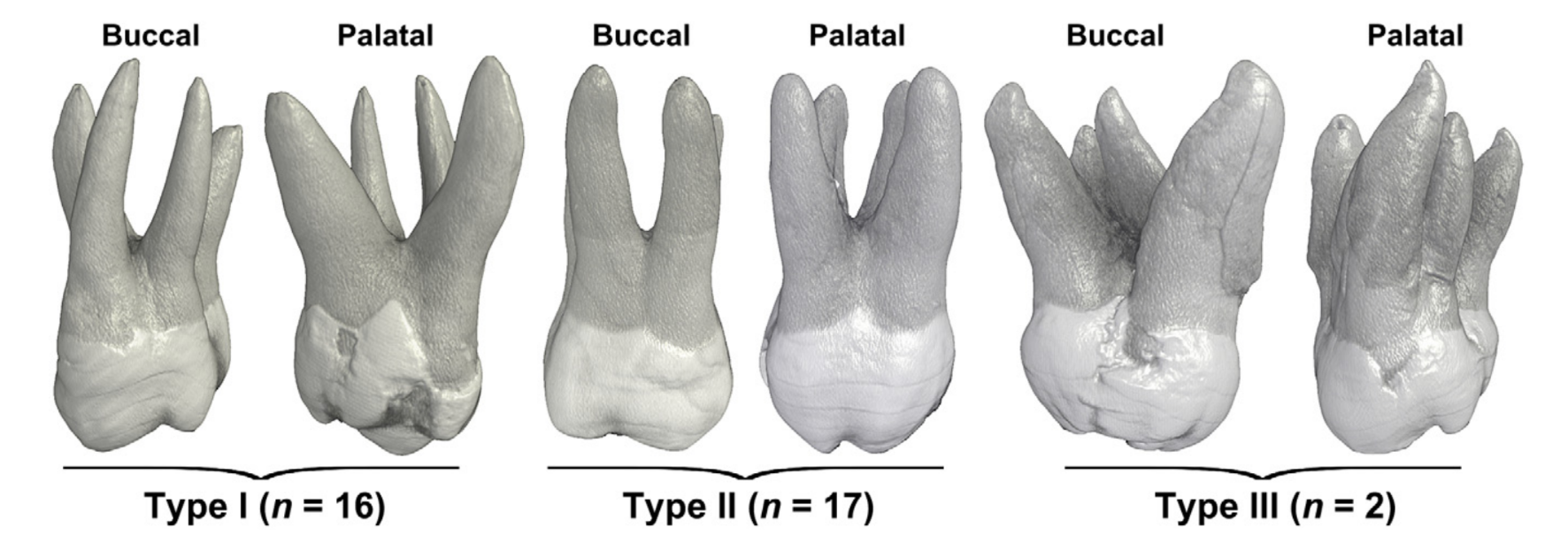
The external morphology of the specimens was classified into 3 types according to the divergence of their roots. In type I, palatal roots were widely divergent and often longer and more tortuous than buccal roots that were less divergent and often ‘‘cow-horn’’ shaped. In type II, roots had blunt apices, run almost parallel to each other, and were often shorter than type I tooth. In type III, palatal roots were less divergent and often shorter than buccal roots that were widely divergent. Then, the size of the mesiobuccal (MB), mesiopalatal (MP), distobuccal (DB), and distopalatal (DP) roots and the distance between the anatomical apexes were measured by using a digital caliper with a resolution of 0.01 mm (Mitutoyo MTI Corporation, Tokyo, Japan). The direction of root curvature and the occurrence of fusion and enamel structures at the root were also evaluated.
After being washed in running water for 24 hours, each tooth was dried, mounted on a custom attachment, and scanned in a micro-CT scanner (SkyScan 1174v2; SkyScan N.V., Kontich, Belgium) at an isotropic resolution of 22.6 mm. Images of each specimen were reconstructed from the apex to the coronal level with dedicated software (NRecon v1.6.4; SkyScan), which provided axial cross sections of the inner structure of the samples. Data Viewer v.1.4.4 software (SkyScan) was used to evaluate the number and location of root canals, the position of the apical foramina, the presence of apical delta, the configuration of the root canal orifices, and the distance from the pulp chamber floor to the furcation. CTAn v1.11 software (Skyscan) was used for 2D evaluation (area, perimeter, roundness, major diameter, and minor diameter) of the root canal 1 mm short of the apical foramen. Volume, surface area, and cross-sectional appearance, expressed as the structure model index (SMI), were also measured. CTVox v.2.2 and CTVol v.2.1 software (Skyscan) were used for 3D visualization of the specimens (supplemental Video S1 is available at www.jendodon.com).
