Micro–computed Tomographic Analysis of the Root Canal Morphology of Mandibular Incisors
Abstract
Introduction: This study aimed to describe the anatomy of mandibular central and lateral incisors using micro–computed tomographic imaging.
Methods: One hundred mandibular incisors were scanned in a micro– computed tomographic device using an isotropic resolution of 22.9 mm. The anatomy of each tooth (length of the roots, presence and location of accessory canals and apical deltas, and number of canals) as well as the 2- and 3-dimensional morphologic aspects of the canal (area, roundness, diameter, volume, surface area, and structure model index) were evaluated. Data were statistically compared using the Student t test (alpha = 0.05).
Results: The mean lengths of the mandibular central and lateral incisors were 20.71 and 21.56 mm, respectively. Most of the central (60%) and lateral (74%) incisors had no accessory canals. An apical delta was observed in only 1 specimen. The cross-section analysis of the apical third showed the presence of 1, 2, or 3 canal orifices. No statistical difference was observed in the comparison of the 2- and 3-dimensional morphologic parameters between central and lateral incisors (P < .05). The qualitative analyses of the 3-dimensional models of the root canal systems of the central and lateral incisor teeth confirm that the most prevalent configurations were Vertucci’s types I (50% and 62%, respectively) and III (28%).
Conclusions: Overall, mandibular central and lateral incisors were similar in terms of the 2- and 3-dimensional analyzed parameters. Vertucci’s types I and III were the most prevalent canal configurations of the mandibular incisors; however, 8 new types have also been described. (J Endod 2013;■:1–7)
The ultimate goal of chemomechanical preparation is to remove the inner layer of the dentin while allowing the irrigant to reach the entire length of the root canal, eradicating bacterial populations or at least reducing them to levels that are compatible with periradicular tissue healing. Unfortunately, canal preparation results are adversely affected by the highly variable root canal anatomy. The presence of additional canals or deviations of the main root canals need to be recognized in order to avoid incomplete instrumentation and the maintenance of etiologic factors involved in apical periodontitis. Therefore, the knowledge of root canal anatomy and its variations is a prerequisite for successful endodontic treatment.
Usually, teeth with single roots present single canals as in mandibular and maxillary anterior teeth. However, particular tooth types, such as mandibular premolars and incisors, are recognized as exhibiting a distinct range of variations in the morphology of their root canal system. In mandibular incisors, often a dentinal bridge is present in the pulp chamber dividing the root into 2 canals. The 2 canals usually join and exit through a single apical foramen, but they may persist as 2 separate canals. On occasion, 1 canal branches into 2 canals, which subsequently rejoin into a single canal before reaching the apex.
The incidence of 2 canals in mandibular incisors has been reported to be as low as 0.3% and as high as 45.3%. The wide range of variation reported in the literature regarding the prevalence of a second canal in mandibular incisors has been related mostly to methodologic and racial differences. In recent years, micro–computed tomographic (micro-CT) imaging has gained increasing significance in the study of hard tissues in endodontics. This technology offers a reproducible technique that can be applied quantitatively as well as qualitatively for the 3-dimensional assessment of the root canal system. To date, the literature lacks a detailed description of the anatomic variation of mandibular incisors using micro-CT technology. Thus, the aim of this study was to describe the morphometric aspects of the internal anatomy of mandibular central and lateral incisors using micro-CT imaging.
