
Micro-CT evaluation of root filling quality in oval-shaped canals
Abstract
Aim: To assess the percentage volumes of filling materials and voids in oval-shaped canals filled with either cold lateral compaction or warm compaction techniques, using micro-computed tomography (micro-CT).
Methodology: Twenty-four single-rooted maxillary premolar teeth with oval-shaped canals were selected and the root canals prepared and assigned to two groups (n = 12), according to the filling technique: cold lateral compaction (CLC) or warm vertical compaction (WVC). Each specimen was scanned using a micro-CT device at an isotropic resolution of 12.5 μm. Percentage volumes of root filling materials and voids were calculated, and data were statistically analysed using Student’s t-test and Friedman’s test, with a significance level of 5%.
Results: Overall, mean percentage volumes of gutta-percha, sealer and voids were 82.33 ± 3.14, 13.42 ± 2.91 and 4.26 ± 0.74 in the CLC group and 91.73 ± 4.48, 7.70 ± 4.44 and 0.57 ± 0.44 in the WVC group, respectively, with a statistically significant difference between groups (P < 0.05). At the apical level, differences in the percentage volumes of filling materials and voids between groups were not significant (P > 0.05).
Conclusions: No root fillings were void free. Warm vertical compaction produced a significantly greater volume of gutta-percha and a significantly lower percentage of voids than those achieved with cold lateral compaction. Distribution of sealer and voids within the root canal space after root filling was unpredictable, irrespective of the technique used.
Introduction
The primary goals of root canal treatment are to debride and disinfect the root canal space to the greatest possible extent, and to seal the canals as effectively as possible, aiming to establish or maintain healthy periapical tissues (Whitworth 2005). The methods and materials used for filling root canals are numerous (Leduc & Fishelberg 2003, Flores et al. 2011, Borges et al. 2012). Conventional root fillings consist of a core material, usually gutta-percha, that should be closely adapted to the canal wall, and cement that seals the interface between the core and the dentine (Schilder 1967, Leduc & Fishelberg 2003, Mirfendereski et al. 2009).
Cold lateral compaction is the most commonly taught and practised filling technique worldwide (Leduc & Fishelberg 2003) and is regarded as the standard against which other filling techniques must be evaluated (Whitworth 2005, De-Deus et al. 2008b). Despite being predictable and relatively simple to execute in regularly tapered canals, root fillings when placed using a lateral compaction technique might lack homogeneity and thus result in a great amount of sealer (De-Deus et al. 2008a). Areas filled by sealer are more vulnerable because sealers may dissolve over time (Versiani et al. 2006, Flores et al. 2011, Borges et al. 2012) and leakage may occur. In an attempt to overcome that shortcoming, warm compaction techniques were developed (Schilder 1967). Generally, these techniques consist of filling the root canal space with thermoplasticized gutta-percha and a thin layer of sealer; subsequently, a cold plugger is used to apically condense the filling material in the canal (De-Deus et al. 2008b, Angerame et al. 2012). As gutta-percha is heated, it becomes more plastic and will adapt to irregularities and ecesses, especially in oval-shaped root canals (De-Deus et al. 2008b). However, the thermoplasticized gutta-percha techniques also have disadvantages. As gutta-percha is heated, it expands, and during cooling, it contracts (1–2%), which may result in voids and gaps along the root filling (Peng et al. 2007, Moeller et al. 2013).
In many studies, the percentage of gutta-percha filled area has been used (Wu et al. 2002, Van der Sluis et al. 2005, De-Deus et al. 2008a,b) as a surrogate measure of the quality of the root filling (Wolf et al. 2014). Most of these procedures allow only partial evaluation of root fillings and some may create irreversible damage to the specimens (Wu et al. 2002, Van der Sluis et al. 2005, De-Deus et al. 2008a,b, Mirfendereski et al. 2009, Souza et al. 2009). These might lead to inaccuracies because some filling material might be lost during sample preparation (Mirfendereski et al. 2009). Thus, an ideal experimental model should allow the preservation of sample integrity to avoid irreversible structural damage (Somma et al. 2011, Versiani et al. 2013a,b). In the last decade, nondestructive micro-computed tomography (micro-CT) technology has emerged as an important imaging tool to evaluate root fillings (Jung et al. 2005, Phides & Hoshino 2008, Hammad et al. 2009, Mirfendereski et al. 2009, Metzger et al. 2010, Somma et al. 2011, Zaslansky et al. 2011, Zogheib et al. 2011, 2013, Angerame et al. 2012, El-Ma’aita et al. 2012, Moeller et al. 2013, Naseri et al. 2013, Wolf et al. 2014), overcoming some limitations of the former studies (Mirfendereski et al. 2009).
