
Morphologic Micro–Computed Tomography Analysis of Mandibular Premolars with Three Root Canals
Abstract
Introduction: This study aimed to describe the anatomy of mandibular premolars with type IX canal configuration by using micro–computed tomography.
Methods: Mandibular premolars with radicular grooves (n = 105) were scanned, and 16 teeth with type IX configuration were selected. Number and location of canals, distances between anatomic landmarks, occurrence of apical delta, root canal fusion, and furcation canals, as well as 2-dimensional (area, perimeter, roundness, major and minor diameters) and 3-dimensional (volume, surface area, and structure model index) analysis were performed. Data were statistically compared by using analysis of variance and Kruskal-Wallis tests (α = 0.05).
Results: Overall, specimens had 1 root with a main canal that divided into mesiobuccal, distobuccal, and lingual canals at the furcation level. Mean length of the teeth was 22.9 ± 2.06 mm, and the configuration of the pulp chamber was mostly triangle-shaped. Mean distances from the furcation to the apex and cementoenamel junction were 9.14 ± 2.07 and 5.59 ± 2.19 mm, respectively. Apical delta, root canal fusion, and furcation canals were present in 4, 5, and 10 specimens, respectively. No statistical differences were found in the 2-dimensional and 3-dimensional analyses between root canals (P > .05).
Conclusions: Type IX configuration of the root canal system was found in 16 of 105 mandibular premolars with radicular grooves. Most of the specimens had a triangle-shaped pulp chamber. Within this anatomic configuration, complexities of the root canal systems such as the presence of furcation canals, fusion of canals, oval-shaped canals in the apical third, small orifices at the pulp chamber level, and apical delta were also observed. (J Endod 2013;■:1–6)
The knowledge of root canal anatomy and its variations is a prerequisite for successful endodontic treatment. The presence of additional canals or deviations of the main root canals need to be recognized to avoid incomplete instrumentation and maintenance of etiologic factors involved in apical periodontitis.
Usually, teeth with single roots present single canals as in mandibular canines and maxillary anterior teeth. However, 2 root canals in single-rooted teeth may be present in mandibular incisors and premolars. In mandibular premolars, radicular grooves in the proximal aspects of the root are commonly associated with the presence of additional canals. A Vertucci type V configuration, in which one canal divides into two at the cervical or middle third, appears to be one of the most frequent anatomic variations in the mandibular premolar teeth. Nevertheless, reports on the presence of C-shaped or multiple canals can also be found in the literature.
Root canal anatomy has been evaluated by using clearing techniques, longitudinal and transverse cross-sectioning, and scanning electron microscope. However, these methods are invasive and therefore cannot accurately reflect the complete morphology of the object being studied. In recent years, micro–computed tomography (micro-CT) has gained increasing significance in the study of hard tissues in endodontics because it offers a reproducible technique that can be applied quantitatively as well as qualitatively for 3-dimensional (3D) assessment of the root canal system.
In mandibular premolars, the occurrence of a main canal that divided into 3 root canals at the middle or apical third, the so-called type IX configuration, is a rarely reported condition. To date, the literature lacks a detailed description of this anatomic variation. Thus, the aim of this study was to describe the morphometric aspects of the external and internal anatomy of mandibular premolars with type IX configuration by using micro-CT.
Materials and Methods
After ethics committee approval (Protocol #131-2010), a total of 105 extracted mandibular premolars with radicular grooves were selected. The patient gender and age were unknown. The samples were mounted on a custom attachment and scanned in a micro-CT system (SkyScan 1174v2; Bruker-microCT, Kontich, Belgium) by using 50 kV, 800 mA, and an isotropic resolution of 18 mm. Images of each specimen were reconstructed with dedicated software (NRecon v.1.6.3; Bruker-microCT) providing axial cross sections of the inner structure of the samples. 3D models were reconstructed from the source images by using automatic segmentation and surface modeling with CTAn v.1.12 software (Bruker-microCT). CTVol v.2.2.1 software (Bruker-microCT) was used for visualization and qualitative evaluation of the specimens regarding the presence of a type IX configuration of the root canal. From the initial sample, 16 mandibular premolars that met this criterion (15.2%) were analyzed.
