
Micro–Computed Tomography Assessment of Dentinal Micro-cracks after Root Canal Preparation with TRUShape and Self-Adjusting File Systems
Abstract
Introduction: The aim of the present study was to evaluate the percentage frequency of dentinal micro-cracks observed after root canal preparation with TRUShape and Self-Adjusting File (SAF) systems by means of micro–computed tomography imaging analysis. A conventional full-sequence rotary system (BioRace) and a single-file reciprocation system (Reciproc) were used as reference techniques for comparison because of their known assertive cutting efficiency.
Methods: Forty anatomically matched mandibular incisors were selected, scanned at a resolution of 14.25 mm, and assigned to 4 experimental groups (n = 10), according to the preparation protocol: TRUShape, SAF, BioRace, and Reciproc systems. After the experimental procedures, the specimens were scanned again, and the registered preoperative and postoperative cross-section images of the roots (n = 70,030) were screened to identify the presence of dentinal micro-cracks.
Results: Overall, dentinal defects were observed in 28,790 cross-section images (41.11%). In the TRUShape, SAF, BioRace, and Reciproc groups, dentinal micro-cracks were visualized in 56.47% (n = 9842), 42.38% (n = 7450), 32.90% (n = 5826), and 32.77% (n = 5672) of the slices, respectively. All dentinal defects observed in the postoperative data sets were already present in the corresponding preoperative images.
Conclusions: None of the preparation systems induced the formation of new dentinal micro-cracks. (J Endod 2016;■:1–4)
Vertical root fracture is a clinical complication that may lead to tooth extraction and has been described in either treated or non-endodontically treated teeth. During the last few years, several studies have reported a causal relationship between mechanical preparation of the root canal with nickel-titanium (NiTi) instruments and the formation of dentinal micro-cracks, which may potentially develop into vertical root fracture.
It has been speculated that the design and the hard-hitting cutting ability of the preparation systems are the main reasons associated with the development of dentinal defects, because they might generate damaging forces toward dentin. Recently, a novel heat-treated NiTi system named TRUShape 3D Conforming Files (Dentsply Tulsa Dental Specialties, Tulsa, OK) has been introduced into the market, claiming to preserve more dentinal structure while providing an optimized canal debridement. The TRUShape system uses the same symmetric triangular cross section but displays a proprietary file design that resembles an S-shape configuration, providing an ability to flex within the canal, creating an envelope of motion kinematics. Another system that is able to preserve more dentin is the Self-Adjusting File (SAF) (ReDent-Nova, Ra’anana, Israel). The SAF is a hollow file designed as a compressible cylinder composed of a thin NiTi lattice with an abrasive surface. It has the ability to adapt its shape to the root canal anatomy, applying a constant and delicate pressure on the canal walls, which might help to reduce the incidence of dentinal defects. This system operates with a continuous flow of irrigant running through the instrument, allowing continuous replacement.
To date, no studies have evaluated the incidence of dentinal micro-cracks resulting from the use of the claimed less aggressive cutting instruments (TRUShape and SAF systems) by using micro– computed tomography (micro-CT) imaging technology. Therefore, the aim of the present study was to evaluate the frequency of dentinal micro-cracks observed after root canal preparation with TRUShape and SAF systems through micro-CT imaging analysis. A conventional full-sequence rotary system (BioRace; FKG Dentaire, La-Chaux-de-Fonds, Switzerland) and a single-file reciprocation system (Reciproc; VDW, Munich, Germany) were used as reference techniques for comparison because of their known assertive cutting efficiency. The hypothesis tested was that there would be differences in the frequency of dentinal micro-crack generation between the groups.
Materials and Methods
Sample Size Estimation
Sample size was derived from the effect size of dentinal defects promoted by rotary and reciprocating systems by Bürklein et al, in which the percentage sum of the sample with complete and incomplete dentinal defects varied from 18.3% to 51.6%. Chi-square test family and variance statistical test (G*Power 3.1 for Macintosh; Heinrich Heine, Universität Düsseldorf, Düsseldorf, Germany), with a = 0.05 and b = 0.95, output 8 specimens as the minimum ideal size required for observing the same frequency of instrument-induced defects over dentin.
