
Shaping ability of single-file reciprocating and heat-treated multifile rotary systems: a micro-CT study
Abstract
Aim: To investigate changes in three-dimensional geometry, in various cross-sectional morphological parameters and in the centring ability of root canals prepared with different preparation systems using microcomputed tomographic imaging technology.
Methodology: Sixty-four mesial canals of mandibular molars were matched based on similar morphological dimensions using micro-CT evaluation and assigned to four experimental groups (n = 16), according to the canal preparation technique: Reciproc, WaveOne, Twisted File and HyFlex CM systems. Changes in several 2D (area, perimeter, form factor, roundness, minor and major diameter) and 3D [volume, surface area, structure model index (SMI)] morphological parameters, as well as canal transportation, were compared with pre-operative values using Kruskal–Wallis and ANOVA post hoc Tukey’s tests with the significance level set at 5%.
Results: Preparation significantly increased all tested parameters in the experimental groups. No significant differences were observed between groups regarding changes in volume, surface area, SMI, form factor and roundness of the root canal after preparation (P > 0.05). In the apical third, the Reciproc group had significantly greater changes in canal area, perimeter, major and minor diameters than the other groups (P < 0.05). Overall, the Twisted File and HyFlex CM systems were associated with significantly less transportation than the reciprocating instruments, Reciproc and WaveOne (P < 0.05).
Conclusions: Shaping procedures led to the enlargement of the root canal space with no evidence of significant preparation errors. Changes in 3D parameters were not different between groups whilst, in the apical third, Reciproc was associated with significantly greater changes in several 2D parameters compared to the other groups. Twisted File and HyFlex CM systems were able to maintain the original canal anatomy with less canal transportation than Reciproc and WaveOne; however, these differences are unlikely to be of clinical significance.
Introduction
Reports have demonstrated that reciprocating instruments decrease preparation time, increase cyclic fatigue life and have a shaping ability similar to that of conventional rotary systems (Berutti et al. 2012, De-Deus et al. 2013, Robinson et al. 2013). Proprietary thermomechanical processes have also resulted in the development of rotary NiTi systems with unique features (Gutmann & Gao 2012). The Twisted File system (SybronEndo, Orange, CA, USA) has been developed with three design features, namely R-phase heat treatment, twisting of the metal and special surface conditioning, which are claimed to enhance strength, flexibility and resistance to fatigue (Pedullà et al. 2013) and thus minimizing transportation even in severely curved root canals (Gergi et al. 2010, Capar et al. 2014, Ordinola-Zapata et al. 2014). The HyFlex CM system (Coltène–Whaledent, Altstätten, Switzerland) is manufactured using an innovative methodology to control the memory of the material (Saber et al. 2014). It has been claimed that it provides superior flexibility allowing better maintenance of the original canal curvature and increased efficiency and safety during canal preparation (Peterset al. 2012, Zhao et al. 2013).
Currently, very little information regarding the shaping ability of these new instruments in mandibular molars is available (Capar et al. 2014, Ordinola-Zapata et al. 2014, Saber et al. 2014). Thus, the purpose of this ex vivo study was to compare the shaping ability of single-file reciprocating (Reciproc and WaveOne) and heat-treated multifile rotary (Twisted File and HyFlex CM) systems on the preparation of moderately curved mesial root canals of mandibular molar teeth, using microcomputed tomography (micro-CT). The null hypothesis tested was that there are no differences in moderately curved root canals prepared with single-file reciprocating systems and heat-treated multifile rotary systems regarding changes in three-dimensional geometry, in cross-sectional morphological parameters and in centring ability.
Materials and methods
Specimen selection and preparation
Approval for the study protocol was obtained from the local ethics committee. From a pool of 250 mandibular molar teeth with fully formed apices, moderately curved mesial roots (10° to 20°) were selected by Schneider’s method (Schneider 1971) using digitized buccolingual radiographs and AxioVision 4.5 software (Carl Zeiss Vision GmbH, Hallbergmoos, Germany). The inclusion criteria comprised only molars with two independent canals in the mesial root in which the final apical gauging allowed a size 10 K-file (Dentsply Maillefer, Ballaigues, Switzerland) to be placed to working length (WL). Based on these criteria, 96 mandibular molars were selected.