DataViewer v.1.4.4 software (Bruker-microCT) was used to evaluate the number and location of root canals, the presence of apical delta, the configuration of the root canal orifices, and the distances between anatomic landmarks. ImageJ v.1.46 software (National Institutes of Health, Bethesda, MD) was used to measure the distances and angulations between the orifices at the division level of the main root canal. CTAn v.1.12 software was used for the 2-dimensional (2D) (area, perimeter, roundness, major diameter, and minor diameter) and 3D (volume, surface area, and structure model index [SMI]) evaluations of the root canal system.
2D evaluation was performed at the main root canal division level and 1 mm short from the apical foramen. Area and perimeter were calculated by using the Pratt algorithm. The cross-sectional appearance, round or more ribbon-shaped, was expressed as roundness. Roundness of a discreet 2D object is defined as 4.A/(π.(dmax)2), where A is the area and dmax is the major diameter. The value of roundness ranges from 0–1, with 1 meaning the perfect circle. The major diameter was defined as the distance between the 2 most distant pixels in that object. The minor diameter was defined as longest chord through the object that can be drawn in the direction orthogonal to that of the major diameter. Volume was calculated as the volume of binarized objects within the volume of interest. For the measurement of the surface area of the 3D multilayer dataset, 2 components to surface measured in 2 dimensions were used: first, the perimeters of the binarized objects on each cross-sectional level, and second, the vertical surfaces exposed by pixel differences between adjacent cross sections. SMI involves a measurement of surface convexity in a 3D structure. SMI is derived as 6.(S’.V)/S2, where S is the object surface area before dilation, S’ is the change in surface area caused by dilation, and V is the initial, undilated object volume. An ideal plate, cylinder, and sphere have SMI values of 0, 3, and 4, respectively.
The results of 2D and 3D analysis as well as the distances between the anatomic landmarks were described as mean, standard deviation, and range. Because normality assumptions could be verified (Shapiro-Wilk test, P > .05), data from the 3D and pulp chamber floor analysis were statistically compared by using analysis of variance post hoc Tukey test. Data from the 2D analysis were not normally distributed (Shapiro-Wilk test, P < .05), and Kruskal-Wallis post hoc Dunn test was used. The statistical analysis was performed by using SPSS v17.0 for Windows (SPSS Inc, Chicago, IL), with a significance level set at 5%.
Results
Qualitative Analysis
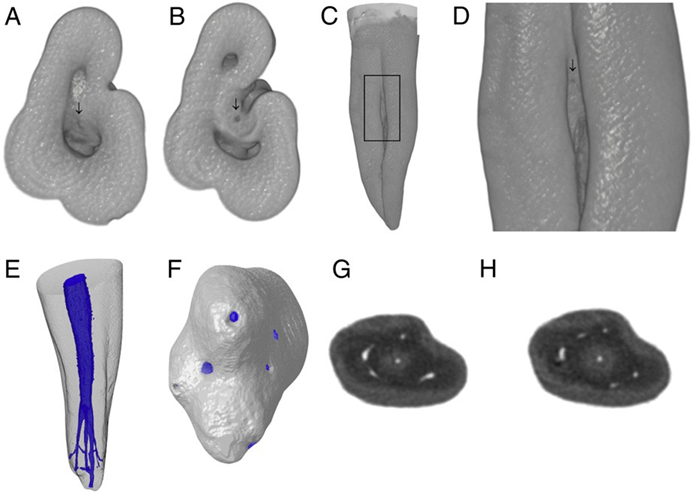
The analysis of the external anatomy showed that most of the specimens had only 1 root (n = 9) with radicular grooves in its buccal (Fig. 1A) and proximal (Fig. 1B) aspects. In 3 teeth, divisions of the main root into mesial and distal roots at the middle third level, with fusion at the apical level, were observed (Fig. 1C). In other 3 specimens this division occurred at the apical third on the buccal aspect of the root. Only 1 tooth had 3 independent roots (Fig. 1D). Mesiobuccal (MB), distobuccal (DB), and lingual (L) canals were observed in 15 teeth (Fig. 1E), and 1 specimen had 1 buccal and 2 lingual (mesiolingual and distolingual) canals (Fig. 1F). Furcation canals (Fig. 2A–D) and apical delta (Fig. 2E–H) were observed in 10 and 4 teeth, respectively.