Sample Selection and Scanning
After approval of the local Ethics Committee, 127 straight mandibular incisors were obtained from a pool of teeth. The specimens were initially inspected with the aid of a stereomicroscope under ×12 magnification. The exclusion criteria comprised teeth with preexisting cracks or not patent to the canal length with a size 10 K-file (Dentsply Maillefer, Baillagues, Switzerland). As a result, 102 specimens were selected and scanned in a micro-CT device (SkyScan 1173; Bruker-microCT, Kontich, Belgium) operated at 70 kV and 114 mA, with a low resolution (70 mm). Then, 40 mandibular incisors with a canal ratio of long to short diameter of more than 2.5 at 5-mm level from the root apex were selected and stored in 0.1% thymol solution at 5◦C. These specimens were scanned again at an increased resolution (14.25 mm) per- formed by 360◦ rotation around the vertical axis, rotation step of 0.5◦, camera exposure time of 7000 milliseconds, and frame averaging of 5, with a 1.0-mm-thick aluminum filter. Images of each specimen were reconstructed (NRecon v.1.6.10; Bruker-microCT), providing axial cross sections of their inner structure by using standardized parameters for beam hardening (40%), a ring artifact correction value of 10, and similar contrast limits. The volume of interest was selected to extend from the cementoenamel junction to the apex of the root, resulting in the acquisition of 800–900 transverse cross sections per tooth.
Root Canal Preparation
The apexes were sealed with hot glue and embedded into polyvinyl siloxane to create a closed-end system. After access cavity preparation, a glide path was created by scouting a stainless steel size 20 K-file (Dentsply Maillefer) up to the working length (WL), which was established by deducting 1 mm from the canal length. Then, the specimens were randomly assigned to 4 experimental groups (n = 10), according to the following protocols.
TRUShape. By using an electric motor (VDW Silver; VDW) preset at 300 rpm and 3 Ncm, TRUShape instruments were used with a gentle in-and-out motion in the following sequence: 20/.08v (two thirds of the WL), 20/.06v (full WL), and 25/.06v (full WL). The instruments were advanced to the midroot in 2 to 5 mm and then in further 2- to 3-mm amplitudes toward the WL.
SAF. A 1.5-mm diameter SAF instrument was operated to the WL with an in-and-out motion by using an RDT3 head (ReDent-Nova) adapted to a vibrating handpiece (GentlePower Lux 20LP; KaVo, Biberach, Germany). Continuous irrigation with 5.25% NaOCl was applied throughout the procedure at a flow rate of 5 mL/min by using a special irrigation apparatus (VATEA; ReDent-Nova).
BioRace. BR0 (25/.08), BR1 (15/.05), BR2 (25/.04), and BR3 (25/.06) NiTi rotary instruments (FKG) were used at 500–600 rpm and 1 Ncm in a crown-down manner up to the WL by using a gentle in-and-out pecking motion. After 3 steady strokes, the file was removed from the canal and cleaned.
Reciproc. R25 instrument (25/.08) was moved in the apical direction by using a slow in-and-out pecking motion of about 3 mm in amplitude with light apical pressure in a reciprocating motion (‘RECIPROC ALL’) powered by an electric motor (VDW Silver) until the WL was reached. After 3 pecking motions, the instrument was removed from the canal and cleaned. The WL was reached in the third wave of instrumentation for all teeth.
All experimental procedures were performed by an experienced operator after training with the systems. Irrigation was performed by using a total of 40 mL 5.25% NaOCl per tooth. Apical patency was confirmed with a size 10 K-file after each file use. After preparation, a postoperative micro-CT scan of each specimen was performed by using the aforementioned parameters.
Dentinal Micro-cracks Evaluation
The preoperative and postoperative image stacks of the specimens were co-registered by using the affine algorithm of the 3D Slicer v.4.5.0 software (available from http://www.slicer.org). Then, the cross-section images of the mandibular incisors were screened from the cementoenamel junction to the apex (n = 70,030) by 3 pre-calibrated examiners. First, postoperative images were analyzed, and the cross-section number in which a dentinal micro-crack had been observed was recorded. Afterward, the preoperative corresponding cross-section image was also examined to verify the existence of the defect. To validate the screening process, image analyses were repeated twice at 2-week intervals; in the case of divergence, the images were examined together until an agreement was reached. In this study, dentinal micro-cracks or dentinal defects were defined as all lines observed on the cross-section slice that extended either from the outer root surface into the dentin or from the root canal lumen to the dentin.
Results
Overall, dentinal defects were observed in 28,790 cross-section images (41.11%). In the TRUShape, SAF, BioRace, and Reciproc groups, dentinal micro-cracks were visualized in 56.47% (n = 9842), 42.38% (n = 7450), 32.90% (n = 5826), and 32.77% (n = 5672) of the slices, respectively. All dentinal defects observed in the postoperative data sets were already present in the corresponding preoperative images (Fig. 1), indicating that no new micro-cracks were observed after root canal preparation with the tested systems.