Materials and Methods
A total of 612 extracted single-rooted human mandibular incisors collected from the Brazilian population were available for this study. Patient sex and age were unknown. Before sample selection, each tooth was cleaned and examined under magnification (×3.5). The exclusion criteria included teeth in which the presence of caries, attrition, or fractured disrupted the characteristic outline of the tooth needed to differentiate the central from the lateral mandibular incisor or would impair later measurements. By applying such criteria, the initial sample was reduced to 234 teeth. To be accepted as central or lateral incisors for this investigation, agreement among 3 of the authors was necessary. Thus, a further 134 teeth were discarded, and the final sample comprised 50 central and 50 lateral incisors (N = 100) with fully formed apices, which were stored in labeled individual plastic vials containing 0.1% thymol solution. After ethics committee approval (Protocol # 0072.0.138.000-09), the specimens were washed in running water for 24 hours, mounted on a custom attachment, and scanned in a micro-CT system (SkyScan 1174v2; Bruker-microCT, Kontich, Belgium) using 50 kV, 800 mA, and an isotropic resolution of 22.9 mm. Images of each specimen were reconstructed from the apex to the level of the cementoenamel junction with dedicated software (NRecon v.1.6.3, Bruker-microCT), providing axial cross-sections of the inner structure of the samples. DataViewer v.1.4.4 software (Bruker-microCT) was used to evaluate the length of the teeth, the presence and location of accessory canals, and the number of canal orifices at 5 different levels in the apical third. CTAn v.2.2.1 software (Bruker-microCT) was used for the 3-dimensional evaluation of the root canal (volume, surface area, and structure model index) from the apex to the cementoenamel junction. Two-dimensional evaluation (area, roundness, major diameter, and minor diameter) of the canal in the apical third at every 1-mm interval from the main apical foramen was also performed.
Volume was calculated as the volume of binarized objects within the volume of interest. For the measurement of the surface area of the 3-dimensional multilayer data set, 2 components to the surface measured in a 2-dimensional plane were used: the perimeters of the binarized objects on each cross-sectional level and the vertical surfaces exposed by pixel differences between adjacent cross-sections. The structure model index (SMI) involves a measurement of surface convexity in a 3-dimensional structure. SMI is derived as 6.([S’.V]/S2), where S is the object surface area before dilation, and S’ is the change in surface area caused by dilation. V is the initial, undilated object volume. An ideal plate, cylinder, and sphere have SMI values of 0, 3, and 4, respectively. Area was calculated using the Pratt algorithm. The cross-sectional appearance, round or more ribbon shaped, was expressed as roundness. The roundness of a discreet 2-dimensional object is defined as 4.A/(p.[dmax]2), where ‘‘A’’ is the area and ‘‘dmax’’ is the major diameter. The value of roundness ranges from 0–1, with 1 signifying a circle. The major diameter is defined as the distance between the 2 most distant pixels in the object, and the minor diameter is the longest chord through the object that can be drawn in the direction orthogonal to that of the major diameter.
Three-dimensional models were reconstructed from the source images by using automatic segmentation and surface modeling with CTAn v.2.2.1 software. CTVol v.2.4 software (Bruker-microCT) was used for visualization and qualitative evaluation of the specimens regarding the root canal configuration according to Vertucci’s configuration system.
Because normality assumptions could be verified (Shapiro-Wilk test, P > .05), the results of the 2- and 3-dimensional analyses of the central and lateral mandibular incisors, described as mean and standard deviation, were statistically compared using the Student t test (SPSS v17.0; SPSS Inc, Chicago, IL) with a significance level set at 5%.