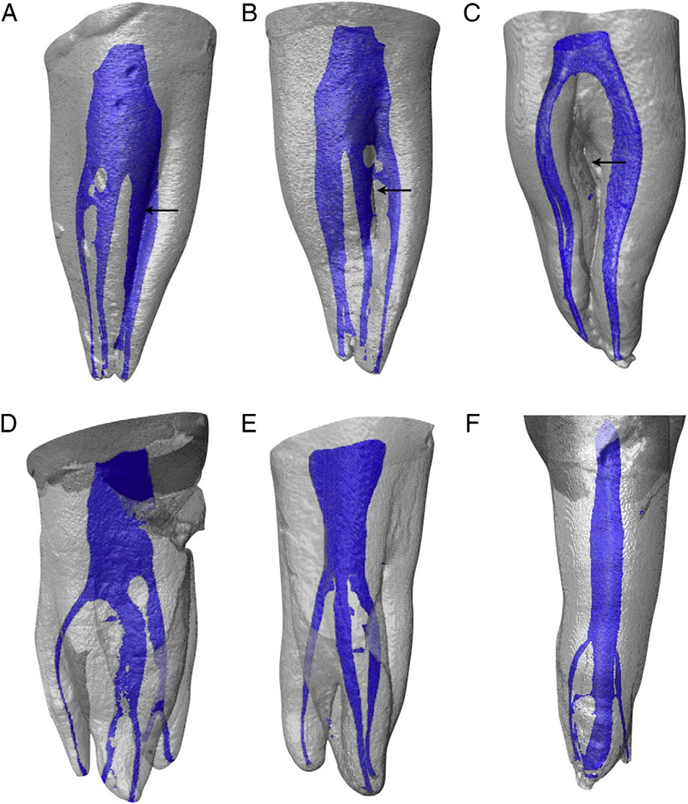
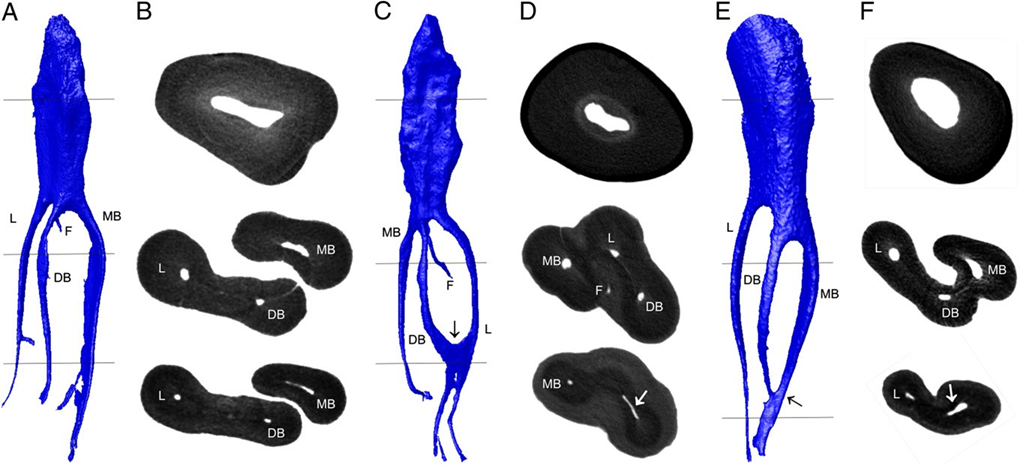
3D models confirmed the presence of a type IX configuration of the root canal system in 16 mandibular premolars (Fig. 3A and B). From the buccal view, superimposition of one of the distinct buccal canals with the lingual canal was observed in some teeth. At the apical third, fusion of the DB and L canals (Fig. 3C and D) as well as MB and DB canals (Fig. 3E and F) were observed in 3 and 2 teeth, respectively.
main root canal into 3 separated canals at the middle third; (C and D) fusion of DB and L canals at the apical third (arrow); (E and F) fusion of MB and DB canals at
the apical third (arrow). F, furcation canal.