After decoronation and resection of the distal root, the specimens were disinfected in 0.5% chloramine T and stored in distilled water at 4 °C. To attain an overall outline of root canal anatomy, each tooth was slightly dried, mounted on a custom attachment and pre-scanned in a relatively low isotropic resolution (70 μm) using a micro-CT scanner (SkyScan 1174v2; Bruker micro-CT, Kontich, Belgium) at 50 kV and 800 μA. Scanning was performed trough 180° rotation around the vertical axis with a rotation step of 1° using a 0.5-mm-thick aluminium filter. After the acquired projection images had been reconstructed into cross-section slices (NRecon v.1.6.9; Bruker micro-CT), 3D models and several morphological parameters of the mesial canals (length, volume and surface area) were obtained (CTAn v.1.14.4; Bruker micro-CT).
Based on the 3D models of this pre-scan set of images, 32 mesial roots of mandibular molars with a type IV Vertucci’s canal configuration system (64 canals) were selected. These roots were scanned again at an increased isotropic resolution of 19.6 μm, using 50 kV, 800 μA, 180° rotation around the vertical axis and rotation step of 0.7°. The projection images were then reconstructed (NRecon v.1.6.9; Bruker micro-CT) and the volume of interest selected extending from the furcation level to the apex of the root, resulting in the acquisition of approximately 650– 750 transverse cross sections per tooth. Subsequently, these 32 roots were matched to create eight groups of four based on the aforementioned morphological aspects of the root canals. One root from each group was randomly assigned to one of the four experimental groups (n = 16) and a flip of a coin was used to define which group would be treated with each of the following preparation techniques: Reciproc (VDW GmbH, Munich, Germany), WaveOne (Dentsply Maillefer), Twisted File (SybronEndo) and Hyflex CM (Coltène–Whaledent) systems. The number of samples per group (n = 16) was based on a previous publication (Gergi et al. 2014) in which a similar methodology was used to evaluate Reciproc, WaveOne and Twisted File Adaptive systems.
After checking the normality assumption (Shapiro–Wilk test), the degree of homogeneity (baseline) of the four groups with respect to the length, volume and surface area of the root canals was confirmed by one-way ANOVA test, with a significance level of 5%.
Root canal preparation
Root canals were accessed and the coronal third was flared with a number 1 LA Axxess Stainless Steel bur (SybronEndo) followed by irrigation with 5 mL 2.5% NaOCl. Patency was confirmed by inserting a size 10 K-file (Dentsply Maillefer) through the apical foramen, before and after completion of root canal preparation. For all groups, a glide path was created by scouting a stainless steel size 15 K-file (Dentsply Maillefer) up to WL, which was established 1 mm short of the apical foramen. In each group, instruments were driven with the VDW Silver motor (VDW GmbH), according to the manufacturers’ instructions, and a single experienced operator performed all preparations.
Reciproc R25 (size 25, .08 taper) and WaveOne Primary (size 25, .08 taper) were introduced into the canal until resistance was felt and then activated in reciprocating motion. The instruments were gently moved down until they reach the WL. Twisted File and HyFlex CM instruments were used in continuous clockwise rotation in a crown-down manner. In the Twisted File group, instrument size 25, .08 taper was used up to two-thirds of the root canal, followed by instrument size 25, .06 taper 2 mm short of the WL. Then, instruments sizes 25, .04 taper, 25, .06 taper and 25, .08 taper were taken to the WL. In the HyFlex CM group, instrument size 25, .08 taper was used until two-thirds of the root canal was shaped, followed by instruments sizes 20, .04 taper, 25, .04 taper, 20, .06 taper and 25, .08 taper up to the WL. In all groups, after three gentle in-and-out motion strokes in apical direction, the instrument was removed from the canal and cleaned, until the WL was reached. To avoid instrument fracture, each set of instruments was used to enlarge two canals only.