Results
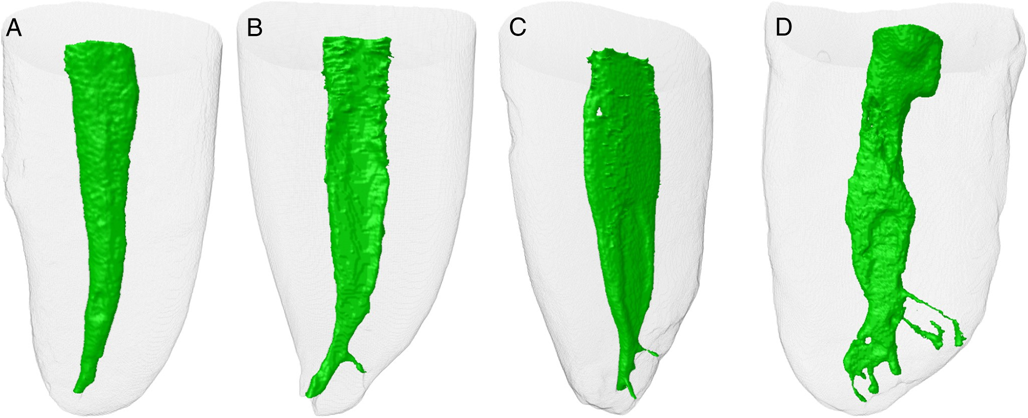
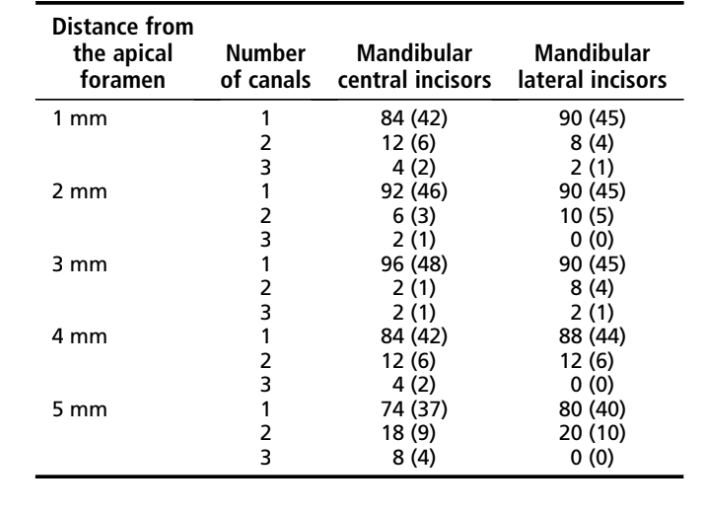
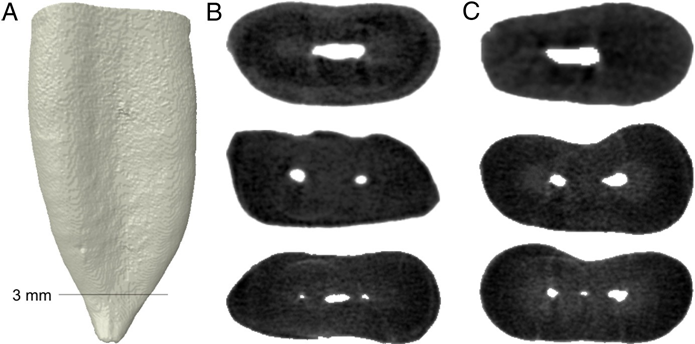
The length of the central and lateral mandibular incisors, measured from the apex to the incisal edge, ranged from 16.01 to 27.18 mm (20.71 1.69 mm) and from 17.45 to 28.38 mm (21.56 1.82 mm), respectively, with no significant statistical difference between them (P > .05). Accessory canals were observed only at the apical third; however, most of the central (n = 30, 60%) and lateral (n = 37, 74%) incisors had no accessory canals (Fig. 1A). In 38% (n = 19) and 26% (n = 13) of the central and lateral incisors, respectively. The number of accessory canals ranged from 1–2 (Fig. 1B and C). An apical delta was observed in only 1 central incisor (2%) (Fig. 1D). The cross-section analysis of the apical third showed that most of the samples had just 1 canal; however, in a few specimens, 2 separate canals were observed in all analyzed levels. Three root canals were present mostly in the apical third of the mandibular central incisor (Table 1 and Fig. 2A–C).