Quantitative Analysis
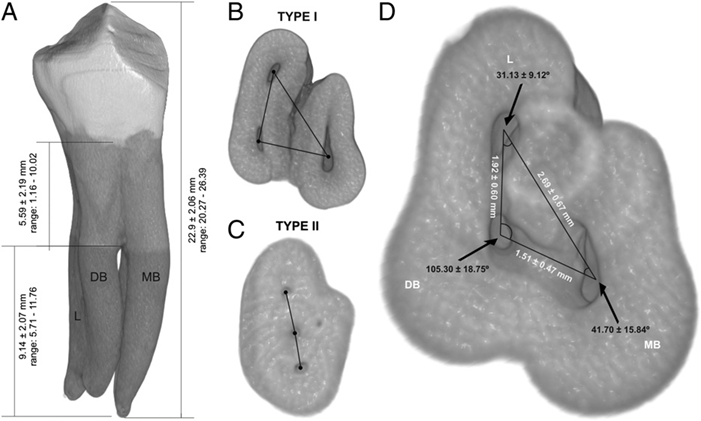
Mean distances (± standard deviation) and range between anatomic landmarks are shown in Figure 4A.
The spatial configurations of the orifices in relation to the pulp chamber floor were classified as type I (triangle-shaped, n = 15) (Fig. 4B) and type II (linear-shaped, n = 1) (Fig. 4C). Mean distances between MB and L canals were significantly higher than the DB to L or DB to MB distances (P < .05), which did not show statistical differences between them (P > .05). Consequently, the angle formed at the DB vertex was higher than those formed at the MB or L vertices, respectively (P < .05) (Fig. 4D).
Overall, mean volume, surface area, and SMI of the root canal system were 2.19 ± 1.51 mm3, 32.46 ± 16.94 mm2, and 2.28 ± 0.37, respectively. 3D analysis of MB, DB, and L canals was per- formed in teeth that did not present fusion of root canals at the apical third (n = 10). No statistical difference was observed in the comparison of volume, surface area, and SMI values between MB (1.05 mm3, 12.52 mm2, and 2.31, respectively), DB (0.45 mm3, 7.87 mm2, and 2.28, respectively), and L (0.59 mm3, 9.24 mm2, and 2.50, respectively) root canals (Table 1) (P > .05).

Data from 2D analysis of the MB, DB, and L canals are presented in Table 2. No statistical difference was found in the comparison of area, perimeter, roundness, and major and minor diameter values at the main root canal division level or at 1 mm short from the apical foramen between MB, DB, and L canals (P > .05). One of the specimens that had 1 buccal and 2 lingual canals (Fig. 1F) was not included in this analysis.

Discussion
Root canal anatomy can vary in the number of roots and root canals. In the endodontic literature, several variations in root canal anatomy of mandibular premolars have been reported. In laboratory-based studies, the presence of additional canals in mandibular premolars ranged from 18% to 32%. Recently, an in vivo cone-beam computed tomography study in a western Chinese population has shown that 11.8% of the mandibular premolars had multiple canals. This wide range of results in the prevalence of canal configurations in mandibular premolars in the literature has been explained by racial differences.
In recent years, micro-CT has been used for the detailed study of the anatomic variations of the root canal systems including mandibular premolar teeth. In this group of teeth, most researchers have reported the presence of C-shaped canals; however, except for case reports, only one previous study that used micro-CT reported the presence of a type IX anatomic configuration of the root canal system in mandibular premolars. In the cited study, the evaluation of the internal anatomy of 115 mandibular first premolars showed that 7.8% of the sample had this type of root canal configuration. In the present study, the higher percentage of type IX configuration (16%) found in the analyzed sample may be explained because only mandibular premolars with radicular grooves were selected, which increased the chance for selecting teeth with multiple canals. Although the presence of 3 root canals in mandibular premolars has been rarely reported in comparison to the Vertucci type V configuration, clinicians must be aware of this anatomic variation. According to a previous report, the characteristic of mandibular premolar with 3 root canals is the presence of a triangle-shaped pulp chamber in which the distance from the mesiobuccal to the lingual orifices was the highest. It is suggested that this geometric configuration could help in the latter localization of the DB canal. However, despite the fact that the triangle-shaped configuration of the orifices was found in most of the sample (n = 15), a linear configuration was also observed in one sample (Fig. 4).