The results of 2D and 3D analysis as well as the distances between some anatomical landmarks were statistically compared by using analysis of variance post hoc Tukey test, with the significance level set as 5%, by using SPSS v17.0 for Windows (SPSS Inc, Chicago, IL).
Results
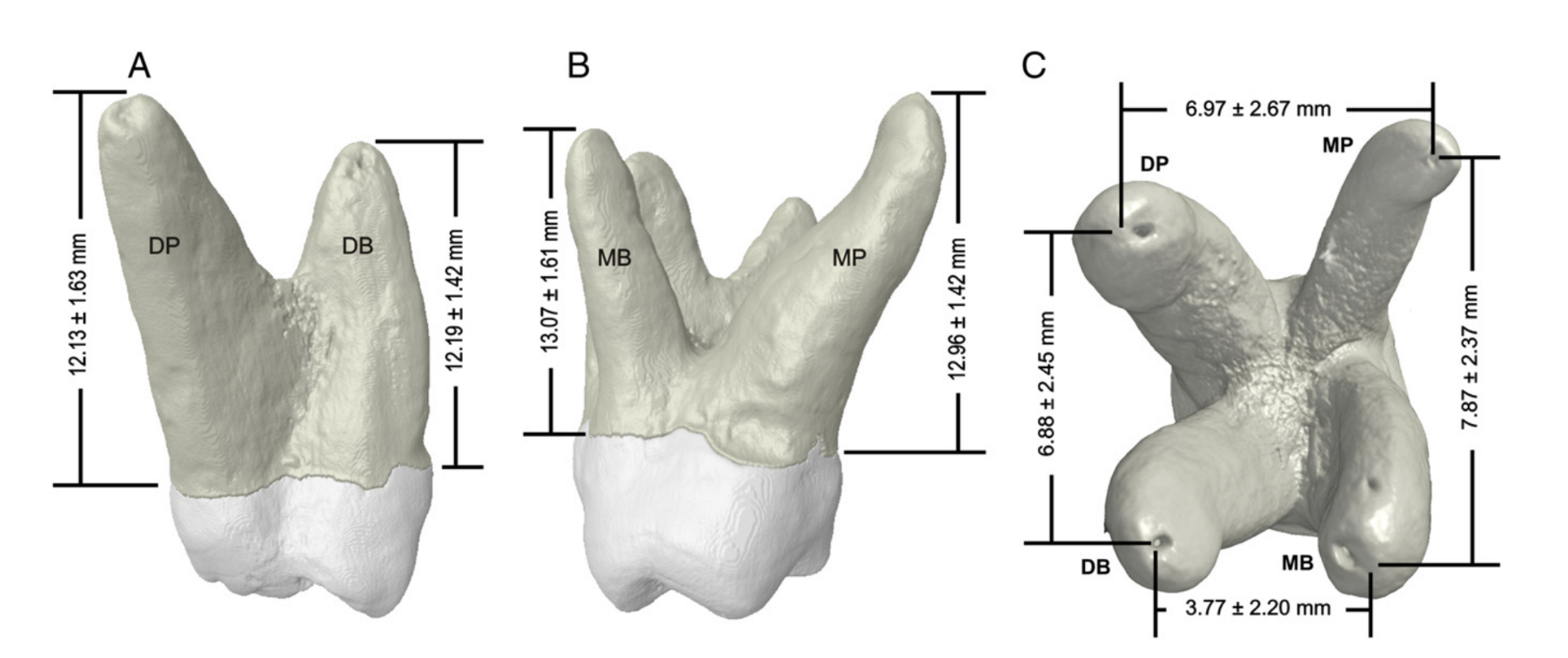
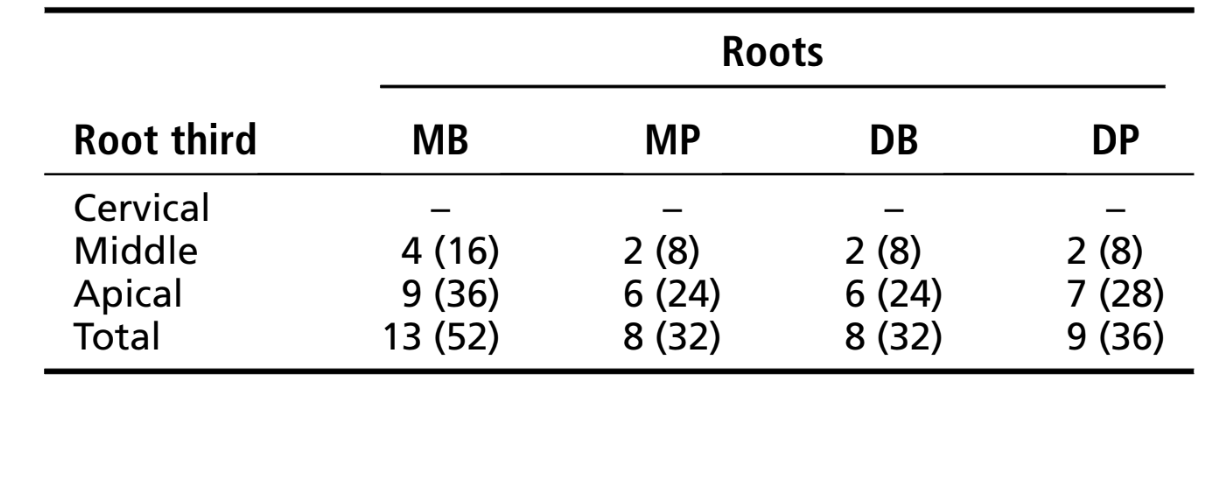
Sixteen specimens were classified as type I (64%), 7 as type II (28%), and 2 as type III (8%) (Fig. 1). Statistical analysis revealed no difference between the length of the roots (P = .07), whereas the mean distance between the apexes of MB and DB roots was significantly lower than