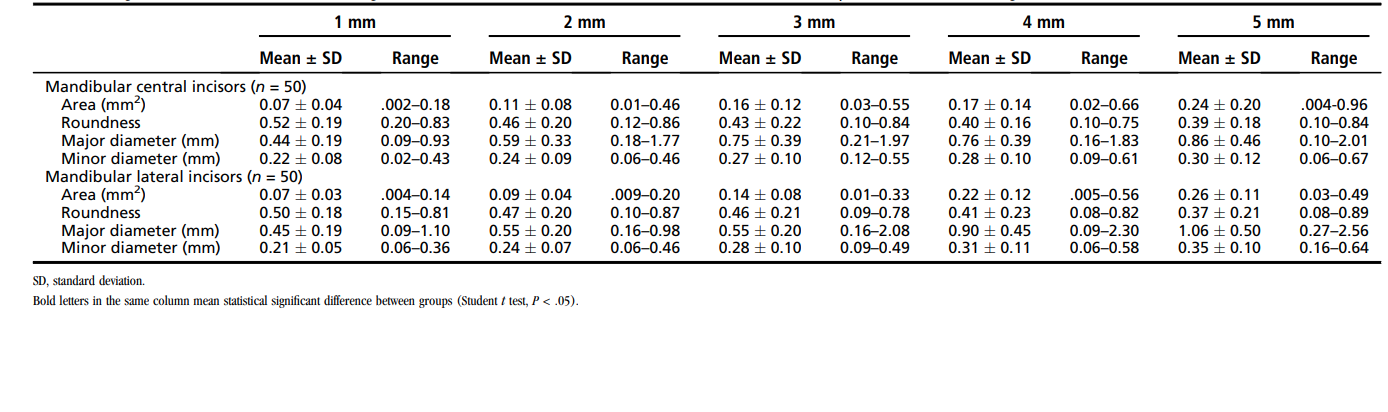
No statistical difference was observed in the comparison of volume, surface area, and SMI values between central (4.38 1.97 mm3, 36.17 10.55 mm2, and 2.16 0.36, respectively) and lateral (4.74 1.33 mm3, 39.76 7.38 mm2, and 2.09 0.44, respectively) incisors, respectively (P > .05). The results of the 2-dimensional morphometric analysis of the root canal at the apical third are detailed in Table 2. The area of the root canal in both teeth increased gradually in the coronal direction. Canal shapes (roundness) did not remain constant from 1 level to the next. Overall, the average roundness ranging from 0.37 0.21 to 0.52 0.19 represents a flat- or oval-shaped configuration of the canal in the apical third of both groups of teeth. The analysis of the external anatomy of the specimens showed that the presence of grooves in the proximal aspects of the root reflected the cross-section configuration of the root canal. No statistical difference was found in the comparison of area, roundness, and minor diameter values at all analyzed levels of the main root canal (P > .05). On average, the major diameter was twice the length of the minor diameter. The latter was generally the narrowest dimension of the canal in all levels. However, a significant statistical difference between central and lateral incisors was observed regarding the major diameter of the canal at 3 and 5 mm from the apical foramen (P < .05). The major diameter of the root canal at the 5-mm level also showed an increase of 95.45% and 135.55% in comparison with the 1-mm level in the central and lateral incisor teeth, respectively.