Between each preparation step, irrigation was performed with disposable syringes and 30-G NaviTip needles (Ultradent, South Jordan, UT, USA) taken up to 2 mm short of the WL, using a total of 20 mL of 2.5% NaOCl per canal. A final rinse with 5 mL 17% EDTA (pH = 7.7), delivered at a 1 mL min—1 rate for 5 min, followed by a 5-min 5-mL rinse with distilled water was performed. Then, canals were dried with absorbent paper points (Dentsply Maillefer), and the roots submitted to a postoperative micro-CT scan and reconstruction, applying the parameter settings mentioned previously.
3D and 2D imaging analysis
3D models of the root canals, before and after preparation, were reconstructed on the basis of micro-CT scans and coregistered using the rigid registration module of the 3D Slicer 4.3.1 free source software (available from http://www.slicer.org/). Colour-coded root canal models (green indicating preoperative and red postoperative canal surfaces) enabled qualitative comparison of the matched root canals before and after shaping using CTVol v.2.2.1 software (Bruker micro-CT). CTAn v.1.14.4 (Bruker micro-CT) was used for measuring volume, surface area, structure model index (SMI), area, perimeter, form factor, roundness, minor and major diameters of the root canals, before and after preparation. Detailed descriptions of the criteria used for the calculation of these parameters were published elsewhere (Peters et al. 2001a, Versiani et al. 2011, 2013a,b, Siqueira et al. 2013). Percentage median increase (%D) and interquartile range of each analysed parameter were calculated by subtracting the scores for the treated canals from those recorded for the untreated counterparts. 3D evaluation was performed for the full canal length, whilst 2D evaluation was undertaken for the apical 5 mm of the root canal in a total of 250 cross sections per canal.
Canal transportation
Canal transportation was assessed from centres of gravity that were calculated for each slice and connected along the z-axis with a fitted line in a total of 10 572 (Reciproc), 10 608 (WaveOne), 10 595 (Twisted File) and 10 583 (HyFlex CM) cross sections, using XLSTAT-3DPlot for Windows (Addinsoft, New York, NY, USA). Mean transportation (in mm) was then calculated by comparing the centres of gravity before and after treatment for the coronal, middle and apical thirds of the canals. Representative measurements were also graphically presented in diagrams.
Statistical analysis
The Shapiro–Wilk test was used to assess the normality of the data. Percentage median increase (%D) and interquartile range of the 3D and 2D parameters were compared between groups using Kruskal–Wallis test, whilst canal transportation was statistically evaluated with one-way ANOVA post hoc Tukey’s test (SPSS v17.0 for Windows; SPSS Inc., Chicago, IL, USA). Significance level was set at 5%.
Results
Canal preparation
Results of 3D and 2D analysis are detailed in Table 1. Preparation significantly increased all parameters in each experimental group. Comparison between systems revealed no significant difference between them regarding changes in the 3D parameters (volume, surface area and SMI) (P > 0.05) and in the cross-sectional appearance of the root canal after preparation (form factor and roundness) (P > 0.05). The Reciproc group had significantly greater changes in the area, perimeter, major and minor diameters of the apical canal than the other groups (P < 0.05), whilst the HyFlex CM system produced the least alteration in the major diameter, compared to the other systems (P < 0.05).