MB-MP, MP-DP, and DP-DB distances (P = .0001) (Fig. 2). Most of the roots presented straight from both buccal and proximal views. Considering the buccal perspective, no curvature was observed in the MP root. The MB root curved only distally, whereas DB and DP roots curved in both mesial and distal directions. From a proximal perspective, most curvatures were observed in the MProot. No curvature toward the buccal direction was found in the DB root (Table 1).

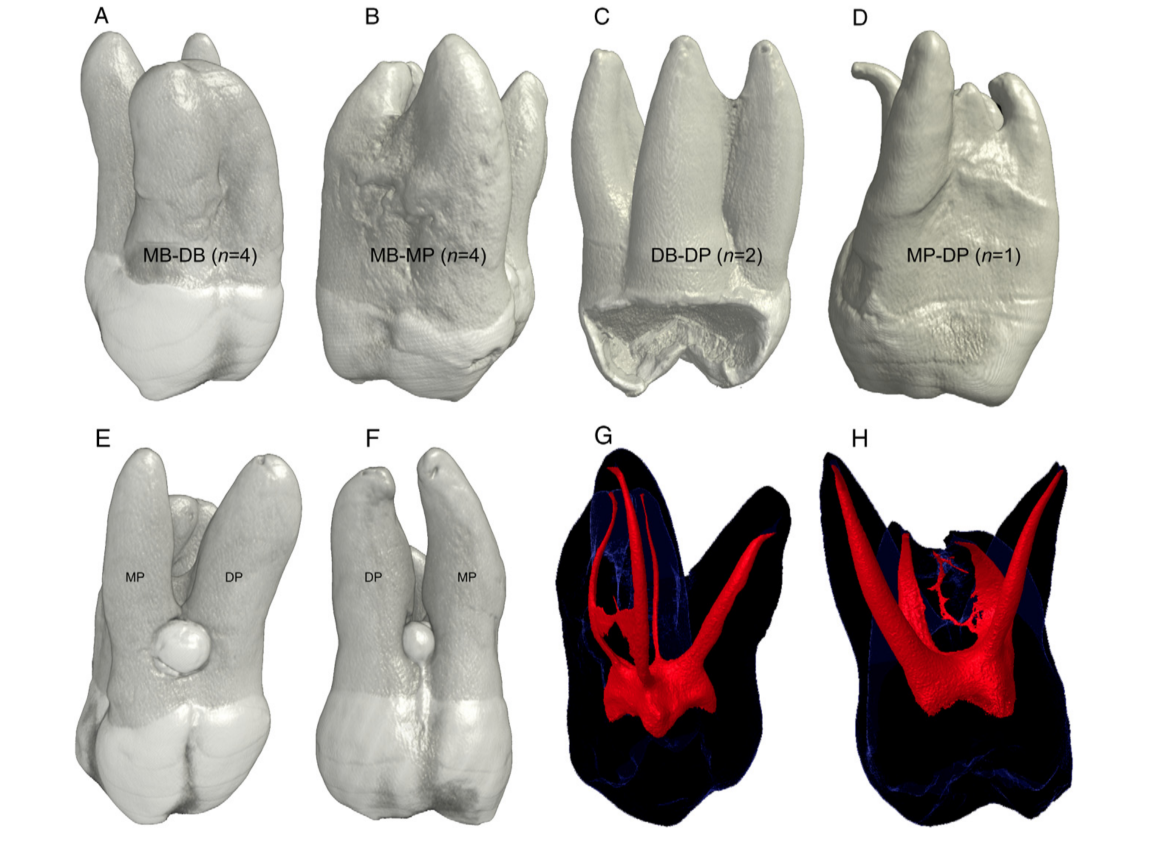
Fusion of roots occurred more often with MB root (n = 8) and less frequently with DP root (n = 3) (Fig. 3A–D). In 2 specimens, the presence of enamel