Considering that three-dimensional distribution of voids is important to understand how different filling procedures impact on material distribution and voids within the root canal, the purpose of this ex vivo study was to assess the percentage volume of filling materials and voids in oval-shaped canals filled with either cold lateral compaction or warm vertical compaction techniques, using micro-CT analysis. The null hypothesis tested was that there was no significant difference in the percentage volume of the filling materials and voids produced by these techniques.
Materials and methods
Sample size calculation
Total sample size for this study was calculated after the effect size estimation of the percentage of voids and gaps promoted by cold lateral compaction using a micro-CT approach, as reported by Hammad et al. (2009). From 12 samples used in each group, the authors reported that the percentage of voids and gaps ranged from 1.02 ± 0.14 (control group) to 4.28 ± 1.44 (experimental group). Following the t-test family and difference between two independent means (G*Power 3.1.7 for Windows, Heinrich Heine, Universität Düsseldorf), a calculated effect size of 3.07 was inputted. Alpha-type error by 0.05 and power beta of 0.95 were also specified. Based on these parameters, a total of 10 samples was indicated as the minimum ideal size required to observe this same effect.
Sample selection
This study was approved by the local ethics committee (protocol 218/2012). One hundred straight single-rooted human maxillary premolars with fully formed apices, extracted for periodontal or orthodontic reasons, were obtained from a pool of teeth and decoronated. The patient’s gender and age were unknown. Preliminary periapical radiographs were taken in both bucco-lingual and mesio-distal directions for each tooth. All teeth with more than one root canal, isthmus, resorption, calcifications or apical curvature were excluded. To attain an overall outline of internal anatomy as well as the calculation of volume and surface area of the root canals, these teeth were pre-scanned at a relatively low resolution of 68 μm using a micro-CT scanner (SkyScan 1172; Bruker-microCT, Kontich, Belgium) at 90 kV and 112 μA. Axial cross-sections of the inner structure of the samples were acquired after reconstruction procedures (NRecon version 1.6.3 software; Bruker-microCT). Based on a slice-by-slice assessment, the slices at 5 and 8 mm, taking the root apex as a reference point, were determined and the root canal outlined. The minimum and maximum diameters of the root canal at these levels were measured using DataViewer version 1.4.4 software (Brucker-microCT). Based on these pre-scan set of images, 24 teeth with a canal ratio of long to short diameter of more than 2, at the 5-mm level, and 3, at the 8-mm level, were selected and stored in 0.1% thymol solution at 5 °C.
The specimens were then pair-matched based on the length, volume and surface area of the root canals. One specimen from each pair was randomly assigned to one of the two experimental groups (n = 12). After checking for normality assumption (Shapiro–Wilk test), the degree of homogeneity (base- line) of the two groups, with respect to the length, volume and surface area of the root canal, was con- firmed using the Student’s t-test, with a confidence level set at 5%.
Root canal preparation
After being washed in running water for 24 h, conventional access cavities were prepared. Apical patency was confirmed by inserting a size 10K-file through the apical foramen before and after completion of root canal preparation. Working length (WL) was established at 1 mm from canal length, and a single experienced operator performed all canal preparations. Then, root canals were serially enlarged with Revo-S NiTi rotary instruments (Micro-Mega, Besanc on, France) driven by a torque-controlled motor (W&H, Bürmoos, Austria) set to 300 rpm using a gentle in-and-out motion. This system is composed of two instruments for shaping and cleaning procedures (SC1 and SC2) and one finishing instrument (SU). These instruments were used in a crown-down manner up to the WL, resulting in an apical third shaped to a size 25, 0.06 taper. Then, the sequence was completed using the Apical Shaper instruments (AS30, AS35 and AS40, tapered at 0.06) up to the WL. Apical enlargement was performed using a size 45 manual K-file (Mani Co, Tokyo, Japan). Two canals were prepared with one set of Revo-S NiTi rotary instruments. The instruments were withdrawn when resistance was felt and changed for the next instrument. During the preparation procedure, the canals were flushed with 2 mL of 5% NaOCl between each instrument, delivered in a syringe with a 30-gauge needle placed 1 mm short of the WL. After preparation, a final rinse with 2 mL of saline solution was performed and the root canals were dried with paper points.