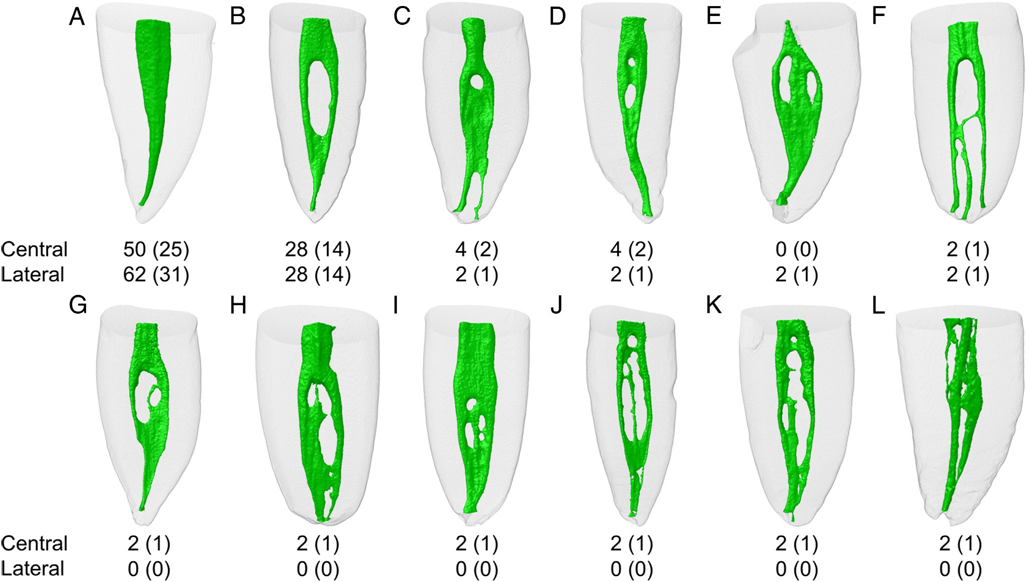
The qualitative analyses of the 3-dimensional models of the root canal system of the central and lateral incisor teeth confirm that the most prevalent configurations were Vertucci’s types I (50% and 62%, respectively) (Fig. 3A) and III (28%) (Fig. 3B) as well as the configuration type VII (Fig. 3C) and its variation (Fig. 3D). Eight new root canal configurations were encountered in the present study (Figs. 3E–L) that are not included in the classic Vertucci’s configuration system. Percentage frequency distribution of the morphologic configuration of the root canal system in the mandibular incisors is summarized in Table 3.

Discussion
The external morphology of mandibular central and lateral incisors has been considered to be similar by many authors. Usually, mandibular incisors have a single root, which is narrower mesiodistally than buccolingually and tapers toward the apex.
Despite the fact that the mandibular lateral incisor resembles the mandibular central incisor, on average, it used to be wider and longer. Woelfel and Scheid reported an average size of 20.8 mm (ranging from 16.9–26.7 mm) and 22.1 mm (ranging from 18.5–26.6 mm) for 226 mandibular central and 234 mandibular lateral incisors, respectively, which is in accordance with the present results.
An accessory canal has been defined as any branch of the main pulp canal or chamber that communicates with the external surface of the root, whereas an apical delta is the presence of multiple accessory canals at or near the apex. They serve as avenues for the passage of irritants primarily from the pulp to the periodontium. In the present study, an apical delta was observed in only 1 central incisor, whereas all accessory canals were located in the apical third. In previous studies, accessory canals in the mandibular central and lateral incisors were observed in 3.2% and 3.9%, 10.3% and 3.8%, and 24% and 26% of the samples. Despite the fact that some authors observed no apical delta in these groups of teeth, its incidence has been reported as being 5.9% and 19.4% and 29.5% and 19.5% in the mandibular central and lateral incisors, respectively. Such differences could be explained through diversity in the sample origin or racial factors as well as the evaluation methods. However, these results confirm the evidence that in mandibular incisors accessory canals are usually located in the apical third.
If surgery becomes necessary, the natural anatomy is altered, and additional anatomic features need to be addressed. Results will be poor if this altered anatomy is not recognized and treated properly. Considering that, in mandibular incisors, most of the accessory canals were observed in the apical third; beveling the root apex 3 mm during surgical procedures may remove the vast majority of unprepared and unfilled accessory canals and thereby eliminate the possibility of failure. However, in a surgical procedure, an undebrided isthmus can become exposed, and a single foramen may become multiple foramina. Despite the fact that canals are generally more ribbon or long oval shaped in the coronal levels and become round or oval 1 mm from the apical foramen, it is interesting to note that the canal number and shape did not always remain constant in the apical third. Thus, in this case, surgical microscopy and ultrasonic root-end preparation would help the clinician to better visualize the apex, incorporating both canals and the isthmus into the root-end preparation to ensure complete debridement and sealing of the root canal system.