pearl in the furcation area of the palatal roots was observed (Fig. 3E and F). All roots had 1 main canal except the MB, which presented 2 canals in 6 specimens (Fig. 3G and H).
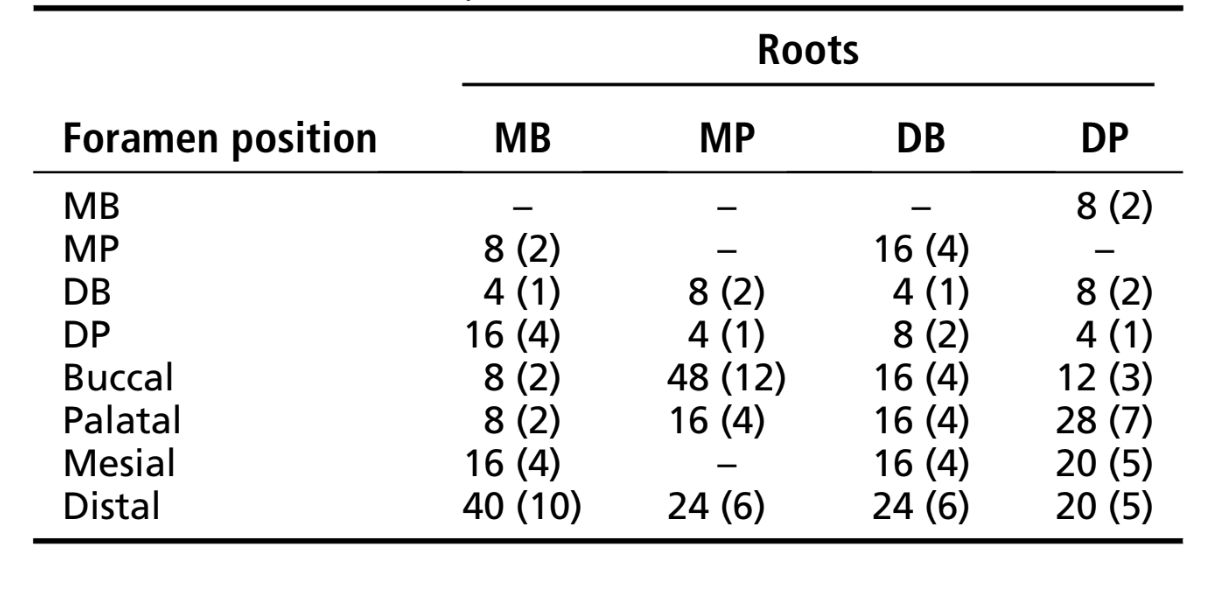
Accessory canals were located mostly in the apical third of the roots, and no furcation canals were found (Table 2). The location of the apical foramina varied considerably, tending to the buccal aspect of the MP roots (48%), to the palatal aspect of the DP roots (28%), and to the distal aspect of the MB (40%) and DB roots (24%) (Table 3). Apical delta was observed only in 8% of the MP (n = 2) and 4% of the DB (n = 1) roots.