Root canal filling
A flip of a coin was used to define which of the experimental groups (n = 12) would be treated with each of the following filling techniques: cold lateral compaction (CLC) or warm vertical compaction (WVC). AH Plus sealer (Dentsply De Trey GmbH, Konstanz, Germany) was prepared according to manufacturer’s instruction, and a total volume of 14 mm3 was introduced into each root canal using a size 40, 0.02 taper manual file (Mani Inc., Tochigi, Japan).
In the CLC group, a pre-fitted size 45, 0.02 taper gutta-percha cone (Diadent Group International, Chongchong Buk Do, Korea) was inserted to full working length. Lateral compaction was achieved using size F accessory gutta-percha cones (Diadent Group International) until a size 25 finger spreader (VDW, Antaeos, Munich, Germany) could penetrate no more than 3 mm into the canal. A heated instrument was used to section the coronal surplus, after which the filling was vertically compacted. In the WVC group, thermoplasticized gutta-percha was injected into the canal in small increments using the Dia-Gun Obturation System (North Fraser Way, Burnaby, BC, Canada). Pressure with a plugger of adequate size (Medesy SRL, Maniago, Italy) was performed to compact the gutta-percha. The specimens were radiographed in the both bucco-lingual and mesio-distal directions to confirm the adequacy of the filling and then stored (37 °C, 100% humidity) for 3 weeks to allow the complete setting of the sealer. If voids were observed in the root filling, the specimen was replaced.
Micro-CT analysis
Each tooth was slightly dried and mounted on a custom attachment, and the analysis of the filling materials was undertaken using a micro-CT system (SkyScan 1172; Bruker-microCT). The roots were scanned at 90 kV, 112 μA and an isotropic pixel size of 12.5 μm, which resulted in 900–1100 transverse cross-sections per specimen. Scanning was performed by 180° rotation around the vertical axis, camera exposure time of 2600 ms, rotation step of 0.6° and frame averaging of 2, applying medium filtering of the data. X-rays were fil- tered with 500-μm aluminium and a 38-μm-thick copper filter. A flat-field correction was taken on the day, prior to scanning, to correct for variations in the pixel sensitivity of the camera. Axial cross-sections of the inner structure of the samples were reconstructed using NRecon version 1.6.3 (Bruker-microCT) with a beam hardening correction of 15%, smoothing of three and an attenuation coefficient range of —0.002 to 0.15.
For the calculation of the volume and surface representations of the filling materials, the original grey-scale images were processed with a slight Gaussian low-pass filtration for noise reduction and an automatic segmentation threshold was used to separate root dentine from gutta-percha, sealer and voids, using CTAn version 1.12 software (Bruker-microCT). This process entails choosing the range of grey levels for each filling material, dentine or void, necessary to obtain an image composed only of black and white pixels. The high contrast of the filling materials compared with the dentine yielded excellent segmentation of the specimens. Separately and for each slice, regions of interest were chosen to allow the calculation of the volume (in mm3) of the filling materials and the voids. Polygonal surface representations of dentine, gutta-percha, sealer and voids were constructed in CTAn version 1.12 software (Bruker-microCT) and qualitatively evaluated using CTVol version 2.2.1 software (Bruker-microCT). In this study, considering that it was not possible to distinguish voids, gaps and spreader tracts from the micro-CT images, all areas without filling material within the root canal space after the filling procedures were considered as voids. Lateral or accessory canals were not considered in the analysis.