Similarities among mandibular central and lateral incisors are not just related to the external anatomy. Actually, 2 and 3-dimensional analyses of the root canal system showed that both teeth present analogous features. Unlike previous studies using clearing, sectioning, modeling, or radiographic methods, algorithms used in micro-CT evaluation allow further measurement of basic geometric parameters such as volume and surface area as well as additional descriptors of canal shape such as SMI. The SMI is determined by an infinitesimal enlargement of the surface, whereas the change in volume is related to changes of surface area (ie, convexity of the structure). This 3-dimensional parameter involves the measurement of the surface convex curvature allowing objective quantification of how ‘‘rod-like’’ or ‘‘plate-like’’ the object is. A 3-dimensional data set was used to create a smooth model of the root canal. Using this model, the surface area and volume were used to calculate the SMI. An object consisting purely of plates would have an SMI of 0, and an object consisting purely of rods would have an SMI of 3. Objects containing a mixture of elements would have intermediate values. In summary, if a perfect plate is enlarged, the surface area does not change, yielding an SMI of 0. However, if a rod is expanded, the surface area increases with the volume, and the SMI is normed, so that perfect rods are assigned an SMI score of 3. In the present study, the SMI results indicated that the root canal system of the central (ranging from 1.42–2.99) and lateral (ranging from 1.4–3.06) incisors varied from a flat- or oval-shaped to a cylinder-shaped geometry.
The results of volume and surface area cannot be compared because there is no information on this subject in the literature regarding the mandibular incisors, although they are 70% and 50% lower than in the mandibular canines, respectively. In infected root canals, it is possible that this small volume and surface area contribute to a rapid loss of effectiveness of the irrigant solution during the shaping procedures. In such situations, a continuous irrigation with fresh solution is recommended. Besides, it would be advisable to perform a high-volume flush of the irrigant solution after the shaping procedure has been completed.
Effective root canal debridement relies on accurate determination of the working length and adequate apical canal enlargement, which allow for a better irrigation in the apical area, optimizing root canal disinfection. A previous study on mandibular incisors reported a canal diameter ranging from 0.13–0.80 mm (major diameter) and from 0.12–0.33 mm (minor diameter) 1 mm short of the apical foramen. Despite differences in the methodologic approach, these results were quite similar to the present ones. Considering all analyzed samples, the major and minor diameters of the root canal at this level ranged from 0.09–1.10 mm and from 0.02–0.43 mm, respectively. Miyashita et al have observed that in 4.6% of their sample (n = 50), the major diameter of the canal in the apical third was above 0.7 mm, whereas Mauger et al found an average canal diameter of 0.49 mm (ranging from 0.18–1.49) at this level. These large variations are consistent with the roundness values that ranged from 0.15–0.83, which means that the canal cross-section varied from ribbon to a more round shape. These data also indicated that, in some cases, the mechanical debridement at the apical level could only be improved with instruments up to an ISO size 100 in order to avoid leaving untouched fins on the buccal and/or lingual aspects of the central canal area. However, considering that the mandibular incisors have a flat root with the narrowest diameter in the mesiodistal direction, using instruments with large tip or taper could lead to stripping or perforation of the root. It stresses the use of additional disinfection supplements such as passive ultrasonic irrigation or negative apical pressure in order to improve apical debridement.
Many methods have been successfully used for many years to investigate the internal morphology of mandibular incisors; however, some inherent repeatedly discussed limitations have encouraged the search for new methods that are able to produce improved results. The difference in the findings of previous studies may be related to the limitations of each method and the individual variation of root canals. In vivo and ex vivo studies on mandibular incisors using radiographic methods allowed only a 2-dimensional evaluation of the complexity of the root canal system. In this way, the results were limited to the number of canals and the presence of a common or separated apical exit. This method does not allow one to determine if a wall of dentin separates 2 distinct canals or if the 2 canals are connected by an isthmus of pulp tissue, which could be achieved by sectioning the specimens. However, sectioning techniques cause the destruction of the specimens as well as important anatomic details limiting the analysis to just a few sections of the root canal. Thus, using conventional methods, fine details of the root canal system may be lost during the sample preparation. To overcome the limitations of the aforementioned 2-dimensional methods, the clearing technique has been used in the study of the internal anatomy of mandibular incisor teeth. The main advantages of this method are that it is inexpensive, does not require complex laboratory equipment, and allows a thorough examination of the root canal system. Conversely, the tooth is irreversibly altered because of its dissolution and the injection of dye. In addition, the ink may penetrate in areas with great dentine permeability and distort the appearance of the original root canal. In contrast, the injected material may not flow adequately into all canal ramifications, resulting in an inaccurate image of the pulp canal space. Thus, in the present study, extracted mandibular incisors were examined using a device that provides 3-dimensional and detailed views of the tooth without the need of sectioning, preparation, or destruction of the specimens.