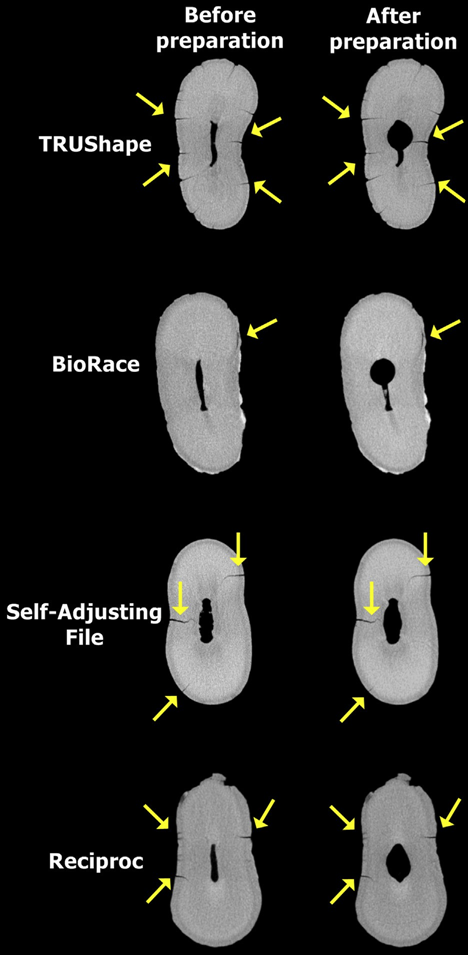
showing the presence of dentinal micro-cracks (yellow arrows) before andafter root canal preparation with TRUShape, BioRace, SAF, and Reciproc systems.
Discussion
This in vitro study evaluated the incidence of dentinal micro-cracks after root canal preparation with TRUShape, SAF, BioRace, and Reciproc systems. To the best of our knowledge, this is the first study assessing the potential correlation between the use of TRUShape and SAF systems and dentinal micro-cracks by using a nondestructive with Reciproc system. Similarly, Saber and Schäfer found the incidence of dentinal defects to be 26% in the group instrumented with Reciproc system. This discrepancy in the results may be explained by an essential difference in the analytical method used. The current body of evidence correlating mechanical preparation and the development of dentinal micro-cracks is mainly based on root-sectioning methods and direct observation by some sort of optical microscopy. As previously stated, these methods present a meaningful disadvantage related to its own destructive nature, which is probably the main cause of the reported outcomes. Although the control groups that used non-prepared teeth in the sectioning studies seemed to validate the experimental design because no dentinal defects were detected, they do not take into consideration the potential damage to dentin produced by the interplay of the mechanical preparation, the chemical attack of the NaOCl-based irrigation, and the sectioning procedures.
Recently, De-Deus et al reported that there was no causal relationship between canal preparation with rotary/reciprocating systems and micro-cracks formation, which is in accordance with the results presented in the current study. The similarities between these studies are related to the use of micro-CT imaging as an assessment tool. Micro-CT nondestructive technology provides the possibility to examine the dentinal tissue before any root canal procedure, which is a very suitable and important feature. It also presents several advantages over the well-established root-sectioning approach. Whereas the latter allows the analysis of only a few slices per sample, which may result in a loss of information, the highly accurate micro-CT method permits the evaluation of hundreds of slices per tooth. This explains the lower frequency of dentinal micro-cracks observed in the control groups of root-sectioning models, which usually investigate a few slices compared with micro-CT studies. Also, this method enables not only the visualization of preexisting dentinal defects but also their precise location throughout the root before and after root canal preparation, improving the internal validity of the experiment as each specimen acts as its own control. In addition, micro-CT technology permits overlapping further experiments on the same specimens, tracking the development of dentinal defects after root canal filling, canal retreatment, post-space preparation, and post-removal procedures. It is important to stress that the crack propagation after instrumentation was not evaluated herein. However, we are aware that this is an important point, and future studies should focus on a three-dimensional longitudinal evaluation, thus allowing us to estimate the cracks propagation in a reliable way.
Conclusion
Under the conditions of the current study, it can be concluded that none of the preparation systems induced the formation of new dentinal micro-cracks.