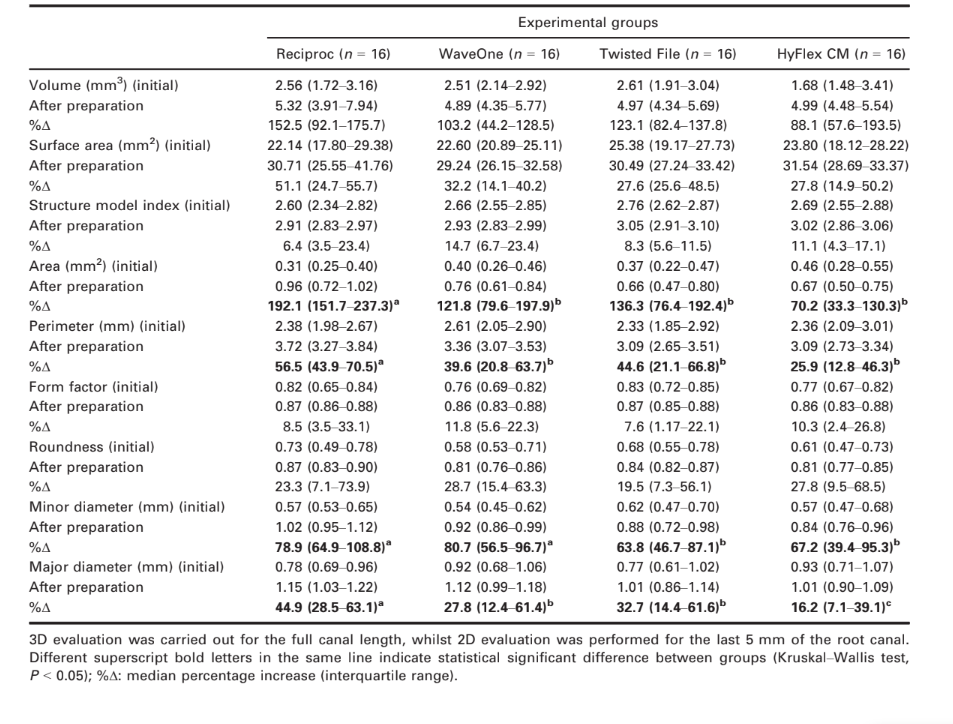
Preoperatively, canal cross sections were oval shaped (mean roundness of ~0.65 and form factor of ~0.85) and tapered (SMI of ~2.9) in all groups (Fig. 1a). After preparation, the outline of the canals was larger and showed a smooth taper in all experimental groups (Fig. 1b). Changes in canal shape, shown as superimpositions of unprepared (green) and prepared (red) areas, had untouched areas mainly on the internal aspect of the canals (Fig. 1b).

Canal transportation
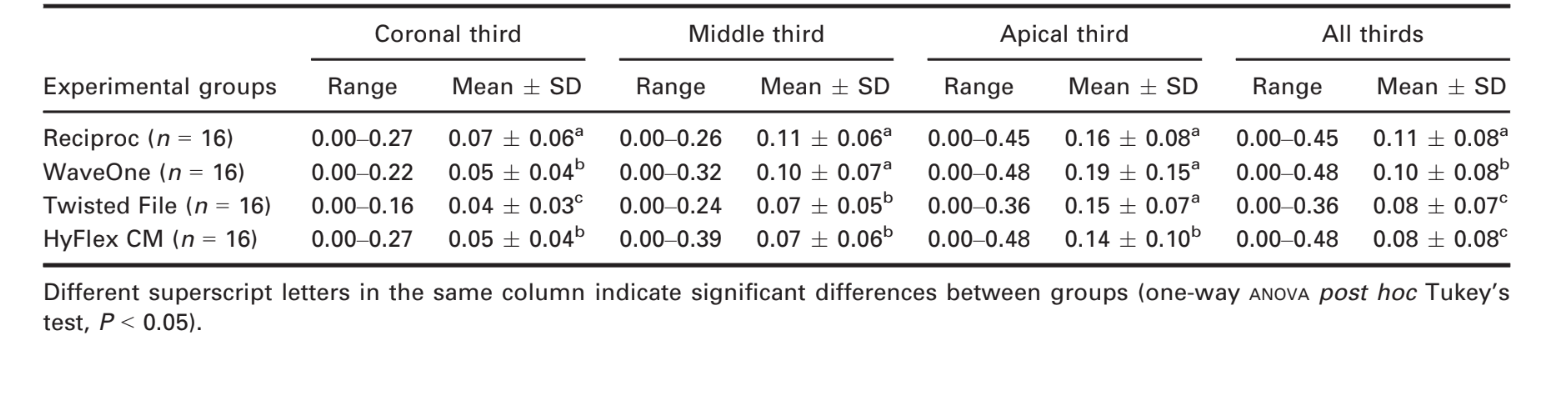
The results of canal transportation are summarized in Table 2 and Fig. 1(c,d). Overall, rotary systems (Twisted File and HyFlex CM) had significantly less transportation than reciprocating instruments (Reciproc and WaveOne) (P < 0.05). In the apical third, significantly less transportation was observed following use of HyFlex CM rather than other systems (P < 0.05).