In 1974, using cleared teeth, Vertucci was able to identify 8 different pulp space configurations. Taken together, only a few studies on mandibular incisors attempted to evaluate the morphology of the root canal using this configuration system as in the present study. Table 3 summarizes the main findings of these studies. Overall, the most prevalent canal configurations of both mandibular central and lateral canals were types I and III. Nonetheless, despite the small percentage of the sample, plenty of different configuration systems have also been reported (Table 3). This lack of consistency in the reported prevalence of different morphologic root canal systems of the mandibular incisors is probably related to the methodology involved, sample selection, study design (in vivo vs ex vivo), racial divergence, or even the varying interpretation of canal configuration by the different investigators.
Although the presence of different root canal configurations in mandibular incisors has been rarely reported in comparison with the classic Vertucci’s configuration system, clinicians must be aware of these anatomic variations. Clinically, radiographs have been one of the most important tools for detecting anatomic variations of the teeth. Unfortunately, double root canals in lower mandibular incisors are rarely apparent on clinical radiographs, and routine endodontic procedures from the lingual approach fail to reveal the presence of the second canal.
Therefore, other diagnostic methods like spiral and cone-beam computed tomographic imaging as well as the use of a surgical operative microscope could be useful in such conditions, supporting clinicians during the diagnosis and treatment of mandibular incisors. In summary, the reported data may help clinicians understand the variations in root canal morphology of mandibular incisors in order to overcome problems associated with shaping and cleaning procedures.
Conclusions
Overall, mandibular central and lateral incisors were similar in terms of the 2- and 3-dimensional analyzed parameters. Vertucci’s types I and III were the most prevalent canal configurations observed in the mandibular incisors; however, 8 new types have also been described.
Authors: Graziela Bianchi Leoni, Marco Aurélio Versiani, Jesus Djalma Pécora, Manoel Damião de Sousa-Neto
References:
- Siqueira JF Jr, Alves FRF, Versiani MA, et al. Correlative bacteriologic and micro– computed tomographic analysis of mandibular molar mesial canals prepared by Self-Adjusting File, Reciproc, and Twisted File systems. J Endod 2013;39:1044–50.
- Siqueira JF Jr. Reaction of periradicular tissues to root canal treatment: benefits and drawbacks. Endod Top 2005;10:123–47.
- Peters OA, Laib A, Gohring TN, et al. Changes in root canal geometry after preparation assessed by high-resolution computed tomography. J Endod 2001;27:1–6.
- Versiani MA, Pécora JD, Sousa Neto MD. Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. Int Endod J 2013;46: 800–7.
- Versiani MA, Pécora JD, Sousa-Neto MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37: 1002–7.
- Vertucci FJ. Root canal morphology and its relationship to endodontic procedures. Endod Top 2005;10:3–29.
- Vertucci FJ. Root canal anatomy of the mandibular anterior teeth. J Am Dent Assoc 1974;89:369–71.
- Mauger MJ, Schindler WG, Walker WA 3rd. An evaluation of canal morphology at different levels of root resection in mandibular incisors. J Endod 1998;24:607–9.
- Gomes BP, Rodrigues HH, Tancredo N. The use of a modelling technique to investigate the root canal morphology of mandibular incisors. Int Endod J 1996;29:29–36.