The mean length of the mandibular premolars was 22.87 ± 2.06 mm. Woelfel studied 238 first and 227 second single- rooted mandibular premolars and found an average length of 22.4 mm (range, 17.0–28.5 mm) and 22.1 mm (range, 16.8– 28.1 mm), respectively, which is in accordance with the present results and similar to a previous report.
The furcation was mostly located at the middle third, and its distance to the cementoenamel junction (CEJ) and the apex ranged from 1.16–10.02 mm and from 5.71–11.76 mm, respectively. Clinically, considering that the mean distance of the pulp chamber floor to CEJ was 5.5 mm, the risk of perforation during access cavity preparation is minimal. In addition, the furcation near the CEJ would allow for better visualization of the root canal orifices than in cases in which furcation is located more apically.
Because of the lack of similar reports on type IX configuration in mandibular premolars, comparisons regarding the distances between anatomic landmarks were made by using data from mandibular premolars with different canal configurations but presenting furcation area. These studies reported that the distance from the furcation to the CEJ and to the apex ranged from 4–13 mm and from 4.88–12.1 mm, respectively, which is in accordance with the present results. Furcation canals that extended from the pulp chamber to the radicular groove were observed in most of the sample (62%). This finding is consistent with previous reports that showed its presence in 2-rooted mandibular canines and premolars with radicular grooves. Clinically, furcation canals in necrotic mandibular premolars with radicular grooves have been associated with persistent periradicular disease.
2D data (area, perimeter, major and minor diameters) analysis of the root canal orifices at the pulp chamber level did not show statistical differences between the canals. Although these data are extremely critical for the root canal negotiation, no similar data could be found in the literature. Overall, orifices had an oval shape (roundness ranged from 0.48–0.54), with a mean minor diameter ranging from 0.24–0.37 mm. However, minimal values such as 0.10, 0.06, and 0.14 mm were also found in the MB, DB, and L canals, respectively. Clinically, if narrow root canals are present, clinicians must be aware of the size of the instrument to be used during root canal negotiation because of the risk of ledge. The combination of small orifice sizes and furcation at the apical third make the treatment of mandibular premolars with type IX configuration a real challenge.
Effective root canal debridement relies on accurate determination of the working length and adequate apical canal enlargement, which allow for better irrigation in the apical area, optimizing root canal disinfection. A previous study that used mandibular premolars with 2 canals reported a major diameter ranging from 0.20–0.60 mm and from 0.12–0.15 mm to the buccal and lingual root canals, respectively. However, because of differences in root canal configuration and sample size, reliable comparisons are not possible to be made with the present results. 2D data (area, perimeter, major and minor diameters) of the root canals 1 mm short of the apical foramen indicated that the debridement at this level could be improved with instruments up to an ISO size 40. However, root canal roundness (0.50–0.63) indicates an oval shape, which could compromise adequate cleaning and shaping, leaving untouched fins on the buccal and/or lingual aspects of the central canal area. A careful selection of instruments is also advisable because of the radicular grooves. In this way, using instruments with large tapers could lead to stripping or perforations of the root. Another important anatomic aspect observed in some teeth was the presence of fusion between the canals at the apical third, which stresses the use of additional disinfection supplements such as passive ultrasonic irrigation or negative apical pressure.