Discussion
The present study compared the shaping ability of two single-file reciprocating (Reciproc and WaveOne) and two heat-treated multifile rotary (Twisted File and HyFlex CM) systems on the mesial root canals of mandibular molars using micro-CT technology.
Comparison between groups revealed no significant difference regarding changes in the 3D parameters of the canals after preparation, and the first null hypothesis tested was accepted. This result is not in accordance with a recent publication using similar methodology in which Reciproc and WaveOne systems yield higher changes in volume and surface area compared to the Twisted File Adaptive system (Gergi et al. 2014) and might be explained as the consequence of the similarity regarding the dimensions of the final instrument used in each group (size 25, .08 taper) and the sample distribution based on 3D morphological parameters of the root canal.
The main role of laboratory-based studies is to develop well-controlled conditions that are able to reliably compare certain factors (Versiani et al. 2013a). The main confounding factor of ex vivo studies is the anatomy of the root canal system under investigation. Consequently, the results might demonstrate the effect of canal anatomy rather than the variable of interest (De-Deus 2012). The influence of canal anatomy in the outcome of root canal preparation has also been emphasized by studies demonstrating that variations in canal geometry before shaping procedures had a greater effect on the changes that occurred during preparation than did the instrumentation techniques (Peters et al. 2001a,b). In recent years, micro-CT has gained increasing popularity in endodontics as it offers a reproducible technique that can be applied for the 3D assessment of the root canal system (Peters et al. 2001a, Versiani et al. 2011, Robinson et al. 2013). Consequently, this method might improve the matching of teeth to enhance the internal validity of ex vivo experiments. Thus, on the basis micro-CT data, it is be possible to further improve sample selection using established morphological parameters to provide a consistent baseline (Versianiet al. 2013a). In the present study, several attempts were made to create a reliable baseline to ensure the comparability of the groups by standardization of the 3D canal morphology of the sample, which was likely to eliminate potentially significant anatomical biases that could confound the results.
In this study, the 3D geometry and cross-sectional shape of the mesial canals were evaluated using three morphometric parameters: SMI, form factor and roundness, respectively. SMI involves a measurement of surface convexity in a three-dimensional structure. An ideal plate, cylinder and sphere have SMI values of 0, 3 and 4, respectively (Peters et al. 2001a).
Before preparation, SMI values (2.59–2.77) indicating a conical frustum-like geometry of the root canal system, which become more cylindrical after preparation (2.82–3.02). As it would be expected, form factor and roundness values indicated that the canals became more round after preparation. Interestingly, the similarity in the 3D geometry of the root canals before and after preparation was also reflected two-dimensionally, as no difference could be observed between groups regarding roundness and form factor in the apical third.
On the other hand, area, perimeter, minor and major diameters of the canals in the apical third were significantly different between the systems after the preparation procedures. Thus, the second null hypothesis was rejected. In infected root canals, the best treatment outcome is usually achieved when root canal infection is eradicated or reduced to levels compatible with periradicular healing (Siqueira et al. 2010). Consequently, it may be reasonable to assume that a larger preparation would allow for an improved disinfection (Hülsmann et al. 2005). Overall, the Reciproc group was associated with significant increases in the area, perimeter and major diameter of the canal compared to the other systems, which is in accordance with a previous study (Gergi et al. 2014). Dissimilarities in the cross-sectional design between the instruments may explain this difference. As previously stated, the cutting ability of an endodontic instrument is a result of the complex interrelationship of parameters such as the cross-sectional design, helical and rake angle, metallurgical proper- ties, surface treatment and movement kinematics (Capar et al. 2014). Reciproc has a double-cutting edge S-shaped geometry, which means sharp cutting edges and smaller cross-sectional area; combined with the reciprocating movement, the cutting efficiency of Reciproc is improved using a pecking motion (Giansiracusa Rubini et al. 2014), explaining its performance. Previous studies have demonstrated that the Twisted File and HyFlex CM instruments have an efficient cutting behaviour compared to other NiTi rotary systems when rotational speed is increased or when they were used in lateral action (Morgental et al. 2013, Peters et al. 2014). In the present study, the lowest values of the rotary systems regarding the 2D parameters may be related to the movement kinematic (pecking motion), the smaller tapered instruments reaching WL before instrument size 25, .08 taper and the occurrence of plastic deformation and disruption of cutting edges as a result of the proprietary heat treatment of the alloy.