Statistical analysis
The volume of gutta-percha, sealer and voids was expressed as the percentage of the root canal volume after shaping and cleaning procedures. The total root canal volume was considered as the sum of volumes previously calculated for the filling materials and voids. The Shapiro–Wilk and Levene’s tests were used to test the assumption of normality and the equality of variance among the datasets, respectively, which were presented as percentage means and standard deviations. Data were normally distributed between groups (P > 0.05) and were compared statistically using the Student’s t-test. Within group, data were skewed (P < 0.05) and therefore compared using the Friedman’s test. The significance level was set at 5% (SPSS version 17.0 for Windows, SPSS Inc., Chicago, IL, USA).
Results
Mean percentage (standard deviation) and volume percentage range of the filling materials (gutta-percha and sealer) and voids are summarized in Table 1. Overall, distribution of sealer and voids within the root canal space after filling procedures was unpredictable, irrespective of the root filling method.
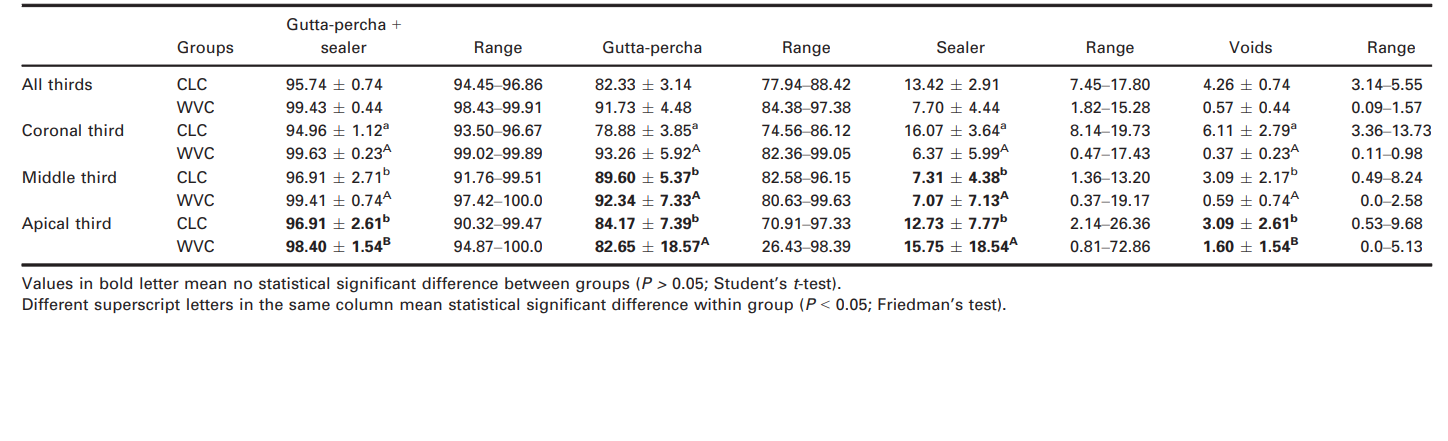
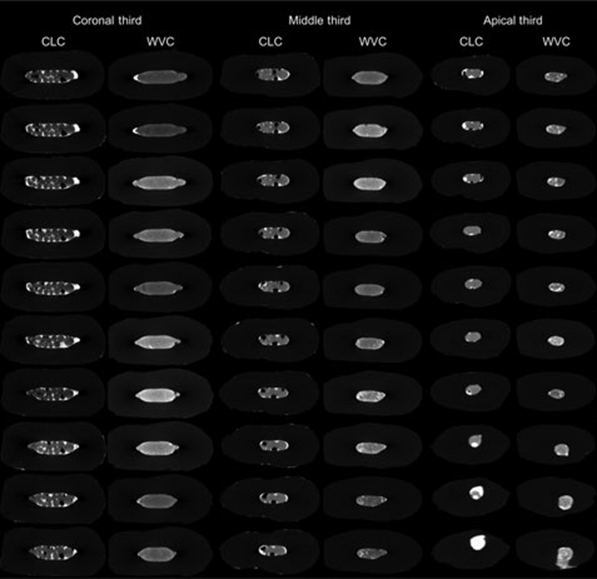
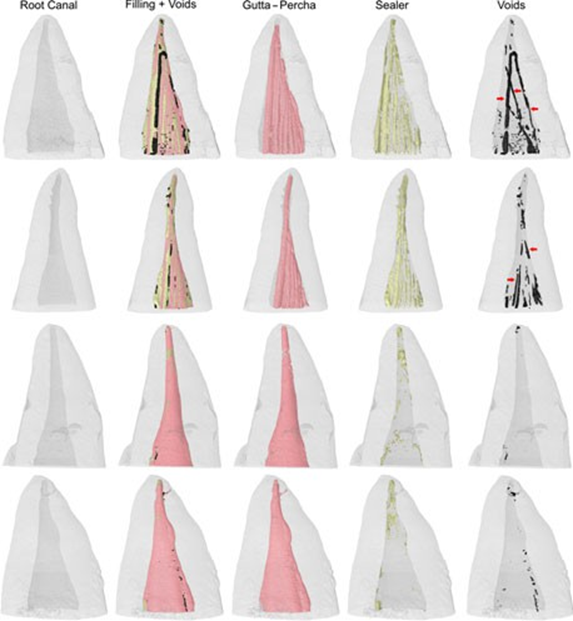
The WVC group had greater percentage volumes of filling materials than the CLC group (P < 0.05). None of the filling techniques was able to completely fill the root canal space; in the WVC group, a significantly lower percentage volume range of voids (0.09–1.57) was observed (P < 0.05). Figures 1 and 2 show the greatest amount of voids and sealer throughout the root canal in the CLC group, while in the WVC group, gutta-percha filled almost all the root canal space. In the CLC group, several gutta-percha cones were observed tightly pressed together with sealer, which remained in direct contact with the dentine. The presence of spreader tracts devoid of sealer was also observed. In the WVC group, the plasticized solid filling material penetrated into the sealer, forming a non-uniform structure with fewer voids and improved adaptation to the canal walls (Fig. 2).