Algorithms used in micro-CT evaluation allow further measurement of basic geometrical parameters such as volume and surface area as well as additional descriptors of canal shape such as SMI. The SMI describes the plate-like or cylinder-like geometry of an object. This variable has been used to detail changes in trabecular microstructure in osteoporosis or other bone diseases, but it may also be used to assess root canal geometry. The SMI is determined by an infinitesimal enlargement of the surface, whereas the change in volume is related to changes of surface area, ie, to the convexity of the structure. If a perfect plate is enlarged, the surface area does not change, yielding an SMI of 0. However, if a rod is expanded, the surface area increases with the volume and the SMI is normed, so that perfect rods are assigned an SMI score of 3. In the present study, the mean SMI result indicates that the root canal system of all canals had a cylinder-like geometry. Nonetheless, the results of volume and surface area of the canals of mandibular premolar teeth with type IX configuration of root canals cannot be compared with others because there is no information on this subject in the literature to date. Thus, the clinical relevance of such findings is still to be determined.
Clinically, radiographs have been one of the most important tools for detecting anatomic variations of the teeth. In the present study, the presence of MB and DB canals in almost all specimens (n = 15) would allow at least the radiographic identification of 2 root canals. In this condition, there is the probability that one of the root canals might be left untreated, which could result in failure of the root canal treatment. Therefore, other diagnostic methods like cone-beam computed tomography, as well as the use of surgical operative microscope, could be useful in such conditions, supporting the clinicians with the diagnosis and treatment of mandibular premolars with 3 root canals. These diagnostic methods may help to evaluate the number and position of root canals as well as the presence of radicular grooves in both sagittal and axial planes. In addition, measurements of the distance between anatomic land- marks such as the distance from furcation to the CEJ or to the apex are also possible in several cone-beam software programs.
In summary, the reported data may help clinicians to a thorough understanding of the variations in root canal morphology of mandibular premolars with 3 root canals (type IX configuration) to overcome problems related to shaping and cleaning procedures.
Conclusions
Type IX configuration of the root canal system was found in 16 of 105 (15.2%) extracted mandibular premolars with radicular grooves. Most of the specimens had a triangle-shaped pulp chamber in which the distance between the MB and L canals was the largest. Within this anatomic configuration, complexities of the root canal systems such as the presence of furcation canals, fusion of canals, oval-shaped canals at the apical level, small orifices at the pulp chamber level, and apical delta were also observed.
Authors: Ronald Ordinola-Zapata, Clóvis Monteiro Bramante, Marcelo Haas Villas-Boas, Bruno Cavalini Cavenago, Marco Húngaro Duarte, Marco Aurélio Versiani
References:
- Vertucci FJ. Root canal anatomy of the human permanent teeth. Oral Surg Oral Med Oral Pathol 1984;58:589–99.
- Siqueira JF. Reaction of periradicular tissues to root canal treatment: benefits and drawbacks. Endod Topics 2005;10:123–47.
- Li X, Liu N, Ye L, et al. A micro-computed tomography study of the location and curvature of the lingual canal in the mandibular first premolar with two canals originating from a single canal. J Endod 2012;38:309–12.
- Vertucci FJ. Root canal morphology of mandibular premolars. J Am Dent Assoc 1978;97:47–50.
- Walker RT. Root canal anatomy of mandibular first premolars in a southern Chinese population. Endod Dent Traumatol 1988;4:226–8.
- Trope M, Elfenbein L, Tronstad L. Mandibular premolars with more than one root canal in different race groups. J Endod 1986;12:343–5.
- Yu X, Guo B, Li KZ, et al. Cone-beam computed tomography study of root and canal morphology of mandibular premolars in a western Chinese population. BMC Med Imaging 2012;12:18.
- England MC Jr, Hartwell GR, Lance JR. Detection and treatment of multiple canals in mandibular premolars. J Endod 1991;17:174–8.
- Velmurugan N, Sandhya R. Root canal morphology of mandibular first premolars in an Indian population: a laboratory study. Int Endod J 2009;42:54–8.
- Robinson S, Czerny C, Gahleitner A, et al. Dental CT evaluation of mandibular first premolar root configurations and canal variations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2002;93:328–32.
- Fan B, Yang J, Gutmann JL, Fan M. Root canal systems in mandibular first premolars with C-shaped root configurations: part I—microcomputed tomography mapping of the radicular groove and associated root canal cross-sections. J Endod 2008; 34:1337–41.