Authors: Mario Luis Zuolo, Gustavo De-Deus, Felipe Gonçalves Belladonna, Emmanuel João Nogueira Leal da Silva, Ricardo Tadeu Lopes, Erick Miranda Souza, Marco Aurélio Versiani, Alexandre Augusto Zaia
References:
- Zadik Y, Sandler V, Bechor R, Salehrabi R. Analysis of factors related to extraction of endodontically treated teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:e31–5.
- Chan CP, Tseng SC, Lin CP, et al. Vertical root fracture in non-endodontically treated teeth: a clinical report of 64 cases in Chinese patients. J Endod 1998;24:678–81.
- Chan CP, Lin CP, Tseng SC, Jeng JH. Vertical root fracture in endodontically versus nonendodontically treated teeth: a survey of 315 cases in Chinese patients. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1999;87:504–7.
- Hin ES, Wu MK, Wesselink PR, Shemesh H. Effects of Self-Adjusting File, Mtwo, and ProTaper on the root canal wall. J Endod 2013;39:262–4.
- Liu R, Hou BX, Wesselink PR, et al. The incidence of root microcracks caused by 3 different single-file systems versus the ProTaper system. J Endod 2013;39: 1054–6.
- Ashwinkumar V, Krithikadatta J, Surendran S, Velmurugan N. Effect of reciprocating file motion on microcrack formation in root canals: an SEM study. Int Endod J 2014;47:622–7.
- Karataş E, Gündüz HA, Kırıcı DÖ, Arslan H. Incidence of dentinal cracks after root canal preparation with ProTaper Gold, Profile Vortex, F360, Reciproc and ProTaper Universal instruments. Int Endod J 2015; http://dx.doi.org/10.1111/iej.12541 [Epub ahead of print].
- Kfir A, Elkes D, Pawar A, et al. Incidence of microcracks in maxillary first premolars after instrumentation with three different mechanized file systems: a comparative ex vivo study. Clin Oral Investig 2016;21:405–11.
- Wilcox LR, Roskelley C, Sutton T. The relationship of root canal enlargement to finger-spreader induced vertical root fracture. J Endod 1997;23:533–4.
- Versiani MA, Souza E, De-Deus G. Critical appraisal of studies on dentinal radicular microcracks in endodontics: methodological issues, contemporary concepts, and future perspectives. Endod Topics 2015;33:87–156.
- Bortoluzzi EA, Carlon D Jr, Meghil MM, et al. Efficacy of 3D conforming nickel titanium rotary instruments in eliminating canal wall bacteria from oval-shaped root canals. J Dent 2015;43:597–604.
- Peters OA, Arias A, Paqué F. A micro-computed tomographic assessment of root canal preparation with a novel instrument, TRUShape, in mesial roots of mandibular molars. J Endod 2015;41:1545–50.
- Bonessio N, Arias A, Lomiento G, Peters OA. Effect of root canal treatment procedures with a novel rotary nickel titanium instrument (TRUShape) on stress in mandibular molars: a comparative finite element analysis. Odontology 2015;105: 54–61.
- Hof R, Perevalov V, Eltanani M, et al. The self-adjusting file (SAF): part 2—mechanical analysis. J Endod 2010;36:691–6.
- Metzger Z, Teperovich E, Zary R, et al. The self-adjusting file (SAF): part 1— respecting the root canal anatomy: a new concept of endodontic files and its implementation. J Endod 2010;36:679–90.
- Bürklein S, Tsotsis P, Schäfer E. Incidence of dentinal defects after root canal preparation: reciprocating versus rotary instrumentation. J Endod 2013;39:501–4.
- Liu R, Kaiwar A, Shemesh H, et al. Incidence of apical root cracks and apical dentinal detachments after canal preparation with hand and rotary files at different instrumentation lengths. J Endod 2013;39:129–32.
- Fedorov A, Beichel R, Kalpathy-Cramer J, et al. 3D Slicer as an image computing platform for the Quantitative Imaging Network. Magn Reson Imaging 2012;30: 1323–41.
- De-Deus G, Silva EJ, Marins J, et al. Lack of causal relationship between dentinal microcracks and root canal preparation with reciprocation systems. J Endod 2014;40:1447–50.
- De-Deus G, Belladonna FG, Souza EM, et al. Microcomputed tomographic assessment on the effect of ProTaper Next and Twisted File Adaptive systems on dentinal cracks. J Endod 2015;41:1116–9.
- Saber SE, Schäfer E. Incidence of dentinal defects after preparation of severely curved root canals using the Reciproc single-file system with and without prior creation of a glide path. Int Endod J 2016;49:1057–64.