The analysis of the canal thirds showed that the WVC group had a significantly smaller void volume than CLC group in the coronal and middle thirds (P < 0.05). No statistical difference between groups was observed in the volume of gutta-percha and sealer in the middle level (P > 0.05). At the apical level, differences in the percentage volume of filling materials and voids between groups were not significant (P > 0.05). Within group, percentage volume of voids in the apical third was significantly higher than in the middle and coronal thirds in the WVC group (P < 0.05); in contrast, CLC group had more voids in the coronal level compared to the apical third (P < 0.05).
Discussion
Considering that the overall distribution of the filling materials and voids within the root canal space was significantly different in the comparison between CLC and WVC techniques, the null hypothesis was rejected. However, despite the WVC technique resulting in denser root fillings, neither of the techniques provided a void-free root filling, corroborating previous studies using either conventional (Wu et al. 2002, De-Deus et al. 2008a,b) or micro-CT methods (Hammad et al. 2009, Angerame et al. 2012, Moeller et al. 2013).
The incidence of voids within root fillings may be affected by many factors such as the anatomical configuration of the canal system, the quality of canal preparation, the consistency and volume of sealer, the operator’s expertise and the technique used. In previous studies, percentage volumes of voids analysed three-dimensionally in canals filled with CLC techniques using resin-based sealers were 4.10 ± 2.70 (EndoREZ) and 4.28 ± 1.44 (RealSeal) (Hammad et al. 2009), while percentage volumes with WVC techniques using AH Plus sealer were 0.70 ± 2.31 (Angerame et al. 2012) and 0.82 ± 2.53 (Somma et al. 2011). Despite differences in sample selection and scanning parameters, these results are in accordance with the present study in which the percentage of voids in the CLC group (4.26 ± 0.74) was significantly higher than in WVC groups (0.57 ± 0.44).