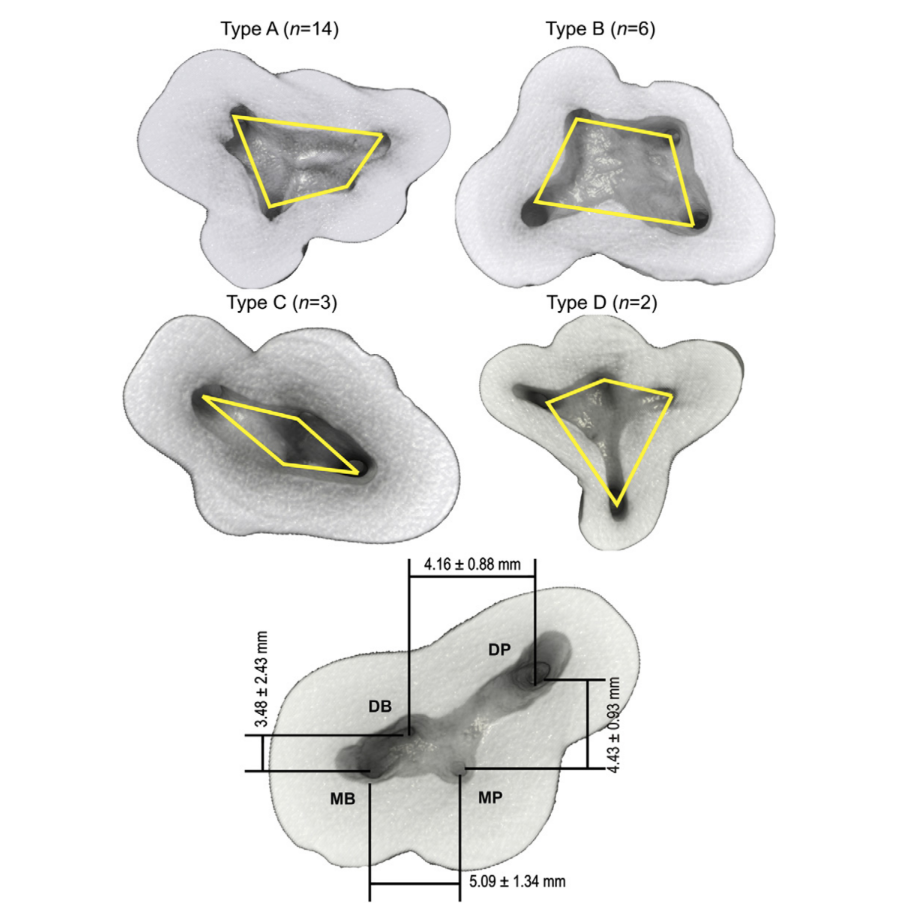
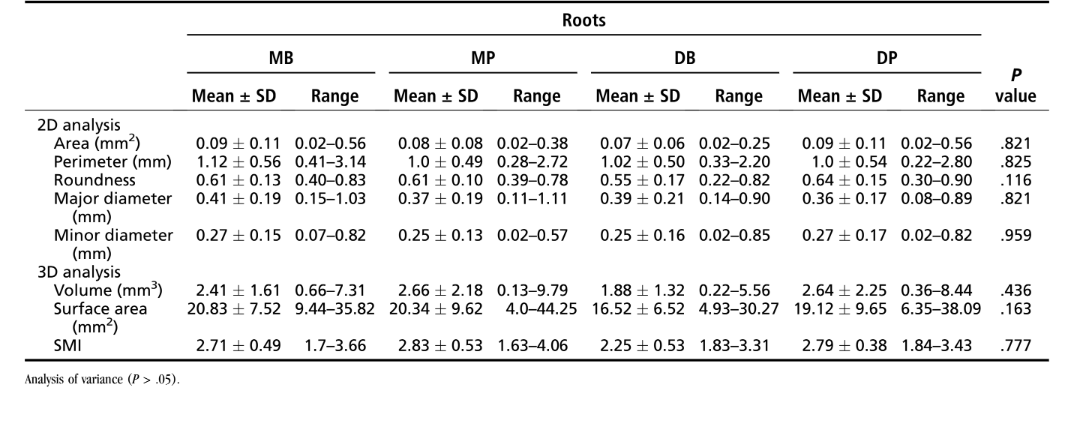
The spatial configurations of the orifices in relation to the pulp chamber floor were classified as type A (irregular quadrilateral-shaped, 56%), type B (trapezoid-shaped, 24%), type C (lozenge-shaped, 12%), and type D (kite-shaped, 8%). Mean distance between the buccal orifices (3.48 ± 2.43 mm) was significantly lower than MP-MB orifice distance (5.09 ± 1.34 mm) (P < .05) (Fig. 4), and the thickness of the pulp chamber floor ranged from 1.20–3.13 mm (2.15 ± 0.57 mm). 2D evaluation of the root canal 1 mm short of the apical foramen (area, perimeter, roundness, major diameter, and minor diameter) as well as volume, surface area, and SMI analysis showed no statistical differences between the roots (P > .05; Table 4).