The present results revealed that rotary systems (Twisted File and HyFlex CM) produced significantly less transportation than reciprocating systems (Reciproc and WaveOne), and the third null hypothesis was also rejected. This finding is corroborated by previous studies (Zhao et al. 2013, Bürklein et al. 2014) and can be attributed to the improved flexibility of the Twisted File and HyFlex CM (Saber et al. 2014), as a result of the thermal pre-treatment of the alloy during manufacturing which makes it more ductile, reducing the magnitude of the restoring forces (Pongione et al. 2012, Saber et al. 2014). Although significant differences regarding canal transportation were obtained, the clinical relevance of the means achieved by rotary (0.08 mm) and reciprocating (0.10–0.11 mm) instruments remains questionable (Hülsmann et al. 2005, Saber et al. 2014) and probably have a limited importance in these moderately curved canals. Thus, it may be assumed that all instruments maintained the original canal curvature well.
Conclusion
Within the limitations of this ex vivo study, it can be concluded that none of the NiTi systems was able to prepare the entire walls of the root canal system. Overall, shaping procedures led to the enlargement of the root canal space with no evidence of significant preparation errors. Changes in 3D parameters were not different between groups whilst, in the apical third, Reciproc was associated with significantly higher changes in several 2D parameters (area, perimeter, major and minor diameters) when compared to the other groups. Twisted File and HyFlex CM systems were able to maintain the original canal anatomy with less canal transportation and better centring ability than Reciproc and WaveOne; however, these differences are unlikely to be of clinical significance.
Authors: M. F. V. Marceliano-Alves, M. D. Sousa-Neto, S. R. Fidel, L. Steier, J. P. Robinson, J. D. Pécora2, M. A. Versiani
References:
- Berutti E, Chiandussi G, Paolino DS et al. (2012) Canal shaping with WaveOne Primary reciprocating files and ProTaper system: a comparative study. Journal of Endodontics 38, 505–9.
- Bürklein S, Borjes L, Schäfer E (2014) Comparison of preparation of curved root canals with Hyflex CM and Revo-S rotary nickel-titanium instruments. International Endodontic Journal 47, 470–6.
- Capar ID, Ertas H, Ok E, Arslan H, Ertas ET (2014) Comparative study of different novel nickel-titanium rotary systems for root canal preparation in severely curved root canals. Journal of Endodontics 40, 852–6.
- De-Deus G (2012) Research that matters – root canal filling and leakage studies. International Endodontic Journal 45, 1063–4.
- De-Deus G, Arruda TE, Souza EM et al. (2013) The ability of the Reciproc R25 instrument to reach the full root canal working length without a glide path. International Endodontic Journal 46, 993–8.
- Gergi R, Rjeily JA, Sader J, Naaman A (2010) Comparison of canal transportation and centering ability of twisted files, Pathfile-ProTaper system, and stainless steel hand K-files by using computed tomography. Journal of Endodontics 36, 904–7.
- Gergi R, Osta N, Bourbouze G, Zgheib C, Arbab-Chirani R, Naaman A (2014) Effects of three nickel titanium instrument systems on root canal geometry assessed by micro- computed tomography. International Endodontic Journal, doi: 10.1111/iej.12296 [Epub ahead of print].
- Giansiracusa Rubini A, Plotino G, Al-Sudani D et al. (2014) A new device to test cutting efficiency of mechanical endodontic instruments. Medical Science Monitor 20, 374–8.
- Gutmann JL, Gao Y (2012) Alteration in the inherent metallic and surface properties of nickel-titanium root canal instruments to enhance performance, durability and safety: a focused review. International Endodontic Journal 45, 113–28.
- Hülsmann M, Peters OA, Dummer PMH (2005) Mechanical preparation of root canals: shaping goals, techniques and means. Endodontic Topics 10, 30–76.