The presence of voids has been attributed to the fact that resin-based sealers undergo a polymerization shrinkage, which might lead to gap and void formation (Hammad et al. 2009, Zogheib et al. 2011, 2013, Wolf et al. 2014). Then, the greater thickness of sealer in the CLC group would explain the greater amount of voids compared to the WVC group. Nevertheless, considering that AH Plus has been proved to have an adequate dimensional stability (Versiani et al. 2006, Flores et al. 2011, Borges et al. 2012), it may be inferred that a greater amount of sealer might not be correlated with a higher percentage of voids. In Fig. 1, spreader tracts devoid of sealer can be observed in the CLC group. The spreaders tended to follow a straight line and left an indentation on the gutta-percha or created a space, which was either occupied by gutta-percha or sealer, or remained as a void. Therefore, the explanation for these results might be more associated with the presence of spreader tracts than with the incomplete adaptation of GP cones, lack of surface adaptation or sealer shrinkage, as previously hypothesized (Hammad et al. 2009, Zogheib et al. 2011, 2013, Wolf et al. 2014).
The analysis of the percentage volumes of voids and sealer in the canal thirds was associated with large standard deviation values in both groups, as previously observed (Hammad et al. 2009, Mirfendereski et al. 2009). In both groups, the greatest amount of sealer was observed in the apical third. In the CLC group, it may be explained because root canals tend towards a rounder cross-section at this level (Wu et al. 2002), favouring the adaptation of the master cone, limiting spreader penetration and, consequently, preventing accessory cones being inserted up to the WL. On the other hand, in the WVC group, the thicker sealer layer in this area appeared to reflect a suboptimal heat soft- ening of gutta-percha (Mirfendereski et al. 2009). It has been speculated that variations in the quality of the filling procedure could be inherent to all techniques independent of the degree of clinical experience (Mirfendereski et al. 2009). Actually, considering the results from previous 3D studies on root filling using micro-CT (Hammad et al. 2009, Mirfendereski et al. 2009, Metzger et al. 2010, Somma et al. 2011, Angerame et al. 2012), it seems that the distribution of sealer and voids within the root canal space is unpredictable, irrespective of the filling method.
Since the development of warm compaction techniques, there has been debate whether they are superior to CLC (Angerame et al. 2012). Although this study showed that canals filled with the WVC technique had less voids than the CLC technique, this is only one indicator for the assessment of the quality of root filling. Additionally, considering that the majority of epidemiological studies on the predictability of root canal treatment have included canal filling by CLC (Whitworth 2005, Peng et al. 2007), it may be hypothesized that there is a threshold of voids within root fillings below which a favourable host response is expected.
Conclusion
No filling technique produced void-free root canal fillings. Warm vertical compaction was associated with a lower percentage volume of voids than those achieved with cold lateral compaction. Distribution of sealer and voids within the root canal space after filling was unpredictable, irrespective of the root filling method.
Authors: A. Keleş, H. Alcin, A. Kamalak, M. A. Versiani
References:
- Angerame D, De Biasi M, Pecci R et al. (2012) Analysis of single point and continuous wave of condensation root filling techniques by micro-computed tomography. Annali dell’Istituto Superiore di Sanità 48, 35–41.
- Borges RP, Sousa-Neto MD, Versiani MA et al. (2012) Changes in the surface of four calcium silicate-containing endodontic materials and an epoxy resin-based sealer after a solubility test. International Endodontic Journal 45, 419– 28.
- De-Deus G, Murad C, Paciornik S, Reis CM, Coutinho-Filho T (2008a) The effect of the canal-filled area on the bacterial leakage of oval-shaped canals. International Endodontic Journal 41, 183–90.
- De-Deus G, Reis C, Beznos D, de Abranches AM, Coutinho-Filho T, Paciornik S (2008b) Limited ability of three commonly used thermoplasticized gutta-percha techniques in filling oval-shaped canals. Journal of Endodontics 34, 1401–5.
- El-Ma’aita AM, Qualtrough AJ, Watts DC (2012) A micro-computed tomography evaluation of mineral trioxide aggregate root canal fillings. Journal of Endodontics 38, 670–2.
- Flores DS, Rached-Júnior FJ, Versiani MA, Guedes DF, Sousa-Neto MD, Pécora JD (2011) Evaluation of physicochemical properties of four root canal sealers. International Endodontic Journal 44, 126–35.
- Hammad M, Qualtrough A, Silikas N (2009) Evaluation of root canal obturation: a three-dimensional in vitro study. Journal of Endodontics 35, 541–4.
- Jung M, Lommel D, Klimek J (2005) The imaging of root canal obturation using micro-CT. International Endodontic Journal 38, 617–26.