Discussion
The most extensive study published on the anatomy of 4-rooted maxillary second molars classified 22 molars into 3 types (I–III) according to the separation level and divergence of the roots. Whereas type I consisted of teeth in which the palatal roots were more divergent than the buccal ones, types II and III were based on the size and fusion of roots. In the present study, a new classification system based only on the divergence of the roots is proposed, considering that fusion might occur in different levels of all roots, making this proposal not feasible. Thus, Christie’s types II and III were combined into one category (type II), and a new variation was described as type III. The average size of the roots ranged from 12.13–13.07 mm, similarly to a previous study in which the mean sizes of MB, DB, and palatal roots of 220 3-rooted maxillary second molars were 12.3, 13.0, and 13.6 mm, respectively. The analysis of the external surface of the roots also showed the presence of enamel pearl in the furcation area of 2 specimens as well as Christie et al, who observed its presence in 3 specimens during the radiographic examination of 16 4-rooted maxillary second molars. The knowledge of the direction of curvature of each root is of particular importance, especially when the curvature is toward the buccal or palatal direction, because it could not be visualized in radiographs. In the present study, most of the roots presented straight from both buccal and proximal perspectives and most of the curvatures toward mesial or distal. Special attention should be given in relation to MP roots by considering that from a proximal perspective, most curve toward buccal (20%). Similarly, eccentric placement of the apical foramina was recognized in all specimens, and its location varied considerably, as observed in other studies.
A new classification system based on the configuration of the canal orifices in relation to the pulp chamber floor was also proposed. The shortest distance observed between the canal orifices of buccal roots might be explained by considering that most of the sample comprised type I configuration. Besides, the position of the canal orifices observed in the present study suggests that the access cavity on 4-rooted maxillary molars should be wider than usual on the palatal aspect, with the access outline to be trapezoidal rather than triangular or square. This is especially important in divergent palatal roots (type I) because the MP canal orifice might be difficult to visualize. Such classifications are expected to be valuable for making proper treatment plans and help the clinician to diagnose and negotiate the root canal anatomy.
There is a wide range of variation in the literature with respect to the number of canals in maxillary molars. In the present study, all roots had only 1 main canal, except the MB root that presented 2 canals in 26% of the sample. This frequency, however, was lower than previous reports that showed a percentage of 2 canals in the MB roots of 3-rooted maxillary second molars to be higher than 40%. This difference might be related to the small sample, but it is supported by most of previous reports in which authors failed to find a second canal in the MB root of 4-rooted maxillary molars.
In the present study, furcation canals were not found, and the mean thickness of the pulp floor (2.15 ± 0.57 mm) was similar to a previous study in which the distance from the furcation to the pulp floor in maxillary molars has been shown to be #3 mm. In this context, the risk of accidental furcation perforation should be considered.
Accessory canals were observed mostly at the apical third of the root, and its frequency was higher (38%) than a previous study (23.3%) that evaluated 3-rooted maxillary second molars. This dissimilarity might be explained by considering differences of the samples and methods used to evaluate the root canal morphology.
Effective canal debridement relies on accurate determination of the working length and adequate apical canal enlargement, because it can overcome the potential limits of irrigation in the apical area, optimizing root canal disinfection. In this way, the knowledge of the diameter of the canal in the apical third might enable the clinician to provide a more predictable root canal preparation. In the present study, the major diameter of the canal 1 mm short of the apical foramen averaged 0.4 mm, which means that debridement in the apical third could be improved with a larger instrument than an ISO size 40.