- Simon JH, Dogan H, Ceresa LM, Silver GK. The radicular groove: its potential clinical significance. J Endod 2000;26:295–8.
- Liu N, Li X, Ye L, et al. A micro-computed tomography study of the root canal morphology of the mandibular first premolar in a population from southwestern China. Clin Oral Investig 2013;17:999–1007.
- Serman NJ, Hasselgren G. The radiographic incidence of multiple roots and canals in human mandibular premolars. Int Endod J 1992;25:234–7.
- Fan B, Ye W, Xie E, et al. Three-dimensional morphological analysis of C-shaped canals in mandibular first premolars in a Chinese population. Int Endod J 2012; 45:1035–41.
- Cleghorn BM, Christie WH, Dong CC. Anomalous mandibular premolars: a mandibular first premolar with three roots and a mandibular second premolar with a C-shaped canal system. Int Endod J 2008;41:1005–14.
- Wu MK, R’Oris A, Barkis D, Wesselink PR. Prevalence and extent of long oval canals in the apical third. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89: 739–43.
- Versiani MA, Pecora JD, Sousa-Neto MD. The anatomy of two-rooted mandibular canines determined using micro-computed tomography. Int Endod J 2011;44: 682–7.
- Peters OA, Laib A, Ruegsegger P, Barbakow F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J Dent Res 2000;79: 1405–9.
- Versiani MA, Pecora JD, de Sousa-Neto MD. Root and root canal morphology of four-rooted maxillary second molars: a micro-computed tomography study. J Endod 2012;38:977–82.
- Sert S, Bayirli GS. Evaluation of the root canal configurations of the mandibular and maxillary permanent teeth by gender in the Turkish population. J Endod 2004;30: 391–8.
- Hulsmann M. Mandibular first premolar with three root canals. Endod Dent Traumatol 1990;6:189–91.
- Chan K, Yew SC, Chao SY. Mandibular premolar with three root canals: two case reports. Int Endod J 1992;25:261–4.
- Nallapati S. Three canal mandibular first and second premolars: a treatment approach. J Endod 2005;31:474–6.
- ElDeeb ME. Three root canals in mandibular second premolars: literature review and a case report. J Endod 1982;8:376–7.
- Rodig T, Hulsmann M. Diagnosis and root canal treatment of a mandibular second premolar with three root canals. Int Endod J 2003;36:912–9.
- Woelfel S. Woelfel’s Dental Anatomy. 8th ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins Health; 2012.
- Fornari VJ, Silva-Sousa YT, Vanni JR, et al. Histological evaluation of the effectiveness of increased apical enlargement for cleaning the apical third of curved canals. Int Endod J 2010;43:988–94.
- Versiani MA, Pecora JD, de Sousa-Neto MD. Flat-oval root canal preparation with self-adjusting file instrument: a micro-computed tomography study. J Endod 2011;37:1002–7.
- Burleson A, Nusstein J, Reader A, Beck M. The in vivo evaluation of hand/rotary/ ultrasound instrumentation in necrotic, human mandibular molars. J Endod 2007;33:782–7.
- Susin L, Liu Y, Yoon JC, et al. Canal and isthmus debridement efficacies of two irrigant agitation techniques in a closed system. Int Endod J 2010;43:1077–90.
- Hildebrand T, Ruegsegger P. Quantification of bone microarchitecture with the structure model index. Comput Methods Biomech Biomed Engin 1997;1:15–23.
- Zhang R, Wang H, Tian YY, et al. Use of cone-beam computed tomography to evaluate root and canal morphology of mandibular molars in Chinese individuals. Int Endod J 2011;44:990–9.
- Tzanetakis GN, Lagoudakos TA, Kontakiotis EG. Endodontic treatment of a mandibular second premolar with four canals using operating microscope. J Endod 2007;33:318–21.
/public-service/media/default/158/GMj69_65311b2333f75.jpg)
/public-service/media/default/148/ix2WY_6531196adc6ec.jpg)
/public-service/media/default/145/GbhGY_65311921a3b65.jpg)
/public-service/media/default/147/bjsSM_65311952dfadf.jpg)