- Leduc J, Fishelberg G (2003) Endodontic obturation: a review. General Dentistry 51, 232–3.
- Metzger Z, Zary R, Cohen R, Teperovich E, Paqué F (2010) The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. Journal of Endodontics 36, 1569–73.
- Mirfendereski M, Roth K, Fan B et al. (2009) Technique acquisition in the use of two thermoplasticized root filling methods by inexperienced dental students: a microcomputed tomography analysis. Journal of Endodontics 35, 1512–7.
- Moeller L, Wenzel A, Wegge-Larsen AM, Ding M, Kirkevang LL (2013) Quality of root fillings performed with two root filling techniques. An in vitro study using micro-CT. Acta Odontologica Scandinavica 71, 689–96.
- Naseri M, Kangarlou A, Khavid A, Goodini M (2013) Evaluation of the quality of four root canal obturation techniques using micro-computed tomography. Iranian Endodontic Journal 8, 89–93.
- Peng L, Ye L, Tan H, Zhou X (2007) Outcome of root canal obturation by warm gutta-percha versus cold lateral condensation: a meta-analysis. Journal of Endodontics 33, 106–9.
- Phides NP, Hoshino E (2008) Evaluation of obturation by image analyses and macrogol and propylene glycol penetration . Journal of LSTR Therapy 7, 6–10.
- Schilder H (1967) Filling root canals in three dimensions. Dental Clinics of North America 11, 723–44.
- Somma F, Cretella G, Carotenuto M et al. (2011) Quality of thermoplasticized and single point root fillings assessed by micro-computed tomography. International Endodontic Journal 44, 362–9.
- Souza EM, Wu MK, van der Sluis LW, Leonardo RT, Bonetti-Filho I, Wesselink PR (2009) Effect of filling technique and root canal area on the percentage of gutta-percha in laterally compacted root fillings. International Endodontic Journal 42, 719–26.
- van der Sluis LW, Wu MK, Wesselink PR (2005) An evaluation of the quality of root fillings in mandibular incisors and maxillary and mandibular canines using different methodologies. Journal of Dentistry 33, 683–8.
- Versiani MA, Carvalho-Júnior JR, Padilha MI, Lacey S, Pascon EA, Sousa-Neto MD (2006) A comparative study of physicochemical properties of AH Plus and Epiphany root canal sealants. International Endodontic Journal 39, 464–71.
- Versiani MA, Pecora JD, Sousa-Neto MD (2013a) Microcomputed tomography analysis of the root canal morphology of single-rooted mandibular canines. International Endodontic Journal 46, 800–7.
- Versiani MA, Steier L, De-Deus G, Tassani S, Pécora JD, Sousa-Neto MD (2013b) Micro–computed tomography study of oval-shaped canals prepared with the Self-adjusting File, Reciproc, WaveOne, and Protaper Universal systems. Journal of Endodontics 39, 1060–6.
- Whitworth J (2005) Methods of filling root canals: principles and practices. Endodontic Topics 12, 2–24. Wolf M, Kupper K, Reimann S, Bourauel C, Frentzen M (2014) 3D analyses of interface voids in root canals filled with different sealer materials in combination with warm gutta-percha technique. Clinical Oral Investigations 18, 155–61.
- Wu MK, van der Sluis LW, Wesselink PR (2002) A preliminary study of the percentage of gutta-percha-filled area in the apical canal filled with vertically compacted warm gutta-percha. International Endodontic Journal 35, 527–35.
- Zaslansky P, Fratzl P, Rack A, Wu MK, Wesselink PR, Shemesh H (2011) Identification of root filling interfaces by microscopy and tomography methods. International Endodontic Journal 44, 395–401.
- Zogheib C, Naaman A, Medioni E, Arbab-Chirani R (2011) Influence of apical taper on the quality of thermoplasticized root fillings assessed by micro-computed tomography. Clinical Oral Investigations 16, 1493–8.
- Zogheib C, Naaman A, Sigurdsson A, Medioni E, Bourbouze G, Arbab-Chirani R (2013) Comparative micro-computed tomographic evaluation of two carrier-based obturation systems. Clinical Oral Investigations 17, 1879–83.