The cross-sectional appearance of the root canal, round or more ribbon-shaped, is expressed as roundness. This index varies from 0 (parallel plates) to 1 (perfect ball). In this study, the average round- ness of the root canal 1 mm short of the apical foramen ranging from 0.55–0.64 indicated that the canals of 4-rooted maxillary second molars are oval-shaped in this region, in accordance with a previous publication that demonstrated similar configuration of the canals in the apical third of 3-rooted maxillary second molars.
Algorithms used in micro-CT evaluation allow further measurement of basic geometric parameters such as volume and surface area as well as additional descriptors of canal shape such as SMI. The SMI describes the plate- or cylinder-like geometry of an object and is determined by an infinitesimal enlargement of the surface, whereas the change in volume is related to changes of surface area, that is to the convexity of the structure. If a perfect plate is enlarged, the surface area does not change, yielding an SMI of 0. However, if a rod is expanded, the surface area increases with the volume and the SMI is normed, so that perfect rods are assigned an SMI score of 3. In the present study, the mean SMI results indicated that the root canals of the 4-rooted maxillary second molar teeth had a cylinder-like geometry. Nonetheless, the results of volume and surface area cannot be compared because there is no information on this subject in the literature to date. Thus, the clinical relevance of such findings is still to be determined.
The number and morphology of the root canal system can vary considerably among teeth. The frequency of 2 palatal roots in maxillary second molars has been reported to be very low, but it should not be left out of consideration during endodontic treatment. An important tool for detecting variations of the root canal in maxillary molars has been the radiograph; however, superposition of the anatomical structures in this region might result in failure to diagnose a second palatal root. In this condition, a root canal might be left untreated, which could result in failure. Therefore, other diagnostic methods such as spiral and cone-beam CT, as well as the surgical operative microscope, could be useful, supporting the clinicians within the diagnosis and treatment of 4-rooted maxillary second molars.
Conclusions
Considering the evaluation of the external and internal anatomy of 4-rooted maxillary second molars, it can be concluded that most of the samples were classified as type I. Fusion of roots and enamel pearls were observed. Most of the roots presented straight with 1 main canal, except the MB root, which presented 2 canals in 24% of the samples. There were no furcation canals. Accessory canals were located mostly in the apical third of the roots, and apical delta was observed in 12% of the roots. The location of the apical foramina varied considerably. Fifty-six percent of the samples presented an irregular quadrilateral-shaped orifice configuration. The mean distance from the pulp chamber floor to the furcation was 2.15 ± 0.57 mm. No difference was observed between roots by considering their length, the configuration of the root canal in the apical third, the SMI, the volume, and the surface area of the root canals.
Authors: Marco Aurélio Versiani, Jesus Djalma Pécora, Manoel Damião de Sousa-Neto
References:
- Setzer FC, Boyer KR, Jeppson JR, Karabucak B, Kim S. Long-term prognosis of endodontically treated teeth: a retrospective analysis of preoperative factors in molars. J Endod 2011;37:21–5.
- Cleghorn BM, Christie WH, Dong CC. Root and root canal morphology of the human permanent maxillary first molar: a literature review. J Endod 2006;32:813–21.
- Aggarwal V, Singla M, Logani A, Shah N. Endodontic management of a maxillary first molar with two palatal canals with the aid of spiral computed tomography: a case report. J Endod 2009;35:137–9.
- Baratto-Filho F, Fariniuk LF, Ferreira EL, P´ecora JD, Cruz-Filho AM, Sousa-Neto MD. Clinical and macroscopic study of maxillary molars with two palatal roots. Int Endod J 2002;35:796–801.
- Barbizam JV, Ribeiro RG, Tanomaru Filho M. Unusual anatomy of permanent maxillary molars. J Endod 2004;30:668–71.
- Benenati FW. Maxillary second molar with two palatal canals and a palatogingival groove. J Endod 1985;11:308–10.
- de Almeida-Gomes F, Maniglia-Ferreira C, dos Santos RA. Two palatal root canals in a maxillary second molar. Aust Endod J 2007;33:82–3.
- Deveaux E. Maxillary second molar with two palatal roots. J Endod 1999;25: 571–3.