- Kartal N, Yanikoglu FC. Root canal morphology of mandibular incisors. J Endod 1992;18:562–4.
- Nattress BR, Martin DM. Predictability of radiographic diagnosis of variations in root canal anatomy in mandibular incisor and premolar teeth. Int Endod J 1991;24: 58–62.
- Walker RT. The root canal anatomy of mandibular incisors in a southern Chinese population. Int Endod J 1988;21:218–23.
- Kaffe I, Kaufman A, Littner MM, et al. Radiographic study of the root canal system of mandibular anterior teeth. Int Endod J 1985;18:253–9.
- Benjamin KA, Dowson J. Incidence of two root canals in human mandibular incisor teeth. Oral Surg Oral Med Oral Pathol 1974;38:122–6.
- Madeira MC, Hetem S. Incidence of bifurcations in mandibular incisors. Oral Surg Oral Med Oral Pathol 1973;36:589–91.
- Green D. Double canals in single roots. Oral Surg Oral Med Oral Pathol 1973;35: 689–96.
- Pineda F, Kuttler Y. Mesiodistal and buccolingual roentgenographic investigation of 7,275 root canals. Oral Surg Oral Med Oral Pathol 1972;33:101–10.
- Laws AJ. Prevalence of canal irregularities in mandibular incisors: a radiographic study. N Z Dent J 1971;67:181–6.
- Rankine-Wilson RW, Henry P. The bifurcated root canal in lower anterior teeth. J Am Dent Assoc 1965;70:1162–5.
- Miyashita M, Kasahara E, Yasuda E, et al. Root canal system of the mandibular incisor. J Endod 1997;23:479–84.
- Hargreaves KM, Cohen S. Cohen’s Pathways of the Pulp, 10th ed. St Louis: Mosby; 2011.
- Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 2004;30: 391–8.
- Sert S, Aslanalp V, Tanalp J. Investigation of the root canal configurations of mandibular permanent teeth in the Turkish population. Int Endod J 2004;37:494–9.
- Neo J, Chee LF. A retrospective clinical study of endodontically treated mandibular incisors in a selected Chinese population. Oral Surg Oral Med Oral Pathol 1990;70:782–3.
- Bellizzi R, Hartwell G. Clinical investigation of in vivo endodontically treated mandibular anterior teeth. J Endod 1983;9:246–8.
- Versiani MA, Steier L, De-Deus G, et al. Micro–computed tomography study of oval-shaped canals prepared with the Self-adjusting File, Reciproc, WaveOne, and Protaper Universal systems. J Endod 2013;39:1060–6.
- Versiani MA, Pécora JD, Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars: a micro-computed tomography study. J Endod 2012;38:977–82.
- Peters OA, Laib A, Ruegsegger P, et al. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res 2000;79:1405–9.
- De Deus QD. Frequency, location, and direction of the lateral, secondary, and accessory canals. J Endod 1975;1:361–6.
- Woelfel JB, Scheid RC. Dental Anatomy: Its Relevance to Dentistry, 6th ed. Philadelphia: Lippincott Williams & Wilkins; 2002.
- Wu MK, R’Oris A, Barkis D, et al. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:739–43.
- Haapasalo M, Shen Y, Qian W, et al. Irrigation in endodontics. Dent Clin North Am 2010;54:291–312.
- Fornari VJ, Silva-Sousa YT, Vanni JR, et al. Histological evaluation of the effectiveness of increased apical enlargement for cleaning the apical third of curved canals. Int Endod J 2010;43:988–94.
- Neelakantan P, Subbarao C, Subbarao CV. Comparative evaluation of modified canal staining and clearing technique, cone-beam computed tomography, peripheral quantitative computed tomography, spiral computed tomography, and plain and contrast medium-enhanced digital radiography in studying root canal morphology. J Endod 2010;36:1547–51.
- Klein RM, Blake SA, Nattress BR, et al. Evaluation of X-ray beam angulation for successful twin canal identification in mandibular incisors. Int Endod J 1997;30:58–63.