- Morgental RD, Vier-Pelisser FV, Kopper PM, de Figueiredo JA, Peters OA (2013) Cutting efficiency of conventional and martensitic nickel-titanium instruments for coronal flaring. Journal of Endodontics 39, 1634–8.
- Ordinola-Zapata R, Bramante CM, Duarte MA, Cavenago BC, Jaramillo D, Versiani MA (2014) Shaping ability of reciproc and TF adaptive systems in severely curved canals of rapid microCT-based prototyping molar replicas. Journal of Applied Oral Science, doi: 10.1590/678-775720130705 [Epub ahead of print].
- Pedullà E, Grande NM, Plotino G, Gambarini G, Rapisarda E (2013) Influence of continuous or reciprocating motion on cyclic fatigue resistance of 4 different nickel-titanium rotary instruments. Journal of Endodontics 39, 258–61.
- Peters OA, Laib A, Gohring TN, Barbakow F (2001a) Changes in root canal geometry after preparation assessed by high-resolution computed tomography. Journal of Endodontics 27, 1–6.
- Peters OA, Schönenberger K, Laib A (2001b) Effects of four Ni-Ti preparation techniques on root canal geometry assessed by micro computed tomography. International Endodontic Journal 34, 221–30.
- Peters OA, Gluskin AK, Weiss RA, Han JT (2012) An in vitro assessment of the physical properties of novel Hyflex nickel-titanium rotary instruments. International Endodontic Journal 45, 1027–34.
- Peters OA, Morgental RD, Schulze KA, Paque F, Kopper PM, Vier-Pelisser FV (2014) Determining cutting efficiency of nickel-titanium coronal flaring instruments used in lateral action. International Endodontic Journal 47, 505–13.
- Pongione G, Pompa G, Milana V et al. (2012) Flexibility and resistance to cyclic fatigue of endodontic instruments made with different nickel-titanium alloys: a comparative test. Annali di Stomatologia 3, 119–22.
- Robinson JP, Lumley PJ, Cooper PR, Grover LM, Walmsley AD (2013) Reciprocating root canal technique induces greater debris accumulation than a continuous rotary technique as assessed by 3-dimensional micro-computed tomography. Journal of Endodontics 39, 1067–70.
- Saber SE, Nagy MM, Schäfer E (2014) Comparative evaluation of the shaping ability of ProTaper Next, iRaCe and Hyflex CM rotary NiTi files in severely curved root canals. International Endodontic Journal, doi: 10.1111/iej.12291 [Epub ahead of print].
- Schneider SW (1971) A comparison of canal preparations in straight and curved root canals. Oral Surgery, Oral Medicine, and Oral Pathology 32, 271–5.
- Siqueira JF Jr, Alves FR, Almeida BM, de Oliveira JC, Roças IN (2010) Ability of chemomechanical preparation with either rotary instruments or self-adjusting file to disinfect oval-shaped root canals. Journal of Endodontics 36, 1860–5.
- Siqueira JF Jr, Alves FRF, Versiani MA et al. (2013) Correlative bacteriologic and micro–computed tomographic analysis of mandibular molar mesial canals prepared by Self-Adjusting File, Reciproc, and Twisted File systems. Journal of Endodontics 39, 1044–50.
- Versiani MA, Pécora JD, Sousa-Neto MD (2011) Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. Journal of Endodontics 37, 1002–7.
- Versiani MA, Pécora JD, Sousa-Neto MD (2013a) Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. International Endodontic Journal 46, 800–7.
- Versiani MA, Steier L, De-Deus G, Tassani S, Pécora JD, Sousa-Neto MD (2013b) Micro–computed tomography study of oval-shaped canals prepared with the Self-adjusting File, Reciproc, WaveOne, and Protaper Universal systems. Journal of Endodontics 39, 1060–6.
- Zhao D, Shen Y, Peng B, Haapasalo M (2013) Micro-computed tomography evaluation of the preparation of mesiobuccal root canals in maxillary first molars with Hyflex CM, Twisted Files, and K3 instruments. Journal of Endodontics 39, 385–8.