- Di Fiore PM. A four-rooted quadrangular maxillary molar. J Endod 1999;25:695–7.
- Gopikrishna V, Reuben J, Kandaswamy D. Endodontic management of a maxillary first molar with two palatal roots and a single fused buccal root diagnosed with spiral computed tomography: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;105:e74–8.
- Holderrieth S, Gernhardt CR. Maxillary molars with morphologic variations of the palatal root canals: a report of four cases. J Endod 2009;35:1060–5.
- Jacobsen EL, Nii C. Unusual palatal root canal morphology in maxillary molars. Endod Dent Traumatol 1994;10:19–22.
- Shin SJ, Park JW, Lee JK, Hwang SW. Unusual root canal anatomy in maxillary second molars: two case reports. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007; 104:e61–5.
- Stone LH, Stroner WF. Maxillary molars demonstrating more than one palatal root canal. Oral Surg Oral Med Oral Pathol 1981;51:649–52.
- Ulusoy OI, Gorgul G. Endodontic treatment of a maxillary second molar with 2 palatal roots: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007;104:e95–7.
- Peikoff MD, Christie WH, Fogel HM. The maxillary second molar: variations in the number of roots and canals. Int Endod J 1996;29:365–9.
- Nanci A. Ten Cate’s oral histology: development, structure, and function. 7th ed. St Louis, MO: Mosby, Inc; 2007.
- Slowey RR. Radiographic aids in the detection of extra root canals. Oral Surg Oral Med Oral Pathol 1974;37:762–72.
- Christie WH, Peikoff MD, Fogel HM. Maxillary molars with two palatal roots: a retrospective clinical study. J Endod 1991;17:80–4.
- Libfeld H, Rotstein I. Incidence of four-rooted maxillary second molars: literature review and radiographic survey of 1,200 teeth. J Endod 1989;15:129–31.
- Blattner TC, George N, Lee CC, Kumar V, Yelton CD. Efficacy of cone-beam computed tomography as a modality to accurately identify the presence of second mesiobuccal canals in maxillary first and second molars: a pilot study. J Endod 2010;36:867–70.
- Versiani MA, Pécora JD, Sousa-Neto MD. The anatomy of two-rooted mandibular canines determined using micro-computed tomography. Int Endod J 2011;44: 682–7.
- Peters OA, Laib A, Ruegsegger P, Barbakow F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res 2000;79: 1405–9.
- Versiani MA, Pécora JD, Sousa-Neto MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002–7.
- Solomonov M, Paqué F, Fan B, Eilat Y, Berman LH. The challenge of C-shaped canal systems: a comparative study of the self-adjusting file and ProTaper. J Endod 2012; 38:209–14.
- Pécora JD, Woelfel JB, Sousa-Neto MD. Morphologic study of the maxillary molars: part I—external anatomy. Braz Dent J 1991;2:45–50.
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589–99.
- Hess W, Zurcher E. The anatomy of the root canals of the teeth of the permanent and deciduous dentitions. London: John Bale, Sons & Danielsson, Ltd; 1925.
- De Deus QD. Frequency, location, and direction of the lateral, secondary, and accessory canals. J Endod 1975;1:361–6.
- Lee JH, Kim KD, Lee JK, et al. Mesiobuccal root canal anatomy of Korean maxillary first and second molars by cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2011;111:785–91.
- Neelakantan P, Subbarao C, Ahuja R, Subbarao CV, Gutmann JL. Cone-beam computed tomography study of root and canal morphology of maxillary first and second molars in an Indian population. J Endod 2011;36:1622–7.
- Zhang R, Yang H, Yu X, Wang H, Hu T, Dummer PM. Use of CBCT to identify the morphology of maxillary permanent molar teeth in a Chinese subpopulation. Int Endod J 2011;44:162–9.
- Deutsch AS, Musikant BL. Morphological measurements of anatomic landmarks in human maxillary and mandibular molar pulp chambers. J Endod 2004;30: 388–90.
- Fornari VJ, Silva-Sousa YT, Vanni JR, Pécora JD, Versiani MA, Sousa-Neto MD. Histological evaluation of the effectiveness of increased apical enlargement for cleaning the apical third of curved canals. Int Endod J 2010;43:988–94.
- Wu MK, R’Oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89: 739–43.